


Lateral epicondylitis results from inflammation and microtearing of fibers in the extensor tendons of the forearm. Symptoms include pain at the lateral epicondyle of the elbow, which can radiate into the forearm. Diagnosis is by examination and provocative testing. Treatment is with rest, nonsteroidal anti-inflammatory drugs (NSAIDs), and physical therapy.
Theories about the pathophysiology of lateral epicondylitis include nonathletic and occupational activities that require repetitive and forceful forearm supination and pronation, as well as overuse or weakness (or both) of the extensor carpi radialis brevis and longus muscles of the forearm, which originate from the lateral epicondyle of the elbow. For example, during a backhand return in racket sports such as tennis, the elbow and wrist are extended, and the extensor tendons, particularly the extensor carpi radialis brevis, can be damaged when they roll over the lateral epicondyle and radial head. Contributing factors include weak shoulder and wrist muscles, a racket strung too tightly, an undersized grip, hitting heavy wet balls, and hitting off-center on the racket.
In resistance trainees, injuries often are caused by overuse (too much activity or doing the same movements too often) or by muscle imbalance between the forearm extensors and flexors. Nonathletic activities that can cause or contribute to lateral epicondylitis include those involving repetitive grasping and twisting the elbow (eg, turning a screwdriver, perhaps typing).
With time, subperiosteal hemorrhage, calcification, spur formation on the lateral epicondyle, and, most importantly, tendon degeneration can occur.
Symptoms and Signs of Lateral Epicondylitis
Pain initially occurs in the extensor tendons of the forearm and around the lateral elbow when the wrist is extended against resistance (eg, as in using a manual screwdriver or hitting a backhand shot with a racket). In resistance trainees, lateral epicondylitis is most noticeable during various rowing and chin-up exercises for the back muscles, particularly when the hands are pronated. Pain can extend from the lateral epicondyle to the mid forearm.
Diagnosis of Lateral Epicondylitis
Provocative testing
Pain along the common extensor tendon when the long finger is extended against resistance and the elbow is held straight is diagnostic. Alternatively, the diagnosis is confirmed if the same pain occurs during the following maneuver: The patient sits on a chair with the forearm on the examination table and the elbow held flexed (bent) and the hand held palm downward; the examiner places a hand firmly on top of that of the patient, who tries to raise the hand by extending the wrist (see also How to Examine the Elbow).
Treatment of Lateral Epicondylitis
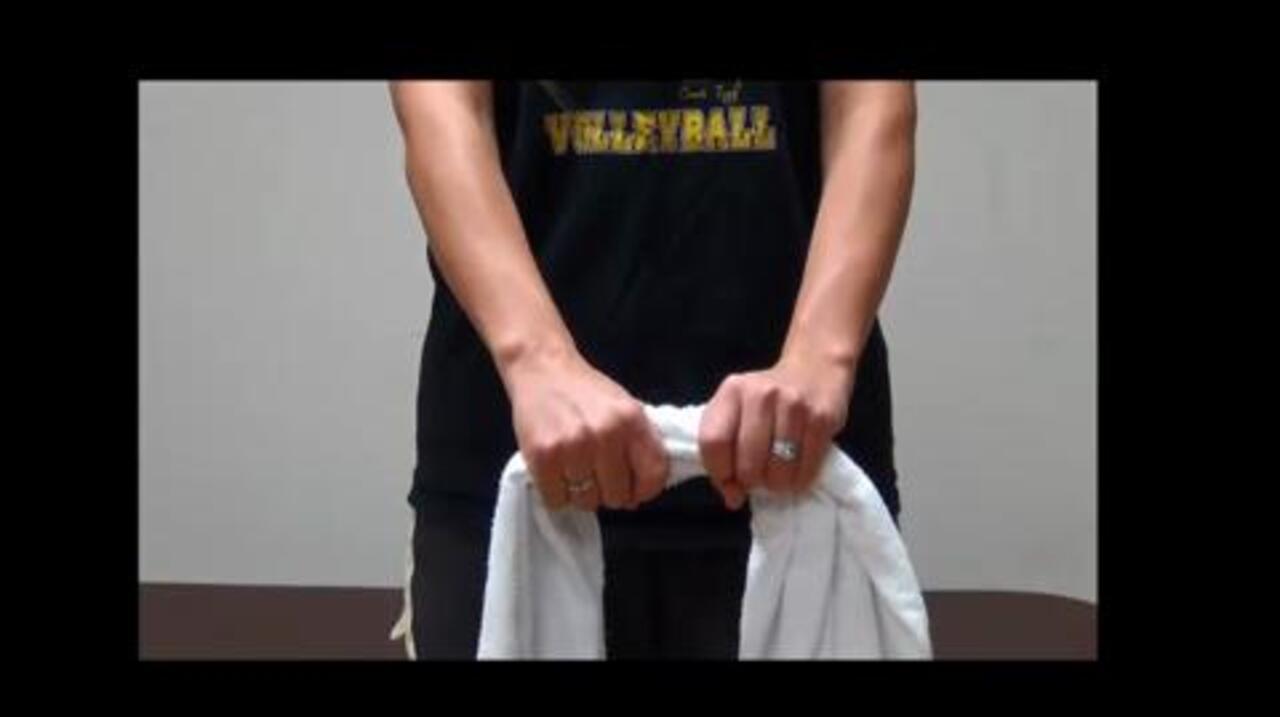
Rest, ice, nonsteroidal anti-inflammatory drugs (NSAIDs), extensor muscle stretches
Modification of activity
Tennis elbow (counterforce) brace
Later, resistive exercises
Treatment involves a 2-phased approach. Initially, rest, ice, NSAIDs, and stretching of the extensor muscles are used. Occasionally a corticosteroid injection into the painful area around the tendon is needed. When the pain subsides, gentle resistive exercises of the extensor and flexor muscles in the forearm are done followed by eccentric and concentric resistive exercises. Activity that hurts when the wrist is extended or supinated should be avoided. Use of a tennis elbow (counter force) brace is often advised. Adjusting the fit and type of racket used can also help prevent further injury.
Although surgery is not usually needed, surgical techniques to treat lateral epicondylitis involve removing scar and degenerative tissue from the involved extensor tendons at the elbow. Surgery is usually considered only after at least 9 to 12 months of unsuccessful conservative treatment; patients should be advised that surgery may not provide satisfactory relief of symptoms.

Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.


Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.
Key Points
Lateral epicondylitis can result from repetitive and forceful forearm supination and pronation, and/or extension of the forearm and wrist; such motions involve the extensor carpi radialis brevis and longus muscles of the forearm, which originate from the lateral epicondyle of the elbow.
Typical activities that involve such motions include a backhand return in racket sports (eg, tennis) and using a screwdriver.
Pain along the common extensor tendon when the long finger is extended against resistance and the elbow is held straight is diagnostic.
Treat initially with rest, ice, NSAIDs, and stretching of the extensor muscles, followed by exercises to strengthen wrist extensors and flexors.
Sometimes corticosteroid injections and rarely surgery may help.






