


Craniocervical junction abnormalities are congenital or acquired abnormalities of the occipital bone, foramen magnum, or first two cervical vertebrae that decrease the space for the lower brain stem and cervical cord. These abnormalities can result in neck pain; syringomyelia; cerebellar, lower cranial nerve, and spinal cord deficits; and vertebrobasilar ischemia. Diagnosis is by magnetic resonance imaging (MRI) or computed tomography (CT). Treatment often involves reduction, followed by stabilization via surgery or an external device.

JOHN T. ALESI/SCIENCE PHOTO LIBRARY

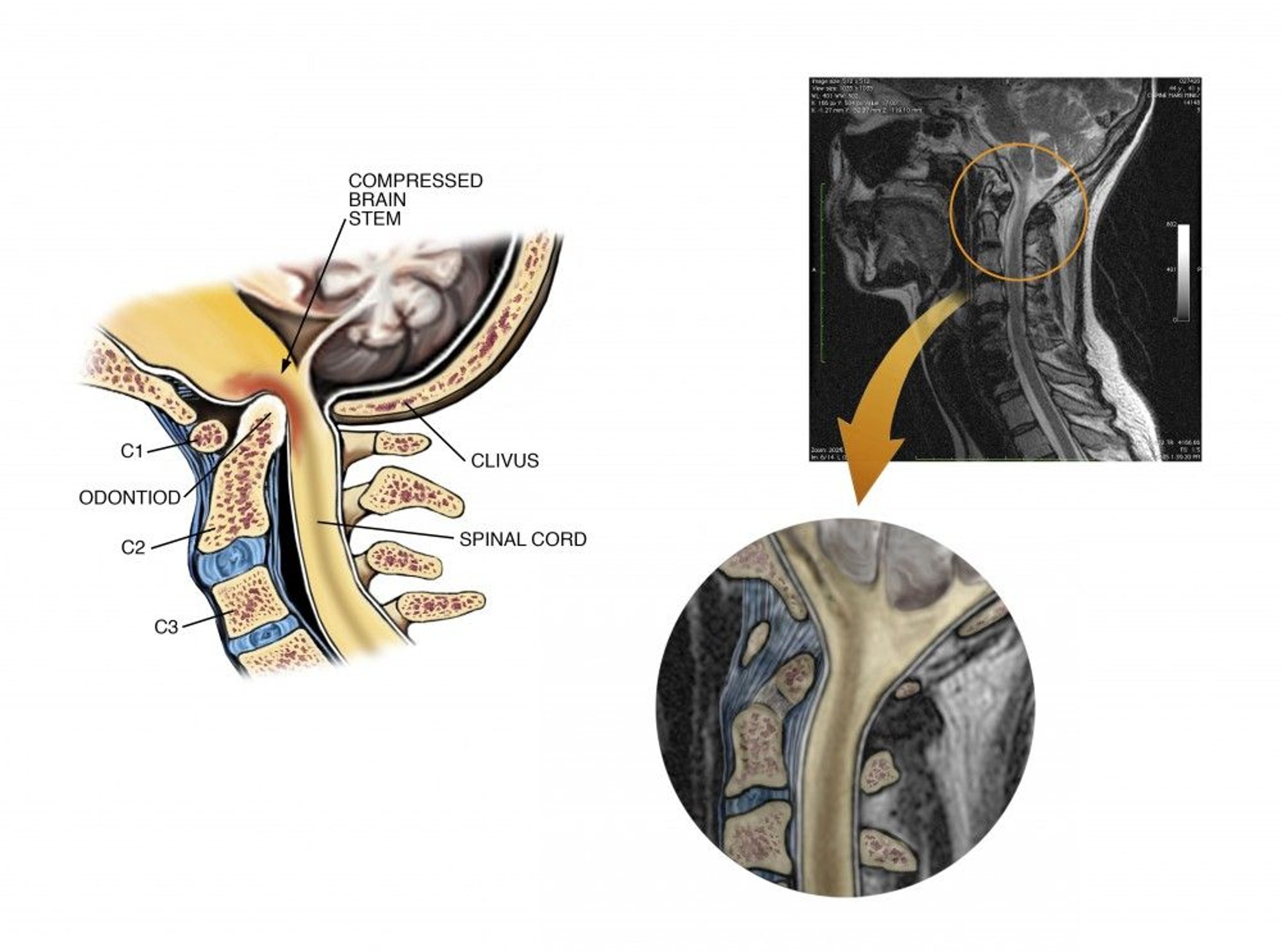
Living Art Enterprises/SCIENCE PHOTO LIBRARY
Neural tissue is flexible and susceptible to compression. Craniocervical junction abnormalities can cause or contribute to cervical spinal cord or brain stem compression; some abnormalities and their clinical consequences include the following:
Fusion of the atlas (C1) and occipital bone: Spinal cord compression if the anteroposterior diameter of the foramen magnum behind the odontoid process is < 19 mm
Basilar invagination (upward bulging of the occipital condyles): Protrusion of the odontoid process through the foramen magnum, typically shortening the neck and causing compression that can affect the cerebellum, brain stem, lower cranial nerves, and spinal cord
Atlantoaxial subluxation or dislocation (displacement of the atlas, usually anteriorly in relation to the axis but sometimes posteriorly, laterally, vertically, or rotationally): Acute or chronic spinal cord compression
Klippel-Feil malformation (fusion of the upper cervical vertebrae or of the atlas to the occiput): Deformity and limited motion of the neck but usually no neurologic consequences, but sometimes compression of the cervical cord after minor trauma
Platybasia (flattening of the skull base so that the angle formed by the intersection of the clival and anterior fossa planes is > 135°), seen on lateral skull imaging: Shortness of the neck and usually causes no symptoms unless it is accompanied by basilar invagination
Etiology of Craniocervical Junction Abnormalities
Craniocervical junction abnormalities, of which there are many, can be congenital or acquired.
Congenital
Congenital abnormalities may be specific structural abnormalities or general or systemic disorders that affect skeletal growth and development. Many patients have multiple abnormalities.
Structural skeletal abnormalities include the following:
Atlas assimilation (congenital fusion of the atlas and occipital bone)
Atlas hypoplasia
Basilar invagination
Congenital Klippel-Feil malformation (eg, with Turner syndrome or Noonan syndrome), often associated with atlanto-occipital anomalies
Os odontoideum (anomalous bone that replaces all or part of the odontoid process)
Platybasia, often with basilar invagination, Chiari malformations (descent of the cerebellar tonsils or vermis into the cervical spinal canal), and other abnormalities
Systemic disorders that affect skeletal growth and development and involve the craniocervical junction include the following:
Achondroplasia (impaired epiphyseal bone growth, resulting in shortened, malformed bones) sometimes causes the foramen magnum to narrow or fuse with the atlas and thus may compress the spinal cord or brain stem.
Down syndrome, Morquio syndrome (mucopolysaccharidosis IV), or osteogenesis imperfecta can cause atlantoaxial subluxation or dislocation.
Acquired
Acquired causes include injuries and disorders.
Injuries may involve bone, ligaments, or both and are usually caused by vehicle or bicycle accidents, falls, and particularly diving; some injuries are immediately fatal.
Rheumatoid arthritis (RA, the most common disease cause) and Paget disease of the cervical spine can cause atlantoaxial dislocation or subluxation, basilar invagination, or platybasia.
Metastatic tumors that affect bone can cause atlantoaxial dislocation or subluxation.
Slowly growing craniocervical junction tumors (eg, meningioma, chordoma) can impinge on the brain stem or spinal cord.
Symptoms and Signs of Craniocervical Junction Abnormalities
Symptoms and signs of craniocervical junction abnormalities can occur after a minor neck injury or spontaneously and may vary in progression. Presentation varies by degree of compression and by structures affected.
The most common manifestations are
Neck pain, often with headache
Symptoms and signs of spinal cord compression
Neck pain often spreads to the arms and may be accompanied by headache (commonly, occipital headache radiating to the skull vertex); it is attributed to compression of the C2 root and the greater occipital nerve and to local musculoskeletal dysfunction. Neck pain and headache usually worsen with head movement and can be precipitated by coughing or bending forward. If patients with Chiari malformation have hydrocephalus, being upright may aggravate the hydrocephalus and result in headaches.
Spinal cord compression involves the upper cervical cord. Deficits include
Spastic paresis in the arms, legs, or both, caused by compression of motor tracts
Commonly, impaired joint position and vibration senses (posterior column function)
Tingling down the back, often into the legs, with neck flexion (Lhermitte sign)
Uncommonly, impaired pain and temperature senses (spinothalamic tract function) in a stocking-glove pattern
Neck appearance, range of motion, or both can be affected by some abnormalities (eg, platybasia, basilar invagination, Klippel-Feil malformation). The neck may be short, webbed (with a skinfold running approximately from the sternocleidomastoid to the shoulder), or in an abnormal position (eg, torticollis in Klippel-Feil malformation). Range of motion may be limited.
Brain compression (eg, due to platybasia, basilar invagination, or craniocervical tumors) may cause brain stem, cranial nerve, and cerebellar deficits. Brain stem and cranial nerve deficits include
Internuclear ophthalmoplegia (ipsilateral weakness of eye adduction plus contralateral horizontal nystagmus in the abducting eye with lateral gaze)
Downbeat nystagmus (fast component downward)
Hoarseness
Dysarthria
Dysphagia
Cerebellar deficits usually impair coordination.
Vertebrobasilar ischemia can be triggered by changing head position. Symptoms may include
Intermittent syncope
Drop attacks (sudden, unprovoked falls)
Vertigo
Confusion or altered consciousness
Weakness
Visual disturbance
Syringomyelia (cavity in the central part of the spinal cord) is common in patients with Chiari malformation. It may cause
Segmental flaccid weakness and atrophy, which first appear or are most severe in the distal upper extremities
Loss of pain and temperature senses in a capelike distribution over the neck and proximal upper extremities
However, light touch is preserved.
Diagnosis of Craniocervical Junction Abnormalities
MRI or CT of the brain and upper spinal cord
A craniocervical abnormality is suspected when patients have pain in the neck or occiput plus neurologic deficits referable to the lower brain stem, upper cervical spinal cord, or cerebellum. Lower cervical spine disorders can usually be distinguished clinically (based on level of spinal cord dysfunction) and by neuroimaging.
Neuroimaging
If a craniocervical abnormality is suspected, MRI or CT of the upper spinal cord and brain, particularly the posterior fossa and craniocervical junction, is done. Acute or suddenly progressive deficits are an emergency, requiring immediate imaging. Sagittal MRI best identifies associated neural lesions (eg, medulla, pons, cerebellar, spinal cord, and vascular abnormalities; syringomyelia) and soft-tissue lesions. CT shows bone structures more accurately than MRI and may be done more easily in an emergency.
If MRI and CT are unavailable, x-rays—lateral view of the skull showing the cervical spine, anteroposterior view, and oblique views of the cervical spine—are taken.

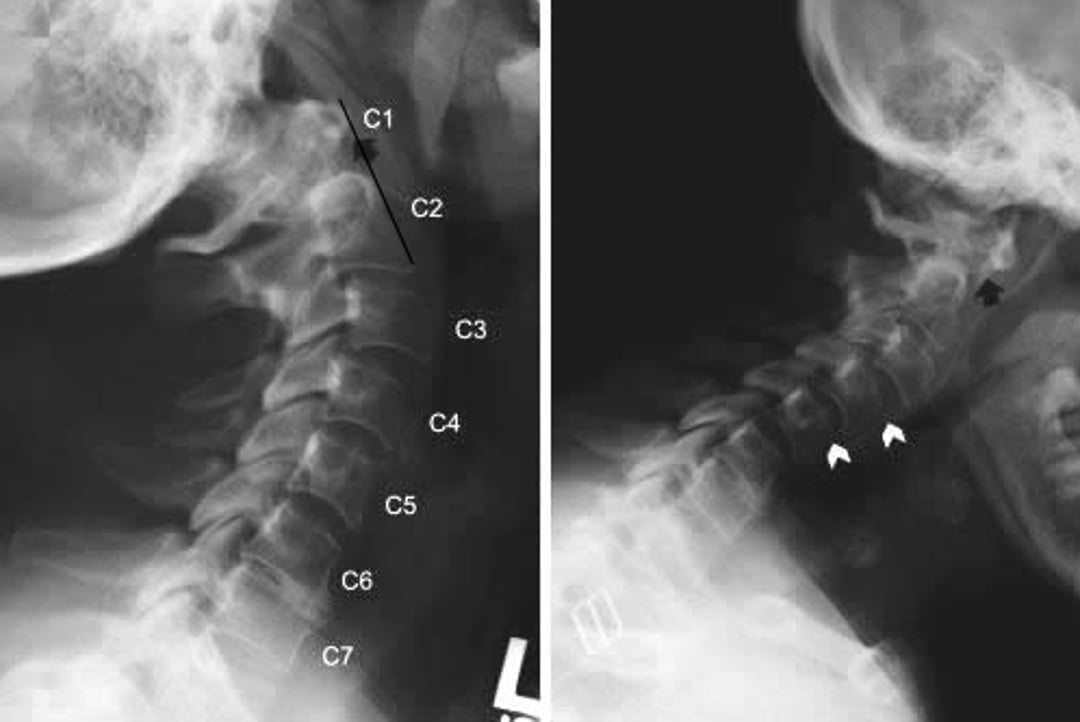
© Springer Science+Business Media

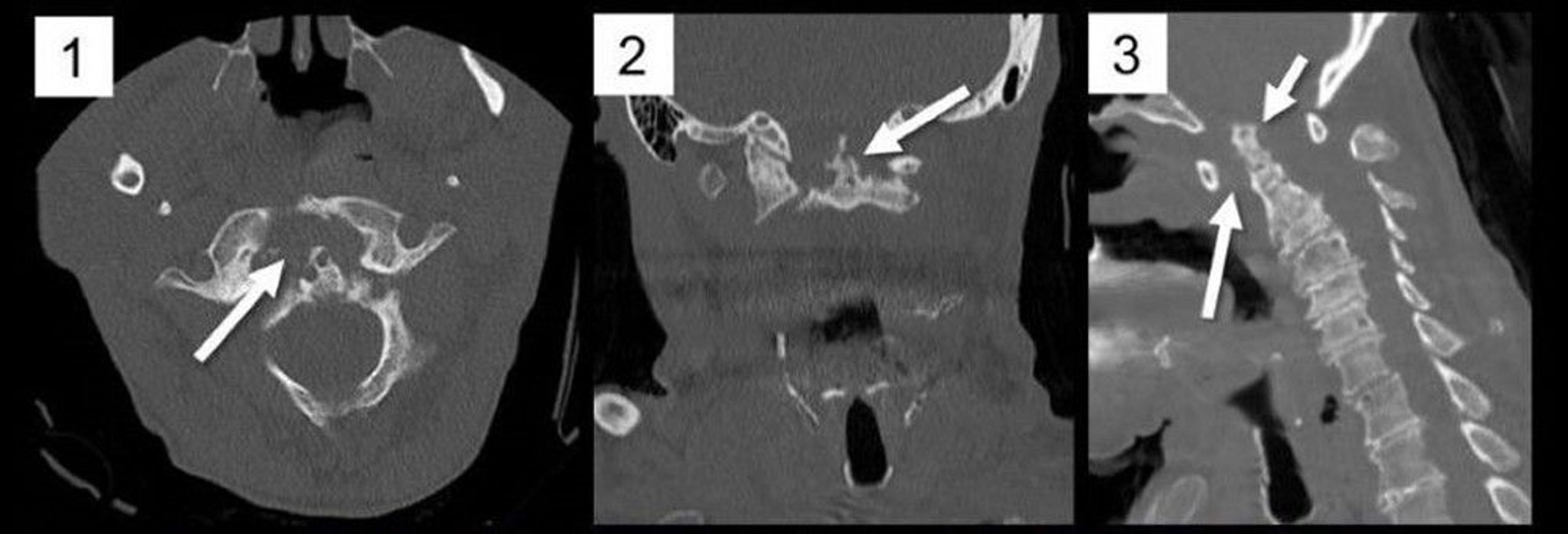
Image courtesy of A. John Tsiouris, MD.
If MRI is unavailable or inconclusive and CT is inconclusive, CT myelography (CT after intrathecal injection of a radiopaque contrast agent) is done. If MRI or CT suggests vascular abnormalities, magnetic resonance angiography or vertebral angiography is done.
Treatment of Craniocervical Junction Abnormalities
Reduction and immobilization
Sometimes surgical decompression, fixation, or both
If neural structures are compressed, treatment consists of reduction (traction or changes in head position to realign the craniocervical junction and thus relieve neural compression). After reduction, the head and neck are immobilized. Acute or suddenly progressive spinal cord compression requires emergency reduction.
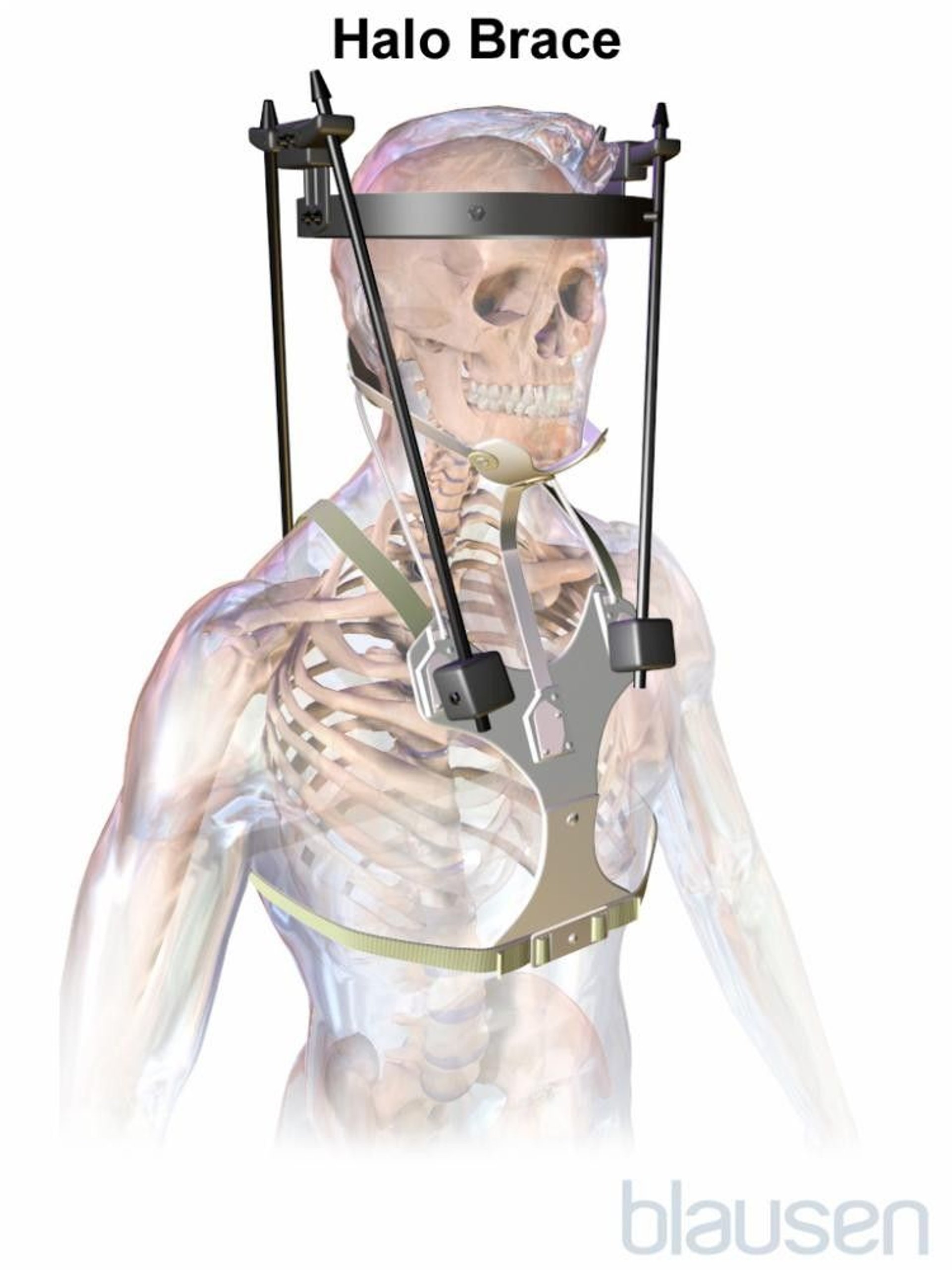
For most patients, reduction involves skeletal traction with a crown halo ring and weight of up to about 4 kg. Reduction with traction may take 5 to 6 days. If reduction is achieved, the neck is immobilized in a halo vest for 8 to 12 weeks; then x-rays must be taken to confirm stability.


Photo courtesy of Depuy/Synthes.

If reduction does not relieve neural compression, surgical decompression, using a ventral or a dorsal approach, is necessary. If instability persists after decompression, posterior fixation (stabilization) is required. For some abnormalities (eg, due to rheumatoid arthritis), external immobilization alone is rarely successful; if it is unsuccessful, posterior fixation or anterior decompression and stabilization are required.
Several different methods of instrumentation (eg, plates or rods with screws) can be used for temporary stabilization until bones fuse and stability is permanent. In general, all unstable areas must be fused.
Bone disease
Radiation therapy and a hard cervical collar often help patients with metastatic bone tumors.
Key Points
Craniocervical junction abnormalities are congenital or acquired abnormalities of the occipital bone, foramen magnum, or first two cervical vertebrae that decrease the space for the lower brain stem and cervical cord.
Suspect a craniocervical junction abnormality if patients have pain in the neck or occiput plus neurologic deficits referable to the lower brain stem, upper cervical spinal cord, or cerebellum.
Diagnose craniocervical abnormalities using MRI or CT of the brain and upper spinal cord.
Reduce and immobilize the compressed neural structures.
Treat most patients with traction, immobilization, or, if reduction is unsuccessful, surgery.




