


Parasitic helminthic worms infect the central nervous system (CNS) of millions of people in developing countries. Infected people who visit or immigrate to nonendemic areas, including the US, may present there. Worms may cause meningitis, encephalitis, cerebral masses, hydrocephalus, stroke, and myelopathy.
(See also Introduction to Brain Infections.)
Neurocysticercosis
(See also Cysticercosis.)
Among about 20 helminths that can cause neurologic disorders, the pork tapeworm Taenia solium causes by far the most cases in the Western Hemisphere. The resulting disorder is neurocysticercosis. After a person eats food contaminated with the worm’s eggs, larvae migrate to tissues, including the brain, spinal cord, and cerebrospinal fluid (CSF) pathways, and form cysts. Cyst diameter rarely exceeds 1 cm in neural parenchyma but may exceed 5 cm in CSF spaces. Older cysts frequently calcify.
Brain parenchymal cysts cause few symptoms until death of the worms triggers local inflammation, gliosis, and edema, causing seizures (most commonly), cognitive or focal neurologic deficits, or personality changes. Larger cysts in CSF pathways may cause obstructive hydrocephalus. Cysts may rupture into CSF, inducing acute or subacute eosinophilic meningitis. Without treatment, neurocysticercosis can cause death; cause of death includes encephalitis, meningitis, hydrocephalus, and untreated seizures.
Neurocysticercosis is suspected in patients who live in or have come from developing countries and who have eosinophilic meningitis or unexplained seizures, cognitive or focal deficits, or personality changes. It is suggested by multiple calcified cystic lesions seen on CT or MRI; a contrast agent may enhance the lesions. Diagnosis requires serum and CSF serologic tests and occasionally cyst biopsy.

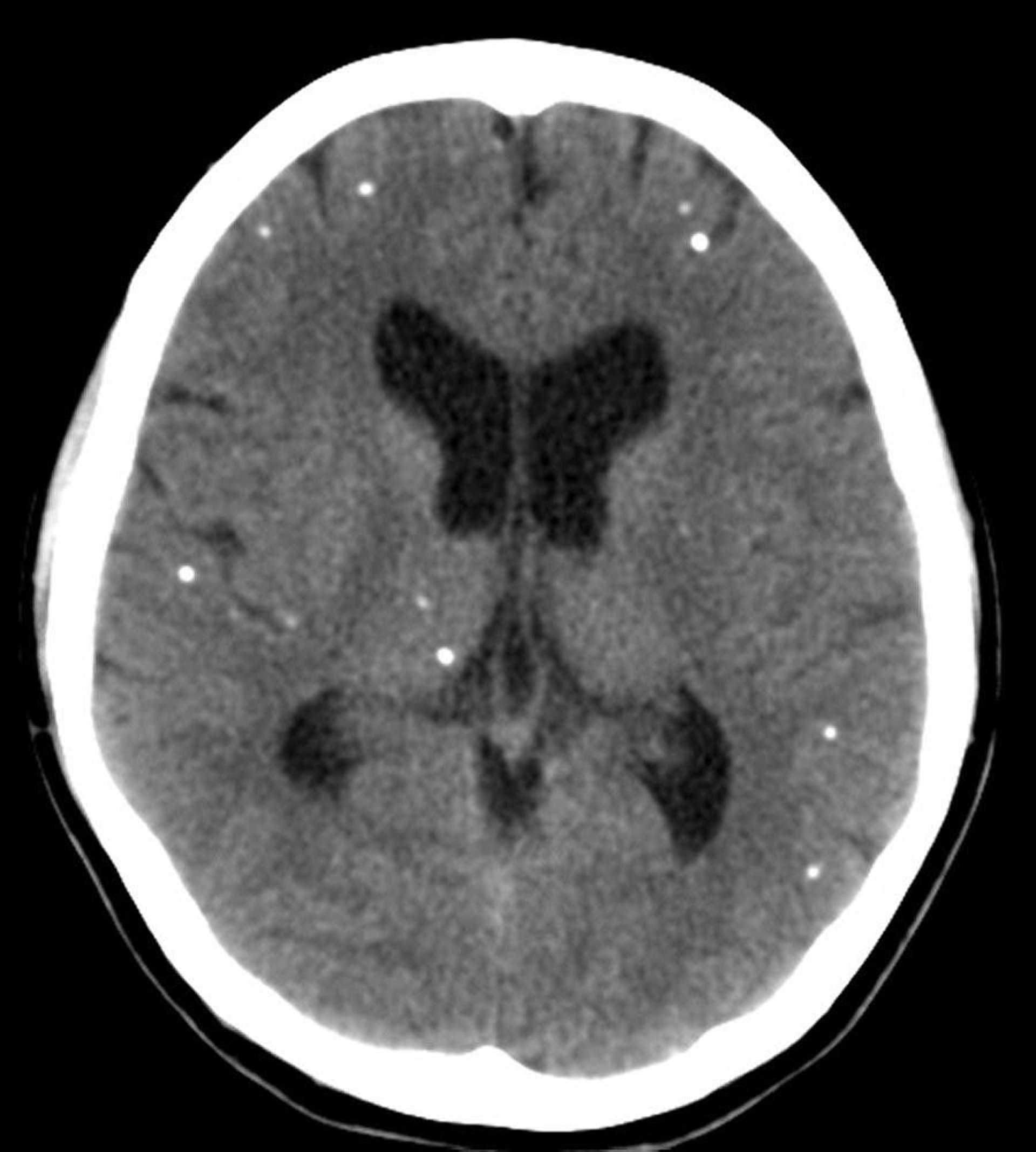
Courtesy of John E. Greenlee, MD.
Short- or long-term treatment with antiseizure drugs may be required. Surgical excision of cysts and ventricular shunts may also be required.
Other helminthic infections
In schistosomiasis, necrotizing eosinophilic granulomas develop in the brain, causing seizures, increased intracranial pressure, and diffuse and focal neurologic deficits.
Large, solitary echinococcal cysts can cause focal deficits and, occasionally, seizures.
Coenurosis, caused by tapeworm larvae (Taenia species), usually produces grapelike cysts that may obstruct CSF outflow in the 4th ventricle.
Symptoms of these cysts require several years to develop and, if the brain is involved, include increased intracranial pressure, seizures, loss of consciousness, and focal neurologic deficits. Neuroimaging and serologic testing are done to differentiate among these cysts and to differentiate them from neurocysticercosis.
Gnathostomiasis, a rare infection by larvae of the nematode Gnathostoma species, results in necrotic tracts surrounded by inflammation along the nerve roots, spinal cord, and brain or in subarachnoid hemorrhage, causing low-grade fever, stiff neck, photophobia, headache, migratory neurologic deficits (occasionally affecting the 6th or 7th cranial nerve), and paralysis. Gnathostomiasis is suspected in returning travelers and in residents of parts of Asia, the Middle East, Europe, Africa, and Central or South America who have migratory skin swellings or unexplained eosinophilic meningitis. Diagnosis requires neuroimaging and CSF testing.






