


Initial stabilization maneuvers include mild tactile stimulation, head positioning, and suctioning of the mouth and nose followed as needed by
Supplemental oxygen
Continuous positive airway pressure (CPAP)
Noninvasive positive pressure ventilation (NIPPV)
Bag-and-mask ventilation or mechanical ventilation
Neonates who cannot be oxygenated by any of these means may require a full cardiac evaluation to exclude congenital cardiopulmonary anomalies and treatment with high-frequency oscillatory ventilation, nitric oxide, extracorporeal membrane oxygenation, or a combination.
(See also Overview of Perinatal Respiratory Disorders and Neonatal Resuscitation.)
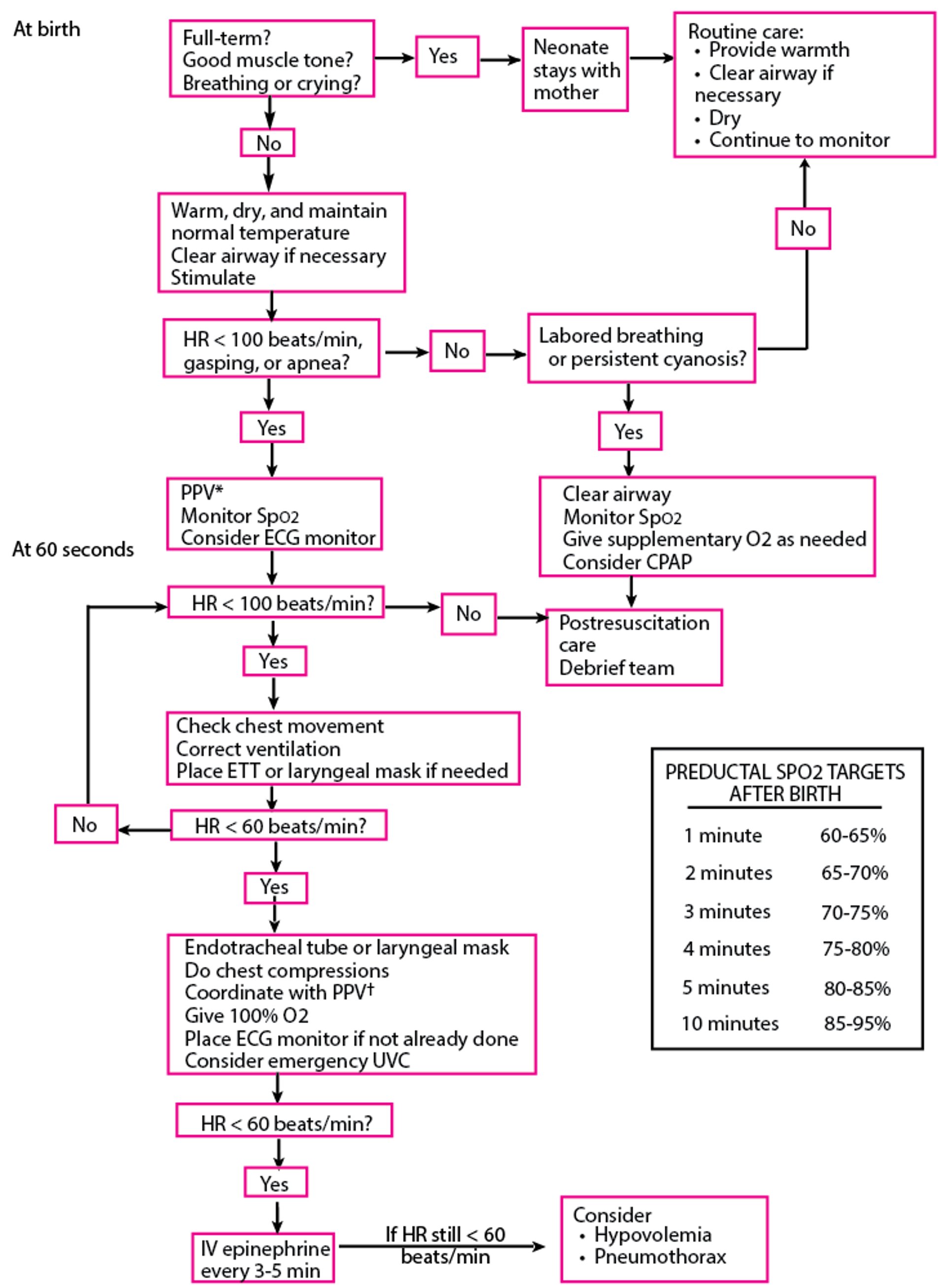
Algorithm for Resuscitation of Neonates
* PPV: Initiate resuscitation with room air (21% FiO2) for infants ≥ 35 weeks of gestational age or 21 to 30% FiO2 for infants < 35 weeks of gestational age. If SpO2 targets are not achieved, titrate inhaled oxygen concentration upward. † 3:1 compression:ventilation ratio with a total of 90 compressions and 30 breaths/minute. Compressions and ventilations are delivered sequentially, not simultaneously. Thus, give 3 compressions at a rate of 120/minute, followed by 1 ventilation over 1/2 second. CPAP = continuous positive airway pressure; ECG = electrocardiography; ETT = endotracheal tube; FiO2 = fractional inspired oxygen; HR = heart rate; PPV = positive pressure ventilation; SpO2 = oxygen saturation; UVC = umbilical venous catheter. Based on Weiner GM: Textbook of Neonatal Resuscitation, ed. 8. Itasca, American Academy of Pediatrics, 2021. |

Oxygen for Neonates and Infants
Oxygen may be given using a nasal cannula or face mask. Oxygen concentration should be set to achieve a PaO2 of 50 to 70 mm Hg in preterm infants and 50 to 80 mm Hg in term infants or an oxygen saturation of 90 to 94% in preterm infants and 92 to 96% in term infants. Lower PaO2 in infants provides almost full saturation of hemoglobin, because fetal hemoglobin has a higher affinity for oxygen; maintaining higher PaO2 increases the risk of retinopathy of prematurity and bronchopulmonary dysplasia. No matter how oxygen is delivered, it should be warmed (36 to 37° C) and humidified to prevent secretions from cooling and drying and to prevent bronchospasm.
An umbilical artery catheter is usually placed for sampling arterial blood gases in neonates who require fraction of inspired oxygen (FIO2) ≥ 40%. If an umbilical artery catheter cannot be placed, a percutaneous radial artery catheter can be used for continuous blood pressure monitoring and blood sampling if the result of the Allen test, which is done to assess adequacy of collateral circulation, is normal.
Neonates who are unresponsive to these maneuvers may require fluids to improve cardiac output and are candidates for CPAP ventilation or bag-and-mask ventilation (40 to 60 breaths/minute). CPAP, either ventilator-derived or bubble, can help avoid intubation (and thus minimize ventilator-induced lung injury) even in extremely preterm infants. However, if the infant does not oxygenate with or requires prolonged bag-and-mask ventilation, endotracheal intubation with mechanical ventilation is indicated, although very immature neonates (eg, < 28 weeks gestation or < 1000 g) are sometimes begun on ventilatory support immediately after delivery (see also 1) so that they can receive preventive surfactant therapy. Because bacterial sepsis is a common cause of respiratory distress in neonates, it is common practice to draw blood cultures and give antibiotics to neonates with high oxygen requirements pending culture results.
Oxygen reference
1. Lista G, Fontana P, Castoldi F, et al: ELBW infants: To intubate or not to intubate in the delivery room? J Matern Fetal Neonatal Med 25 (supplement 4):63–65, 2012. doi: 10.3109/14767058.2012.715008
CPAP for Neonates and Infants
In CPAP, constant pressure is maintained throughout the respiratory cycle, usually 5 to 7 cm H2O, but with no additional inspiratory pressure support. CPAP keeps alveoli open and improves oxygenation by reducing atelectasis and thereby the amount of blood shunted through atelectatic areas while the infant breathes spontaneously. CPAP can be provided using nasal prongs or masks and various apparatuses to provide the positive pressure; it also can be given using an endotracheal tube connected to a conventional ventilator with the rate set to zero.
Bubble CPAP (1) is a low-technology way of providing CPAP in which the outflow tubing is simply immersed in water to provide expiratory resistance equal to the depth of the tubing in the water (exhalation makes the water bubble, hence the name).
CPAP is indicated when FIO2 ≥ 40% is required to maintain acceptable PaO2 (50 to 70 mm Hg) in infants with respiratory disorders that are of limited duration (eg, diffuse atelectasis, mild respiratory distress syndrome, lung edema). In these infants, CPAP may preempt the need for positive pressure ventilation.
Common complications of nasal CPAP are gastric distention, aspiration, pneumothorax, and nasal pressure injuries. The need for increasing FIO2 and/or pressure are signs that intubation may be necessary (2).
CPAP references
1. Gupta S, Donn SM: Continuous positive airway pressure: To bubble or not to bubble? Clin Perinatol 43(4):647–659, 2016. doi: 10.1016/j.clp.2016.07.003
2. Fedor KL: Noninvasive respiratory support in infants and children. Respir Care 62(6):699–717, 2017. doi: 10.4187/respcare.05244
NIPPV for Neonates and Infants
NIPPV (see also Noninvasive positive pressure ventilation [NIPPV]) delivers positive pressure ventilation using nasal prongs or nasal masks. It can be synchronized (ie, triggered by the infant's inspiratory effort) or nonsynchronized. NIPPV can provide a back-up rate and can augment an infant's spontaneous breaths. Peak pressure can be set to desired limits. It is particularly useful in patients with apnea to facilitate extubation and to help prevent atelectasis. NIPPV has been found to reduce the incidence of extubation failure and the need for reintubation within 1 week more effectively than nasal CPAP; however, it has no effect on the development of chronic lung disease or on mortality.
Mechanical Ventilation for Neonates and Infants
Endotracheal tubes (ETT) are required for mechanical ventilation (see also Tracheal Intubation).
For ETT diameter:
2.5 mm (the smallest) for infants < 1000 g or < 28 weeks gestation
3 mm for infants 1000 to 2000 g or 28 to 34 weeks gestation
3.5 mm for infants > 2000 g or > 34 weeks gestation
Intubation is safer if oxygen is insufflated into the infant’s airway during the procedure. Orotracheal intubation is preferred.
For insertion depth, the tube should be inserted such that the
5.5- to 6.5-cm mark is at the lip for infants who weigh < 1 kg
7-cm mark for 1 kg
8-cm mark for 2 kg
9-cm mark for 3 kg
The tip of the endotracheal tube should be positioned about halfway between the clavicles and the carina on chest x-ray, coinciding roughly with vertebral level T2. If position or patency is in doubt, the tube should be removed and the infant should be supported by bag-and-mask ventilation until a new tube is inserted. A CO2 detector is helpful in determining that the tube is placed in the airway (no CO2 is detected with esophageal placement). Acute deterioration of the infant’s condition (sudden changes in oxygenation, arterial blood gases, blood pressure, or perfusion) should trigger suspicion of changes in the position of the tube, patency of the tube, or both.
Modes of ventilation:
Synchronized intermittent mandatory ventilation (SIMV)
Assist control (AC) ventilation
High-frequency oscillatory ventilation
In SIMV, the ventilator delivers a set number of breaths of fixed pressure or volume within a time period. These breaths are synchronized with the patient's spontaneous breaths but also will be delivered in the absence of respiratory effort. The patient can take spontaneous breaths in between without triggering the ventilator.
In AC, the ventilator is triggered to deliver a breath of predetermined volume or pressure with each patient inspiration. A back-up rate is set in the event the patient is not taking any or enough breaths.
High-frequency oscillatory ventilation (delivering 400 to 900 breaths/minute at a set mean airway pressure) can be used in infants and is often preferred in extremely preterm infants (< 28 weeks gestation) and in some infants with air leaks, widespread atelectasis, or pulmonary edema.
Optimal mode or type of ventilation depends on the infant’s response. Volume ventilators are considered useful for larger infants with varying pulmonary compliance or resistance (eg, in bronchopulmonary dysplasia), because delivering a set volume of gas with each breath ensures adequate ventilation. AC mode is often used for treating less severe pulmonary disease and for decreasing ventilator dependence while providing a small increase in airway pressure or a small volume of gas with each spontaneous breath.
Initial ventilator settings are estimated by judging the severity of respiratory impairment. Typical settings for an infant in moderate respiratory distress are
FIO2 = 40%
Inspiratory time (IT) = 0.4 seconds
Expiratory time = 1.1 seconds (both inspiratory and expiratory times vary based on rate and need; a higher inspiratory time improves oxygenation, and a higher expiratory time improves ventilation)
SIMV or AC rate = 40 breaths/minute (depends on infant's spontaneous respiratory rate and higher rates, such as 60 breaths/minute, may be needed if infant is making no spontaneous respiratory effort or lower depending on quality of infant's respiratory efforts; higher rates mandate shorter inspiratory and/or expiratory times than given above)
Peak inspiratory pressure (PIP) = 15 to 20 cm H2O for very low-birth-weight and low-birth-weight infants and 20 to 25 cm H2O for near-term and term infants
Positive end-expiratory pressure (PEEP) = 5 cm H2O
These settings are adjusted based on the infant’s oxygenation, chest wall movement, breath sounds, and respiratory efforts along with arterial or capillary blood gases.
PaCO2 is lowered by increasing the minute ventilation through an increase in tidal volume (increasing PIP or decreasing PEEP) or an increase in rate.
PaO2 is increased by increasing the FIO2 or increasing the mean airway pressure (increasing PIP and/or PEEP, or prolonging IT).
Patient-triggered ventilation often is used to synchronize the positive pressure ventilator breaths with the onset of the patient’s own spontaneous respirations. This seems to shorten the time on a ventilator and may reduce barotrauma.
Ventilator pressures or volumes should be as low as possible to prevent barotrauma and bronchopulmonary dysplasia; an elevated PaCO2 is acceptable as long as pH remains ≥ 7.25 (permissive hypercapnia). Likewise, a PaO2 as low as 40 mm Hg is acceptable if blood pressure is normal and metabolic acidosis is not present.
Adjunctive treatments used with mechanical ventilation in some patients include
Paralytics
Sedation
Nitric oxide
Inhaled nitric oxide 5 to 20 ppm may be used for refractory hypoxemia when pulmonary vasoconstriction is a contributor to hypoxia (eg, in idiopathic/persistent pulmonary hypertension, pneumonia, or congenital diaphragmatic hernia) and may prevent the need for ECMO.
Weaning from the ventilator can occur as respiratory status improves. The infant can be weaned by lowering
FIO2
Inspiratory pressure
Rate
As the rate is reduced, the infant takes on more of the work of breathing. Infants who can maintain adequate oxygenation and ventilation on lower settings typically tolerate extubation. The final steps in ventilator weaning involve extubation, possibly support with nasal (or nasopharyngeal) CPAP or NIPPV, and, finally, use of a hood or nasal cannula to provide humidified oxygen or air.
Corticosteroids, once used routinely for weaning and treatment of chronic lung disease, are no longer recommended in preterm infants because risks (eg, impaired growth, hypertrophic cardiomyopathy) outweigh benefits. A possible exception is as a last resort in near-terminal illness, in which case parents should be fully informed of risks.
Complications of mechanical ventilation
Mechanical ventilation complications more common among neonates include
Pneumothorax
Asphyxia from endotracheal tube obstruction
Ulceration, erosion, or narrowing of airway structures due to adjacent pressure from equipment
ECMO for Neonates and Infants
ECMO is a form of cardiopulmonary bypass used for infants with respiratory failure who cannot be oxygenated adequately or ventilated with conventional or oscillating ventilators. Eligibility criteria vary by center, but in general, infants should have reversible disease (eg, persistent pulmonary hypertension of the newborn, congenital diaphragmatic hernia, overwhelming pneumonia) and should have been on mechanical ventilation < 7 days. Primary cardiac compromise may also be an indication for ECMO.
sepsis). Flow rates can be adjusted to obtain desired oxygen saturation and blood pressure.
ECMO is contraindicated in infants < 34 weeks, < 2 kg, or both because of the risk of intraventricular hemorrhage with systemic heparinization.
Complications of ECMO include thromboembolism, air embolization, neurologic (eg, stroke, seizures) and hematologic (eg, hemolysis, neutropenia, thrombocytopenia) problems, and cholestatic jaundice.






