Equine ascarid infection can cause small intestinal impactions. Exposure to Parascaris spp is common worldwide, but disease is exceedingly rare. Foals typically present with gastric reflux, elevated heart rate, and pain. Ultrasonography can be used to diagnose impaction. Most cases with impaction require surgery. Complications include intussusception, volvulus, or intestinal rupture. Benzimidazoles are effective anthelmintics for equine ascarids.
Two ascarid species infect horses, Parascaris equorum and P univalens. Little is known about the biologic differences between the two species, and recent data suggests that P univalens is common around the world, whereas P equorum is extremely rare.
Ascarid eggs are regarded as environmentally durable and are claimed to remain infectious for several years. However, survival is temperature-dependent, because eggs do not tolerate temperatures exceeding 40˚C for more than a few days. Eggs are likely to remain viable over winter in most climates and be infective in the following foaling season. Eggs are infective once they have embryonated and contain infective larvae.


Once ingested, the eggs hatch and L3 larvae begin hepato-tracheal migration, , arriving in the lungs ~1 week postinfection. Here, they penetrate the alveoli and bronchioles, where they remain for ~2 weeks before they are coughed up into the pharynx and swallowed to return to the small intestine as L4 larvae. The first intestinal stages appear 3–4 weeks postinfection. The parasites then require ~2 months before they become adults and begin shedding eggs at 90–110 days postinfection. Ascarid worm burdens reach their highest levels in foals at ~5 months of age, after which a mounting immune response begins clearing the infection, regardless of anthelmintic treatment. Weanlings and yearlings can sometimes become reinfected to a lesser degree, but the majority of ascarid burdens are eliminated as foals reach 1 year old.
The median age of reported cases of ascarid small intestinal impaction is 5 months, which coincides with the worm burden peak, but cases have been reported in yearlings, young adults, and fully mature horses as well.
Clinical Signs of Ascarid-associated Colic in Horses
The classic case of ascarid-associated colic is a foal aged 5 months old recently dewormed with an effective anthelmintic. The foal may have an anthelmintic treatment history of no treatments administered during the months before the event or usage of anthelmintics to which resistance is commonly reported in Parascaris spp, such as ivermectin. The foal may present with these clinical signs:
elevated heart rate
dehydration
hyper- or hypoperistalsis
positive gastric reflux
hyperemic mucous membranes
clear signs of pain and limited response to analgesics
Clinical laboratory findings are typically unremarkable but transabdominal ultrasonography can reveal dilated loops of small intestine with hyperechoic worms clearly visible.
The pulmonary stages of Parascaris spp infection have caused bronchitis or bronchopneumonia in experimentally inoculated foals, but this is not reported to be a clinically significant sign in domestic horses.
Diagnosis of Ascarid-associated Colic in Horses
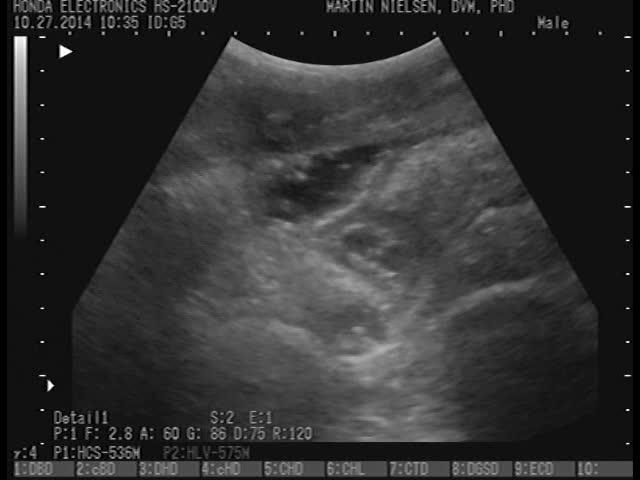
Ascarid eggs in a fecal sample document the presence of sexually mature female parasites, but this does not correlate with risk of impaction because a majority of 5-month-old foals are likely to be ascarid positive. Transabdominal ultrasonography, however, is diagnostic of the condition because the worms are easily visualized, and additional findings such as thickened mucosal walls and dilated loops of small intestine can be noted.
Treatment of Ascarid-associated Colic in Horses
In the acute presentation, treatment should be directed at resolving the small intestinal impaction. If surgery is elected, it can either include enterotomy and removal of as many worms as possible or a less invasive approach, where the parasites are milked/massaged into the cecum. Whereas the latter implies less contamination and risk of intestinal adherences or strictures, the massaging can still inflict trauma to the serosal surfaces of the intestines, which can lead to complications as well.
A more conservative medical approach can be taken in cases presenting with no gastric reflux and controllable pain manifestations. Administration of mineral oil can be combined with spasmolytic medication and fluid therapy. A full labelled dose of a benzimidazole should be administered and gastric reflux checked every 3 hours for the initial 24–48 hours or until the patient is stabilized. Dead adult worms may be recovered via nasogastric tube or found in the feces. Progression can be monitored with frequent ultrasonography.
The above procedures should be combined with the following supporting measures, where appropriate:
fluid therapy
pain medication
correction of acidosis/alkalosis
anti-inflammatory therapy
antibiotics
The current recommendation is to include an anthelmintic as part of the treatment plan. Benzimidazoles are generally recommended due to the low levels of resistance reported in equine ascarids as well as the nonparalytic mode of action, in which worms die over the course of 2–3 days. Given the high levels of resistance reported throughout the world, macrocyclic lactones are unlikely to work well against these parasites. Pyrantel products may be effective but should be used with caution because of their paralytic mode of action.
Prevention of Ascarid-associated Colic in Horses
Current parasite control recommendations are designed to reduce the risk of parasitic disease through fecal diagnostic testing, routine monitoring of anthelmintic efficacy, and a combination of strategic and targeted treatments. It is generally recommended to target Parascaris spp twice before weaning, with treatments given at ~2 months of age and at ~5 months or before weaning. The anthelmintic of choice should be a benzimidazole at the labelled dose. Fecal egg counts determined before and after the 5-month treatment can be used to 1) determine the relative presence of strongyles versus ascarids, and 2) evaluate the treatment efficacy against these and guide the need to separately target strongyle parasites, if necessary. A detailed presentation of current recommendations for equine parasite control can be found in the American Association for Equine Practitioners (AAEP) Guidelines (see below).
Zoonotic Risk of Ascarid-associated Colic in Horses
None.
Key Points
Parascaris spp parasites are ubiquitous in foals across the world, but disease is extremely rare.
Diagnosis of ascarid-associated colic is by clinical presentation and transabdominal ultrasonography.
Most patients require surgery, but a conservative approach can be taken in less severe cases.
Current recommendations for equine parasite control are designed to reduce the risk of parasitic disease, including ascarid-associated colic.
For More Information
Recommendations from the AAEP for equine parasite control
Also see pet health content regarding ascarids in horses.