Inflammation of the oral tissues can be either primary or secondary. Inflammation in the oral cavity may affect the gingiva (gingivitis), nongingival tissues of the periodontium (periodontitis), alveolar mucosa (alveolar mucositis), sublingual mucosa (sublingual mucositis), lip and cheek mucosa (labial and buccal mucositis), lip (cheilitis), oral mucosa (stomatitis), mucosa of the dorsal or ventral tongue surface (glossitis), mucosa of the caudal oral cavity (caudal mucositis), mucosa forming the lateral walls of the pharynx (faucitis), mucosa of the palate (palatitis), palatine tonsil (tonsillitis), or mucosa of the pharynx (pharyngitis). The nature and severity of the lesions vary greatly depending on the etiology and duration of the disease. Contact mucositis and contact mucosal ulceration represent lesions in susceptible animals that are secondary to mucosal contact, with a tooth surface bearing the responsible irritant, allergen, or antigen. They have also been called “contact ulcers” and “kissing ulcers.” Stomatitis is inflammation of the mucous lining of any of the structures in the mouth; in clinical use, the term should be reserved to describe widespread oral inflammation (beyond gingivitis and periodontitis) that may also extend into submucosal tissues (eg, marked caudal mucositis extending into submucosal tissues may be termed caudal stomatitis).
Periodontal disease, including gingivitis and periodontitis, is the most common oral problem in small animals. Gingivitis is a gingival inflammatory response to the presence of bacterial plaque on an adjacent tooth surface. Periodontitis is inflammation of nongingival tissues of the periodontium (namely periodontal ligament and alveolar bone); it results from the combination of bacterial periodontopathogens and the host's immune response that together destroy the tooth-supporting tissues. (Also see Periodontal Disease in Small Animals.)
Periapical disease (granuloma, abscess, or cyst) is usually caused by endodontic disease (spread of infection and inflammation from within the tooth through the apical foramina into the periapical tissues). Clinically, a sinus tract may develop that manifests as a circular raised area of inflamed granulation tissue with a central draining fistula that opens near the mucogingival junction. The tract can be followed to the primary periodontal or periapical lesion, and the etiology resolved. (Also see Endodontic Disease in Small Animals.) A parulis is a true periodontal abscess (eg, an encapsulated mucopurulent lesion within a periodontal pocket).


Courtesy of Dr. Gregg A. DuPont.
Other causes of oral inflammatory conditions include immunopathy (eg, autoimmune disease, immune deficiency), chemical agents, infectious disease, trauma, metabolic disease, developmental anomalies or conformational anatomy that predisposes to irritation or inflammation, burns, radiation therapy, or neoplasia. Infectious agents that have been associated with oral inflammation, glossitis, stomatitis, and oral ulcerations include feline herpesvirus, feline calicivirus, feline leukemia virus, feline immunodeficiency virus, canine distemper virus, Bartonella henselae, and certain Leptospira serovars. Traumatic stomatitis may be seen after oral exposure to plant material (embedded plant awns) or fiberglass insulation. When chewed, plants of the species Dieffenbachia may also cause oral inflammation and ulcers. Contact with processionary caterpillars may also cause severe glossitis. Thallium is the major heavy metal responsible for oral lesions; incidence of this toxicity is low. Uremia can cause stomatitis and oral ulcers. Recurrent oral ulcerations are also seen in gray Collies with cyclic hematopoiesis.
Signs vary widely with the cause and extent of inflammation. Anorexia may be seen, especially in cats. Halitosis and drooling are common with caudal stomatitis or glossitis, and saliva may be blood tinged. The animal may paw at its mouth and resent any attempt to examine the oral cavity because of pain. Regional lymph nodes may be enlarged.
Feline Stomatitis


Courtesy of Dr. Ben Colmery III.
Feline stomatitis (FS) is a relatively uncommon (3% of feline oral problems) but serious condition. Affected cats present with progressively worsening inflammation of oral mucosal tissues (particularly the gingiva, alveolar mucosa, labial and buccal mucosa, sublingual mucosa, and mucosa of the caudal oral cavity) and increasing levels of discomfort. More significantly, the mucosa of the caudal oral cavity and the area at and lateral to the palatoglossal folds are often severely ulcerated, friable, inflamed, and proliferative. Severe ulceroproliferative inflammation that involves this area bilaterally in the back of the mouth is pathognomonic for FS. The cause is unproved, but it is suspected to result from an inappropriate inflammatory response in affected cats to one or more antigens. A high percentage of affected cats (100% in some studies) are chronic carriers of feline calicivirus. FS may be caused by the sum of multiple sensitivities in an individual, with antigen on the tooth surfaces, including the root surfaces and periodontal ligament, exceeding a threshold.


Courtesy of Dr. Gregg A. DuPont.
The most immediate sign is severe pain when opening the mouth. Cats vocalize and jump when they yawn or open their mouth to eat. Halitosis, ptyalism, and dysphagia may be seen. Cats often show an “approach-avoidance” behavior as they approach their food in hunger, then hiss and run off in anticipation of discomfort. If the condition is severe and of long duration, weight loss may be evident. The disease is slowly progressive and may not be recognized until lesions have become severe. Mandibular lymphadenopathy is sometimes present. Pain often prevents adequate examination of the oral cavity without sedation or anesthesia.
Diagnosis:
Diagnosis is made by visual identification of bilateral inflammation of the mucosa of the caudal oral cavity and the tissues at or lateral to the palatoglossal folds during oral examination. In advanced cases, the cat will strongly object to opening the mouth. Additional tests include virus isolation (eg, calicivirus and herpesvirus), retroviral tests, and evaluation for systemic disease (eg, renal failure). Although a definitive association with Bartonella infection has not been shown, testing has been recommended. In atypical cases (unilateral involvement, usually proliferative focal lesion), biopsy and histopathologic evaluation is required to exclude oral neoplasia or other specific oral disorders. Most biopsy samples collected from chronic inflammatory or ulcerated lesions reveal a predominance of lymphocytes and plasma cells, which indicate the chronic inflammatory nature of the lesion without elucidating the primary etiology.
Treatment:
Partial-mouth extraction (removal of all premolars and molars) or full-mouth extraction (removal of all teeth) and debridement of the associated soft and hard tissues is the only treatment to provide lasting improvement and aid in overall longterm control. Partial- or full-mouth extractions provide significant improvement in 60%–80% of affected cats when done early in the disease course and when no root tips or fragments are left behind. Chronically affected cats treated medically for many months have a poorer prognosis after surgery. Dental radiographs of areas with missing teeth are required to check for retained roots. Any retained root fragments must be removed, because they will prevent improvement. Postoperatively, medical therapy focuses on controlling inflammation, infection, and pain. Oral administration of corticosteroids such as prednisolone is less effective than SC or IM injection of methylprednisolone. An alternative is transdermal administration of prednisolone. In refractory cases, use of interferon omega may be considered, injected intralesionally before the start of oral administration. Commonly used antibiotics include amoxicillin-clavulanic acid or clindamycin, but the response to treatment may be lacking or only transient. Culturing the lesions and performing susceptibility tests are rarely indicated, even in chronic or recurrent infections. Nutritional support is required in chronic cases with severe weight loss and dehydration. Pain control with sublingual buprenorphine or a transdermal fentanyl patch should also be considered, along with dietary changes (nonallergenic, soft palatable foods) and administration of topical antiseptics (eg, dilute chlorhexidine or zinc ascorbate). Placement of a feeding tube should be considered in debilitated cats that do not respond to therapy.
Many other treatments for FS have been reported, including good home oral hygiene, periodontal therapy, frequent dental cleanings, cyclosporine therapy, laser therapy, and bovine lactoferrin. Perhaps with the exception of cyclosporine, none of these provide longterm resolution. Corticosteroid administration alone usually results in significant and immediate clinical improvement from modulation of the excessive inflammatory response, but it is not recommended except as a last resort. Without surgery (ie, partial- or full-mouth extractions), repeated use of corticosteroids is frequently required. This treatment becomes progressively less effective and eventually completely ineffective. In addition, cats that have received repeated corticosteroid treatments have a poorer prognosis once the teeth are extracted. Partial- or full-mouth extractions often result in significant improvement or complete resolution of the inflammation if performed early in the course of the disease and before multiple corticosteroid treatments.
Canine Stomatitis
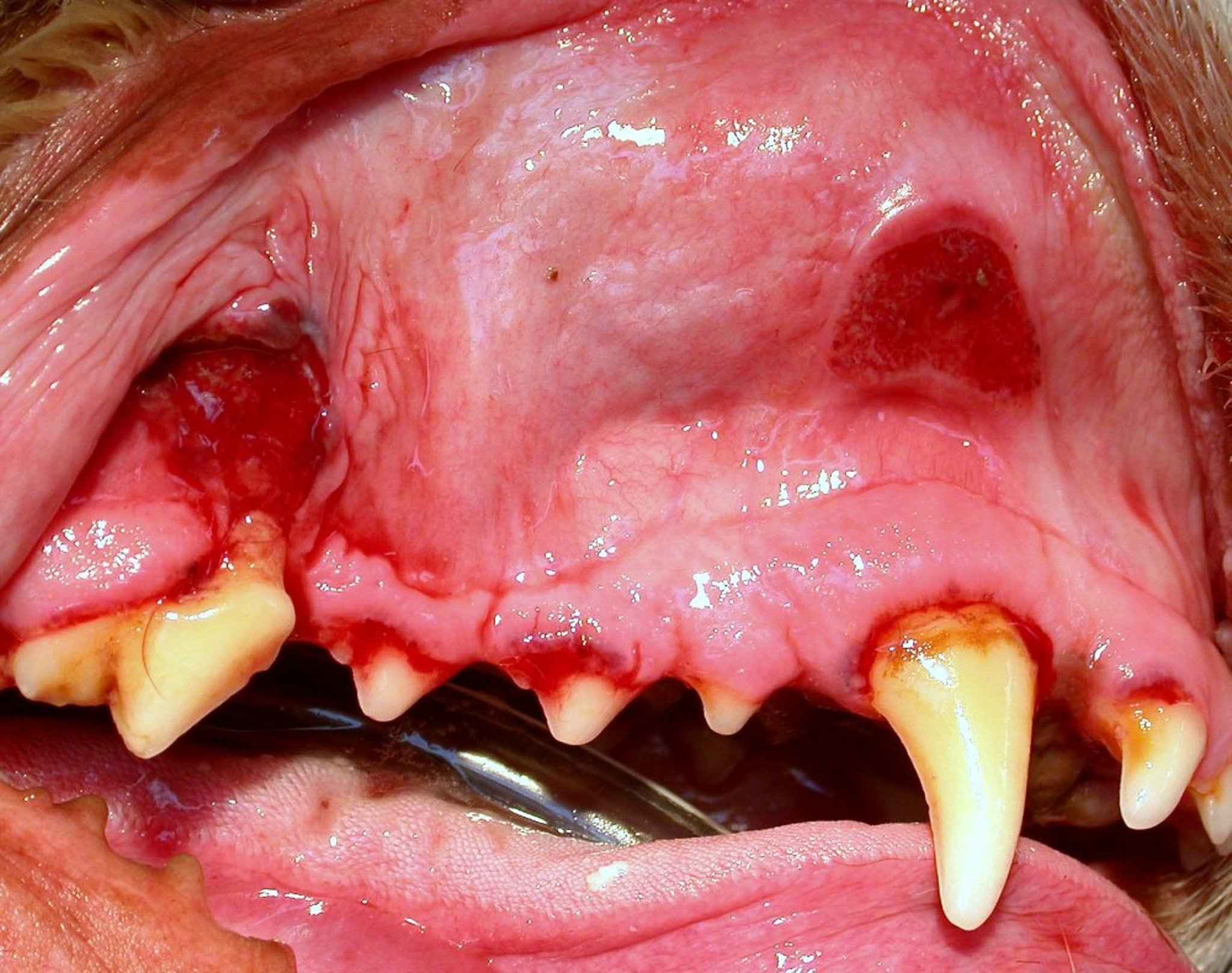
Characteristics of canine stomatitis that often manifest as contact mucositis and contact mucosal ulceration (also called chronic ulcerative paradental syndrome or CUPS) include severe gingivitis, multiple sites of gingival recession and dehiscence, and large areas of ulcerated labial and buccal mucosa adjacent to the surfaces of large teeth. The problem commonly affects Greyhounds, and it has also been seen in Maltese, Miniature Schnauzers, Labrador Retrievers, and other breeds.
Diagnosis:

Courtesy of Dr. Gregg A. DuPont.
Diagnosis of canine stomatitis is by clinical observation of the typical oral lesions after excluding other etiologies such as uremic stomatitis, caustic stomatitis, or specific infectious agents. The characteristic lesion is the contact ulcer that develops where the lip or cheek mucosa contacts the tooth surface, most commonly on the inner surface of the upper lip adjacent to the upper canine and carnassial teeth. These lesions have also been termed “kissing ulcers” or "kissing lesions," because they are found where the lips “kiss” the teeth. An immune profile should be done, and a biopsy considered for histopathology.
Treatment:
The underlying pathology of canine stomatitis is an immunopathy that results in an excessive local inflammatory response to the antigens in dental plaque. Eliminating, or at least minimizing, plaque through professional dental cleaning and meticulous home oral hygiene (twice daily tooth brushing) may resolve the problem. However, even slight residual plaque on the tooth surfaces will perpetuate the inflammation and ulcerations. Supplemental antimicrobial measures with topical chlorhexidine gluconate rinses or gels and possibly oral antibiotic treatment with metronidazole should also be used. In severe cases, topical anti-inflammatory preparations to modulate the inflammatory response may provide comfort. Discomfort caused by the ulcers complicates efforts to brush the teeth and administer oral medications. In cases in which discomfort is severe and the owners are unable or unwilling to brush the teeth, extraction of all teeth associated with ulcers may be necessary to remove the contact surfaces on which plaque accumulates. Although this may help control the lesions, it is not curative, because plaque forms on mucosal surfaces in the mouth, including the tongue. In some cases with complete extractions, dogs continue to develop lesions due to a hyperimmune response to the plaque.
Lip Fold Dermatitis and Cheilitis
Lip fold dermatitis is a chronic, moist dermatitis seen most commonly in breeds that have pendulous lips and lower lateral lip folds (eg, spaniels, English Bulldogs, Saint Bernards) that have prolonged contact with saliva. The lesions may be exacerbated when poor oral hygiene results in increased salivary bacterial levels. The lower lip folds can become very malodorous, inflamed, uncomfortable, and swollen.

Courtesy of Dr. Ben Colmery III.
Lip wounds, resulting from fights or chewing on sharp objects, are common and vary widely in severity. Thorns, grass awns, plant burrs, and fishhooks may embed in the lips and cause marked irritation or severe wounds. Irritants such as plastic or plant material can produce inflammation of the lips. Lip infections may develop secondary to wounds or foreign bodies or can be associated with inflammation of adjacent areas. Direct extension of severe periodontal disease or stomatitis can produce cheilitis. Licking areas of bacterial dermatitis or infected wounds can spread the infection to the lips and lip folds. Other causes of inflammation of the lips include parasitic infections, autoimmune skin diseases, and neoplasia.
Clinical Findings and Diagnosis:
Inflammation of the lips and lip folds can be acute or chronic. Animals with cheilitis may paw, scratch, or rub at their mouth or lip; have a foul odor on the breath; and occasionally salivate excessively or be anorectic. With chronic infection of the lip margins or folds, the hair in these areas is discolored, moist, and matted with a thick, yellowish or brown, malodorous discharge overlying hyperemic and sometimes ulcerated skin.
Cheilitis due to extension of infection from the mouth or another area of the body usually is detected easily because of the primary lesion.
Treatment:
Medical management of lip fold dermatitis includes clipping the hair, cleaning the folds 1–2 times/day with benzoyl peroxide or a mild skin cleanser, and keeping the area dry. Topical diaper rash cream applied daily may be helpful. Surgical correction (cheiloplasty) of deep lip folds is a more longlasting remedy.
Cheilitis that is unrelated to lip folds usually resolves with minimal cleansing, appropriate antibiotics if a bacterial infection is present, and specific treatment of primary etiologies (eg, autoimmune skin disease). Wounds of the lips should be cleaned and sutured if necessary. Treatment of periodontal disease or stomatitis is necessary to prevent recurrence.
Infectious cheilitis that has spread from a lesion elsewhere usually improves with treatment of the primary lesion, but local treatment also is necessary. With severe infection, hair should be clipped from the lesion and the area gently cleaned and dried. Antibiotics are indicated if the infection is severe or systemic.
Mycotic Stomatitis
Mycotic stomatitis caused by overgrowth of the opportunistic yeast Candida albicans is an uncommon cause of stomatitis in dogs and cats. It is characterized by stomatitis, halitosis, ptyalism, anorexia, oral ulceration, and bleeding from the oral tissues. It is usually thought to be associated with other oral diseases, longterm antibiotic therapy, or immunosuppression. Diagnosis is confirmed by culture of the organism from the lesion or by histologic evidence of tissue invasion.

Courtesy of Dr. Ben Colmery III.
Any existing underlying local or systemic diseases affecting the oral cavity should be treated. Ketoconazole or a related benzimidazole should be administered until the lesions resolve, after which antibiotic therapy should be discontinued. An adequate level of nutrition should be maintained. The prognosis is guarded if predisposing diseases cannot be adequately treated or controlled.
Acute Necrotizing Ulcerative Gingivitis
Acute necrotizing ulcerative gingivitis (ANUG) is a relatively uncommon disease of dogs characterized by severe gingivitis, ulceration, and necrosis of the oral mucosa. Fusobacterium spp and spirochete organisms (Borrelia vincenti), normal inhabitants of the mouth, have been suggested as a cause of this disease after some predisposing factor increases their numbers or decreases the local resistance of the oral mucosa. The role, if any, of these organisms in causing disease is unknown. In people, Bacteroides melaninogenicus intermedius may play a more important role. Other potential factors are stress, excess glucocorticoid administration in susceptible dogs, and poor nutrition.
The disease appears first as reddening and swelling of the gingival margins and interdental papillae, which are painful, bleed easily, and may progress to gingival recession. Extension to other areas of the oral mucosa is common, resulting in ulcerated, necrotic mucous membranes and exposed bone in severe cases, leading to osteomyelitis and osteonecrosis. Halitosis is severe, and the animal may be anorectic because of pain. Ptyalism sometimes occurs, and the saliva may be blood tinged. Differential diagnoses include severe periodontal disease, autoimmune skin disease, uremia, neoplasia, and other systemic disease associated with oral lesions.
Diagnosis is made by exclusion of other etiologies.
Treatment of periodontal disease, partial- or full-mouth extractions, debridement of lesions, oral hygiene, antibiotics (amoxicillin-clavulanate, ampicillin, clindamycin, metronidazole, tetracyclines), and oral antiseptics (dilute chlorhexidine solution or gel) are indicated.
Glossitis


Courtesy of Dr. Ben Colmery III.
Glossitis, an acute or chronic inflammation of the tongue, may be due to infectious (calicivirus, herpesvirus, rhinotracheitis virus, leptospirosis), physical (irritation from excess calculus and periodontal disease, foreign bodies that penetrate or become lodged under the tongue, traumatic wounds), or chemical agents; metabolic disease (uremia, hypoparathyoidism, diabetes); or other causes such as electric or thermal burns and insect stings. Foreign body glossitis is especially a problem in longhaired dogs that attempt to remove plant burrs from their coats.

Courtesy of Dr. Ben Colmery III.
Drooling and a reluctance to eat are common signs, but the cause may go undiscovered unless the mouth is carefully examined. Periodontitis may result in reddening, swelling, and occasionally ulceration of the lateral edges and the tip of the tongue. A thread, string, or other linear foreign body may get caught under the tongue. There may be no inflammation of the dorsal surface of the tongue, but the ventral surface is painful, shows acute or chronic irritation, and frequently is lacerated by the foreign body. Porcupine quills, plant material, and other foreign materials may become embedded so deeply they are not palpable. Insect stings cause acute swelling of the tongue.
In chronic cases of ulcerative glossitis, a thick, brown, foul-smelling discharge (occasionally with bleeding) may be present. Frequently, the animal is reluctant to allow oral examination.


Courtesy of Dr. Gregg A. DuPont.
Fissured, or plicated, tongue (lingua dissecta) describes a textural variation of the dorsum of the tongue with deep central or lateral longitudinal grooves. The fissure deepens with age and is therefore thought to be acquired from some extrinsic factor. However, it may also represent a developmental anomaly. The groove often becomes deeply filled with hairs that act as a local irritant, causing inflammation and discomfort.
Any foreign bodies or hairs should be removed, and broken or diseased teeth removed or treated. Bacterial infectious glossitis should be treated with an appropriate systemic antibiotic. Debridement and dilute chlorhexidine mouthwashes are beneficial in some cases. Lingual curettage is sometimes required if foreign material is embedded in the tongue. A soft diet and parenteral fluids are administered as needed. If the animal is debilitated and unable to eat well for a prolonged period, a feeding tube to allow for nutritional support should be considered. Acute glossitis due to insect stings may require emergency treatment.
If the glossitis is secondary to another condition, the primary disease should be treated. Tongue tissues heal rapidly after irritation and infection have been eliminated.