Equine emergencies can often be distilled to the basics of resuscitation, establishing an airway and maintaining adequate circulatory volumes. It is imperative in an emergent situation to provide a timely fluid resuscitation plan or establish an airway in a horse with an upper airway obstruction. In addition, abdominal emergencies are one of the most common problems identified by the equine practitioner. Diagnosis is often aided by nasogastric intubation as well as samples obtained from the abdominal cavity, which can be used to guide therapeutic recommendations.
Emergency Fluid Therapy
In emergency situations, resuscitation fluids are often indicated to replace blood volume and interstitial deficits. Lack of adequate circulating volume can lead to multi-organ dysfunction or failure and increase mortality in horses with hypovolemic shock.
Conditions that may require emergency fluid replacement include:
injuries with concurrent blood loss
physical exhaustion
acute rhabdomyolysis
hyperthermia
circulatory shock secondary to systemic illness
Fluids may be needed for maintenance purposes when oral intake is physically not possible. Replacement fluids are required when excessive losses have been incurred or ongoing fluid losses anticipated.
Design of a fluid therapy regimen requires consideration of the volume required, the type of fluids needed, and the route and rate of administration.
Determining Fluid Volume in Equine Emergencies
The volume to be administered throughout 24 hours can be estimated using the following formula:
volume to administer (L) = maintenance rate (60 mL/kg/day) + estimated fluid deficit (body wt [kg] × estimate of dehydration) + estimate of ongoing losses
Maintenance fluid requirements are ~1 L/hour for adult horses (~450 kg) but are much lower if the animal is not eating. Dehydration can be estimated by using clinical and laboratory parameters ( see Table: Physical and Laboratory Parameters for Estimation of Dehydration in Horses). These numbers should be considered in relation to the horse’s age and clinical condition and are only an estimate of the deficit. For example, a nervous horse may have a transiently high heart rate in response to excitement and an increased PCV because of splenic contraction.
Ongoing losses are difficult to estimate, because losses from the GI tract are hard to measure. The equine GI tract secretes and reabsorbs the equivalent of the extracellular fluid volume (~30% of body weight) on a daily basis. If small-intestinal ileus or obstruction is present, the amount of gastric reflux obtained can be easily quantitated to gauge losses. If the large intestine is not reabsorbing water (eg, diarrhea), fluid losses can be significant but difficult to measure. With severe diarrhea, ~50% of the extracellular fluids can be lost daily.
The formula to calculate volume of fluid to administer provides only a crude estimate of needs; volumes administered should be adjusted based on response to treatment, including:
heart rate
pulse quality
capillary refill time
urine production
PCV
serum total protein
creatinine
lactate
Reassessment is required to adjust the daily fluid requirements for any horse receiving supplemental fluids, and the timing should be dictated by the horse’s clinical condition. In horses in severe shock, cardiovascular parameters may need to be monitored continually (eg, every 15 minutes) until improvement is noted. In horses with severe ongoing fluid losses (eg, diarrhea, anterior enteritis), cardiovascular parameters should be reassessed every 4 hours and laboratory parameters measured as frequently as 4 times a day until the horse stabilizes.
Selecting Fluid Type in Equine Emergencies
After determination of volume required, the type of fluid to be administered should be selected. Fluid choices include crystalloids (fluids containing substances that freely cross the capillary membrane) and colloids (fluids retained in the vascular space for a certain number of hours because of their larger molecular size). Crystalloids are most commonly used for replacement fluid therapy, whereas colloids are more often reserved for resuscitation purposes.
Two general types of crystalloids are available: balanced electrolyte solutions (BES), which are solutions of electrolytes in concentrations similar to those in plasma, and saline solutions, which contain only sodium chloride. Although considered a crystalloid, dextrose solutions are rarely used alone and are usually added as a supplement to a BES when indicated by the needs of the individual horse. The decision to choose BES or saline can be based on a serum chemistry profile. In most emergency cases, a BES is used.
The addition of colloids to a fluid therapy regimen serves two purposes: it prevents edema formation caused by hypoproteinemia, and it maintains the intravascular fluid volume. Plasma products that contain antibodies to treat or prevent a variety of conditions (including endotoxemia, Rhodococcus equi pneumonia, West Nile virus infection, clostridial diseases, and snake envenomation) are also available. Colloid solutions are available in natural or synthetic forms. Natural colloids are plasma, serum products, or albumin. In general, fresh or fresh frozen plasma is selected when an increase in colloid oncotic pressure is needed, and coagulation factors or specific anticoagulants such as antithrombin III are required. Albumin solutions are not commonly administered to horses, because the intravascular half-life of albumin in diseases with compromised vascular permeability is short. They also do not have the added benefits of whole plasma. Synthetic colloids include dextran and hydroxyethyl starch. The synthetic colloid most commonly administered to horses is hydroxyethyl starch (hetastarch). It is used to increase plasma oncotic pressure, and its effect is best evaluated by clinical response (decreased edema) or increased oncotic pressure (measured by colloid osmometry). A refractometer that measures total protein cannot be used to monitor the effect of synthetic colloid administration.
Rate of Fluid Administration in Equine Emergencies
The goal of fluid therapy for treatment of shock is to rapidly expand circulating blood volume to improve tissue perfusion and oxygen delivery. Isotonic crystalloids should be administered at a dosage of up to 60–80 mL/kg in the first hour (equal to the circulating blood volume) for maximal benefit. This fluid rate, the “shock dose,” should be given in boluses of 6-20 mL/kg (approximately 10 L at a time in a 500 kg horse), and the horse should be reassessed between each bolus to determine whether additional boluses are needed.
Because of the large volumes of BES required, hypertonic fluids or colloids may be given first to immediately support the circulation until the shock dose of crystalloids can be administered. At a dosage of 2–4 mL/kg, hypertonic saline (7.5%) can rapidly expand the circulating volume by redistributing extravascular fluids into the vascular space. Because of redistribution, hypertonic solutions have a short duration of effect (~45 min) in horses. Colloid solutions can be used for a more sustained effect. Hydroxyethyl starch has been reported to increased oncotic pressure for up to 24–36 hours. However, dosages of colloids >10 mL/kg/day have caused coagulopathies. For resuscitation, a combination of hypertonic saline (4 mL/kg) and hetastarch (4 mL/kg) may have the most beneficial and sustained effects.
Route of Fluid Administration in Equine Emergencies
The flow rate of fluids through an administration set is directly proportional to the diameter of the line and inversely proportional to the viscosity of the fluid and the length of the infusion set. Polytetrafluoroethylene or polyurethane 14–gauge catheters are routinely used in horses. A rate of 7 L/hour can be achieved when fluids are >2 feet above the jugular vein, and faster rates can be achieved through gravity flow if the fluid bags are raised even higher. For more rapid flow, 10- or 12-gauge catheters with large-bore connection sets can be used, but large gauge catheters are more thrombogenic. Other ways to increase fluid administration rates include catheterizing both jugular veins or using a pressure bag system or peristaltic pump. Complications of peristaltic pumps are endothelial damage and an increased risk of venous thrombosis.
An alternative route of fluid administration is use of an indwelling nasogastric tube. Case selection is key, and horses that are in shock, are >8% dehydrated, or have positive net gastric reflux are not candidates for oral fluids. Equine electrolyte solutions are preferred, or a homemade mixture can be formulated using 5.27 g sodium chloride, 0.37 g potassium chloride, and 3.78 g bicarbonate per liter of water. The daily fluid rate is divided into boluses and administered using a bilge pump. The horse should be checked for reflux before administration. Volumes <8 L every 2–4 hours are typically well accepted. If a smaller gauge feeding tube is in place, a continuous delivery system from a nonsterile IV set and fluid bags or a carboy can be used, and the rate should be determined in a manner similar to that of an IV infusion rate.
Nasogastric Intubation
Nasogastric intubation is an essential and possibly life-saving procedure performed routinely in cases of equine colic to decompress the stomach and to provide therapy.
After the horse is adequately restrained, the nasogastric tube is passed into the ventral meatus, using the thumb to keep the tube directed correctly. If a hard structure is encountered (eg, the ethmoid or nasal turbinates) and the tube is difficult to pass, the tube should be redirected more ventrally. Once the pharynx is reached, a soft resistance is felt when the tube contacts the larynx and/or esophageal opening. The horse’s head is flexed at the poll, and the tube can be turned 180° so that the curvature of the tube is directed dorsally toward the esophagus. Swallowing is stimulated with gentle pressure against the esophageal opening or by blowing small puffs of air into the tube, and the tube is then passed into the esophagus by coordinating with the swallow reflex.
Methods to identify that the nasogastric tube is in the esophagus include:
negative resistance to suction by mouth
palpation of the nasogastric tube dorsal to the larynx
palpation of the nasogastric tube above the left jugular vein
identification of feed material in the reflux obtained
If the tube is in the trachea, shaking the trachea will result in a “rattle.” If the horse coughs, or if air is noted when suction is applied by mouth, the tube should be withdrawn into the pharynx and the procedure repeated until the tube is correctly positioned. Once the tube is confirmed to be in the esophagus, intermittently blowing into the tube will help to dilate the esophagus and facilitate insertion into the stomach. The tube is advanced into the stomach until level with the twelfth rib. If difficulty is encountered in passing the tube through the cardia, up to 60 mL of mepivicaine (in a 405 kg horse) may be injected into the tube and followed with air or water.
Once the tube is in place, if there is no spontaneous reflux, the stomach should be lavaged. It should not be assumed that any excess fluid in the stomach will drain spontaneously. Medications should never be administered by nasogastric tube without checking first for net reflux. To do so, the tube is filled with ~2 L of water using a pump or funnel with gravity flow to establish a siphon effect, the pump removed, and the end of the tube directed downward to verify the presence of gastric contents. Subtracting the amount of water pumped in from the amount of fluid obtained determines the “net” reflux. Horses should be lavaged with at least 8 L of water to confirm lack of net reflux before any therapy is administered.

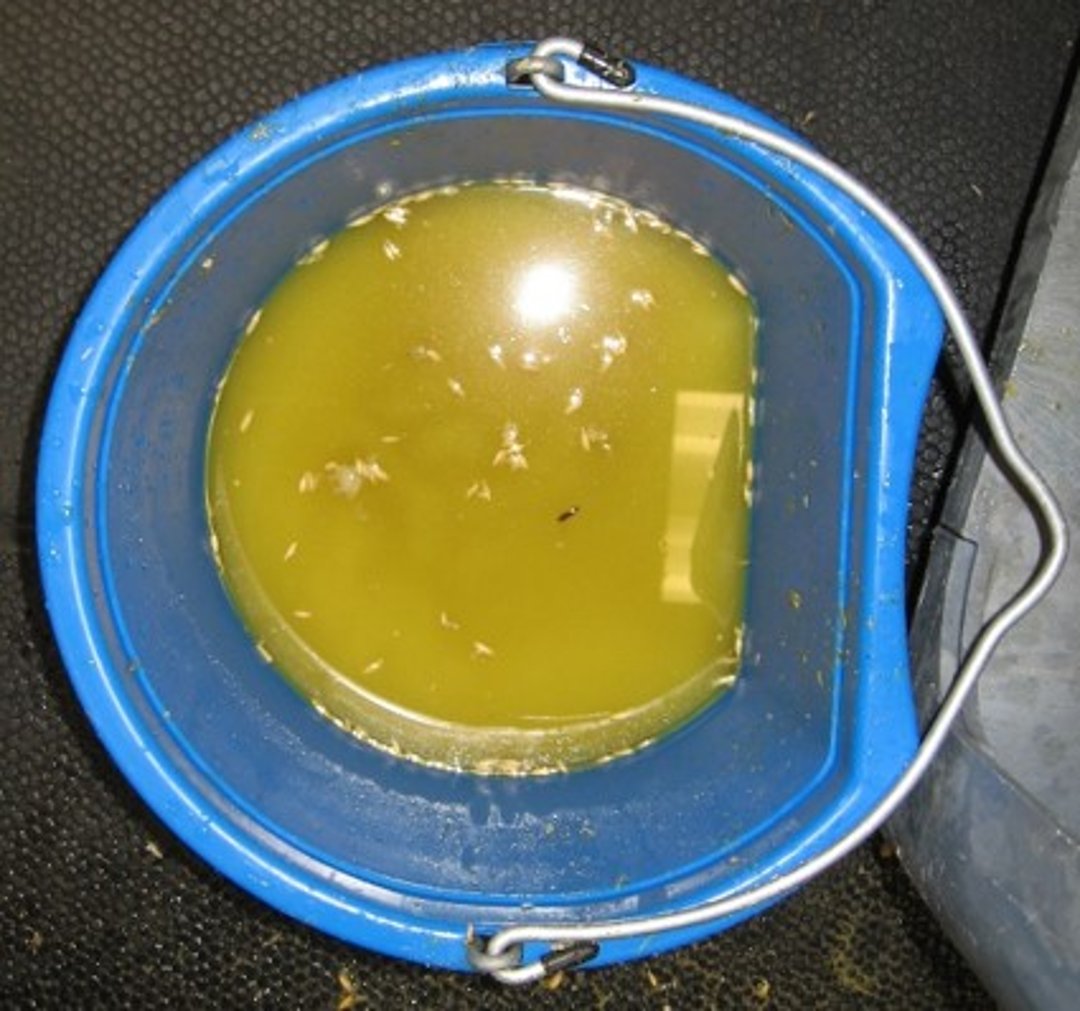
Courtesy of Dr. Amelia Munsterman.
Net nasogastric reflux is not normal. Occasionally, a small amount of reflux (< 1 L) is obtained if a horse has had an indwelling nasogastric tube. In most adult horses with colic, > 2 L net reflux is abnormal. When reflux is obtained, the amount, character, and timing in relation to the onset of colic should be noted, as well as any clinical response to gastric decompression.


Courtesy of Dr. Amelia Munster-man.
Common causes of net gastric reflux include:
small intestinal ileus (functional, mechanical)
obstruction of the small intestine or pylorus
compression of the ileum by a distended ascending colon or cecum
Lesions of the proximal small intestine or pylorus produce large amounts of nasogastric reflux early in relation to the onset of colic. With lesions of the distal jejunum and ileum, there is initially no net reflux, but nasogastric reflux usually becomes productive several hours after the onset of colic. Foul-smelling, fermented, or copious bloody reflux is associated with anterior enteritis and should be treated as a biohazard because of the association of this disease with clostridial and Salmonella spp organisms. With mechanical obstructions, including strangulating lesions and ileal impactions, the reflux is usually composed of feed material and intestinal secretions. However, nasogastric reflux may become hemorrhagic with loss of intestinal viability. Reflux originating from the small intestine is alkaline, whereas reflux composed of gastric secretions is acidic. Because gastric outflow obstruction is rare in horses, pH is usually not measured.
Response to gastric decompression should be noted. Horses with functional ileus show signs of relief, and the heart rate may decrease in response to decompression. Horses with a mechanical obstruction usually remain in pain, although some do respond. The rest of the physical examination of horses with nasogastric reflux should focus on determining whether functional or mechanical ileus is present. The amount of net reflux obtained should be noted after each decompression and the volume of fluids given IV adjusted accordingly. Horses with functional ileus generally need gastric decompression every 2–4 hours. The nasogastric tube should be left in place only as long as required, because it can cause pharyngeal and laryngeal irritation. Esophageal rupture has been described in severe cases.
Abdominocentesis
Abdominocentesis is important in the evaluation of abdominal disease (eg, weight loss, colic, peritoneal effusions, or postoperative complications). It is most commonly used to identify the cause of small intestinal distention and net nasogastric reflux, because large intestinal diseases often do not cause changes in peritoneal fluid in the peracute stage. Ultrasonography can be used to determine the best location to obtain a fluid sample, which can be collected using an 18-gauge needle, a canine bitch catheter, or a teat cannula through a stab incision. Most commonly, the sample is obtained just to the right of midline, caudal to the descending pectoral muscle on the dependent abdomen. This will prevent the site of the abdominocentesis from interfering with a surgical incision if an exploratory laparotomy is needed, and it will also help to avoid puncture of the spleen. The body wall is much thicker off midline, and the length of the instrument used to sample the fluid should be considered. A needle tap should be avoided with severe small-intestinal distention to reduce the risk of bowel puncture and iatrogenic peritonitis. The fluid is collected using sterile technique into a tube with anticoagulant for analysis and into a sterile tube for culture if peritonitis is suspected. It is useful to shake out the EDTA from the tube before sampling, because excess EDTA will falsely increase the total protein measurement.


Courtesy of Dr. Amelia Munsterman.


Courtesy of Dr. Amelia Munsterman.
Normal values for abdominocentesis include a total protein < 2.5 g/dL and WBC counts of < 5,000 cells/μL. Repeated abdominocentesis will not significantly alter these values. On cytology, neutrophils comprise most of the cells; the remainder are lymphocytes, macrophages, and peritoneal cells. With intestinal strangulation, protein increases in the first 1–2 hours. After 3–4 hours of strangulation, RBCs are present, and after ≥ 6 hr, WBCs increase gradually as intestinal necrosis progresses. Degenerate neutrophils will be noted on cytology, and the gross appearance is serosanguinous. Peritoneal lactate is also increased with intestinal ischemia (> 4 mmol/L) and is found to increase over time if serial abdominocenteses are performed.

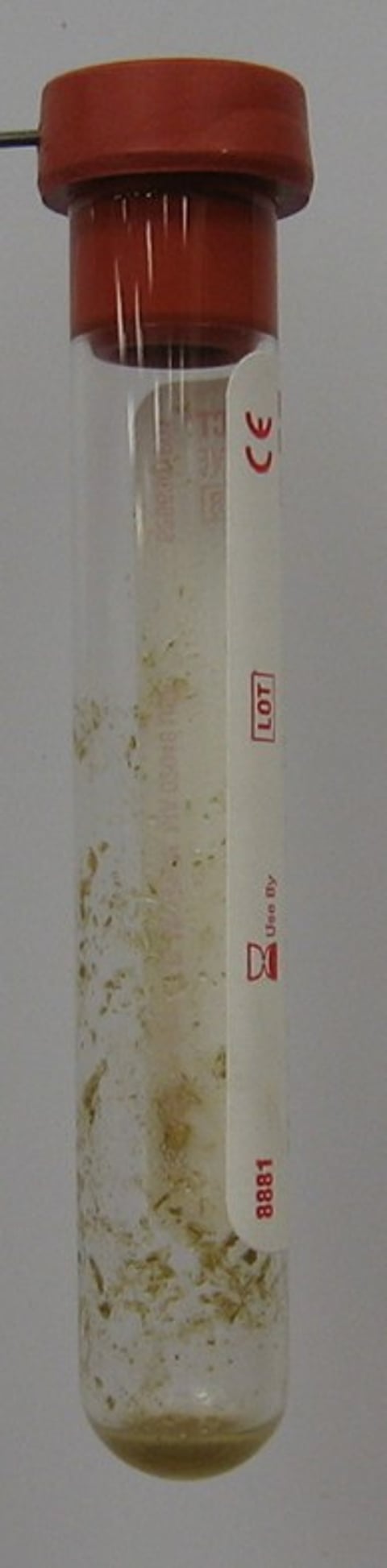
Courtesy of Dr. Amelia Munsterman.
Enterocentesis sometimes occurs, especially in cases of sand colic, and should be differentiated from intestinal rupture. With enterocentesis, cytology reveals plant material, bacteria, and debris, but few cells. The horse’s clinical condition is not consistent with rupture, although in early rupture (~2–4 hours), clinical signs of endotoxemia (eg, depression, tachycardia, congested mucous membranes, signs of shock) may not be seen. Cytology of abdominal fluid compatible with intestinal rupture shows a large number of toxic and degenerate neutrophils, in addition to bacterial organisms, plant material, and bacteria that have been phagocytized by neutrophils. Both enterocentesis and intestinal rupture may demonstrate gross evidence of plant material characteristic of ingesta on visual examination.

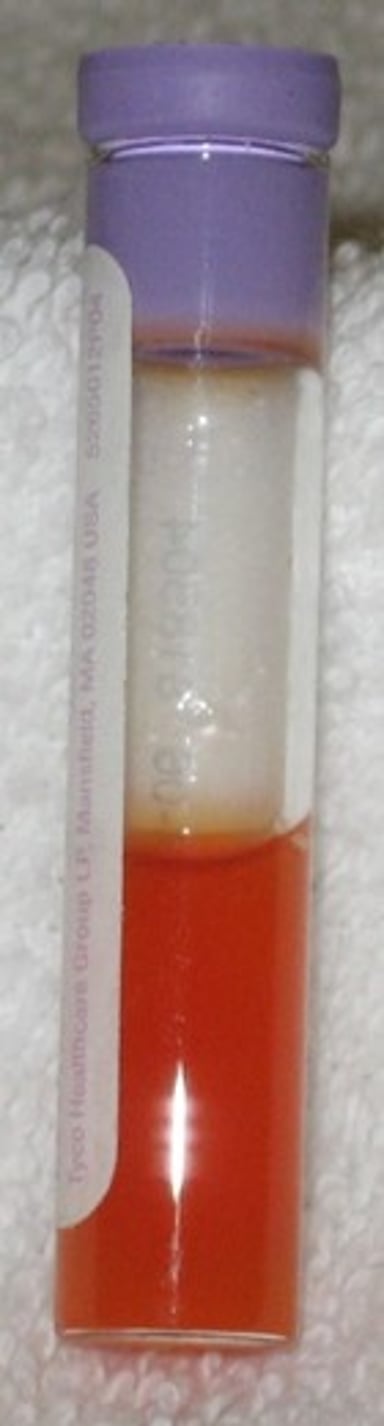
Courtesy of Dr. Amelia Munsterman.
Blood contamination that occurs during the procedure should be differentiated from internal hemorrhage or severely devitalized bowel. Blood from skin vessels or an abdominal vessel usually swirls in the sample and sediments when centrifuged, leaving the sample above the sediment clear. Fresh blood contamination shows platelets on cytological examination, which are not present in blood accumulations >12 hours old. If the spleen is accidentally punctured, centrifugation of the sample reveals a PCV the same or higher than the peripheral PCV. In cases of internal hemorrhage, the blood in the sample is hemolyzed, there are no platelets, and erythrophagocytosis may be seen. When centrifuged, the supernatant will remain reddish. Abdominal ultrasound will reveal fluid swirling in the abdomen. If vascular compromise of the bowel has occurred, hemolysis of RBCs that leak from damaged capillaries will result in a serosanguinous fluid, with a red supernatant after centrifugation.
Abdominal surgery increases the total protein and WBCs in the abdominocentesis. With a sterile peritonitis, the WBC count will remain increased for up to 2 weeks, and cell counts of 40,000 cells/dL have been reported at 6 days after surgery. Neutrophils will appear nondegenerate on cytology, and no bacteria will be observed. The total protein peaks at 6 g/dL 6 days after surgery and may remain increased for 1 month. After an enterotomy, or a resection and anastomosis, degenerate neutrophils and occasional bacteria may be seen in the first 12–24 hours but should resolve in time. If septic peritonitis is present, clinical signs will be consistent with bacterial infection (eg, fever, depression, anorexia, ileus, colic, endotoxemia). The WBC and total protein in the abdominocentesis will be markedly increased. On cytology, >90% of cells are neutrophils and will appear degenerate. Free and phagocytized bacteria are seen. A serum–peritoneal glucose difference >50 mg/dL or a peritoneal fluid pH <7.2 with a peritoneal glucose <30 mg/dL is supportive of a diagnosis of peritonitis.
Trocarization
Trocarization is useful to decompress the abdomen when abdominal compartment syndrome is suspected (increased intra-abdominal pressure resulting in severe abdominal distention, dyspnea, and perfusion abnormalities). Trocarization is performed only for distention of the cecum and large intestine and never to decompress the small intestine or stomach. Thus, it is necessary to identify the segment of intestine involved before the procedure. In adult horses, this is done by transrectal palpation combined with transabdominal ultrasound. Abdominal auscultation may note a “ping” after percussion indicative of a gas-filled organ. In foals or small horses, radiographs and/or ultrasound can be used. The distended segment of the large intestine must also be against the body wall so it can be safely reached by percutaneous trocarization. The most common site for trocarization is the upper right flank, just cranial to the greater trochanter at the location of the cecal base. Ultrasound is used to confirm a gas-filled structure, immediately under the body wall at the chosen site, to avoid puncture of other organs or large blood vessels.


Courtesy of Dr. Amelia Munsterman.
In adult horses, a 14-gauge, 12.5-cm, over-the-needle catheter is typically used, whereas in neonates, a 5-cm 18-gauge needle may be adequate. The area is clipped, sterilely prepared, and infiltrated with a local anesthetic. The catheter is inserted aseptically and attached to a long extension set that is placed in a nonsterile cup of water to monitor progress. Gas released will produce bubbles, and the catheter may be repositioned as the bowel decompresses. A successful trocarization may take >30 min to decompress the bowel passively; the procedure can be shortened by the use of active suction. An antibiotic (usually ~5 mL of gentamicin) is infused subcutaneously as the catheter is withdrawn.
Complications after trocarization may include:
peritonitis
hemorrhage
a local subcutaneous abscess
The horse should be observed for 48 hours for signs of peritonitis, including abdominal pain and fever. Peritonitis is confirmed with abdominocentesis and treated with systemic broad-spectrum antibiotics until it is resolved. Hemorrhage is typically self-limiting, and local abscesses can be drained percutaneously.
Tracheotomy
Tracheotomy is used as an emergency procedure for conditions resulting in acute upper airway obstruction (eg, arytenoid chondritis, snakebite, foreign body). The incision site is selected at the junction of the proximal and middle third of the neck, above the “V” formed by the paired sternomandibularis muscles. If possible, the skin should be clipped, aseptically prepared, and infiltrated with a local anesthetic. In acute respiratory distress, this may not be safely performed, and the procedure is accomplished without sterile preparation.


Courtesy of Dr. Amelia Munsterman.
The initial incision (6–10 cm) is made on the midline, through the skin and cutaneous colli muscle, and then extended between the paired sternothyrohyoideous muscles. Alternatively, the sternothyrohyoideous muscles can be divided on the midline by blunt push-cutting with Metzenbaum scissors. The trachea is exposed, and a transverse incision is made through the mucosa between two tracheal rings, taking care to avoid the tracheal cartilages. The incision will extend to ~30% of the circumference of the trachea. If the horse's head is elevated or extended, the tracheal incision should be made caudal relative to the skin incision, to avoid covering the tracheotomy site when the head is lowered. A J-type silicone tracheotomy tube may be used and secured in place to the mane with gauze. The cuff should not be inflated, unless the horse is to be ventilated, to prevent tracheal necrosis. Alternatively, a self-retaining Pate tracheotomy tube may be preferred because of the tendency of J-tubes to fall out.


Courtesy of Dr. Amelia Munsterman.
The tracheotomy tube should be removed, cleaned, and replaced twice a day or more often if secretions occlude the lumen. Local inflammation and surface-associated infections are common due to the contaminated nature of the procedure (the incision enters the trachea). Attention to postoperative nursing care (cleaning the wound) will reduce the amount of contamination. Petroleum jelly applied to the surrounding skin will also help to reduce skin scalding.


Courtesy of Dr. Amelia Munsterman.
Complications are rare (eg, cartilage deformity, intraluminal granulation tissue, mucosal structure) but can be reduced by removing the tube as soon as possible. One method to determine when the tube can be removed is to temporarily occlude the lumen by hand and observe whether the horse can breathe without it. After tube removal, the site is cleaned with saline twice daily and allowed to heal by second intention. The trachea will generally close in 10–14 days and heal completely in 3 weeks.
Key Points
A fluid challenge with a bolus of balanced electrolyte solution (6-20 mL/kg) can be used to stabilize a hypovolemic patient. Vital parameters, mentation, PCV, total protein, and urine production should be closely monitored, and boluses can be repeated until the clinical signs improve or plateau.
Nasogastric intubation should be provided for every horse presenting with gastrointestinal pain, and volumes of net reflux above 2 L warrant further investigation.
Abdominocentesis is most useful in identification of small intestinal disease, and differentiating between causes of small intestinal ileus.
Trocarization is useful for decompression of the large intestine and cecum and may extend the time available for safe treatment of colic, allowing for successful medical management of abdominal disease.
Tracheotomy is a contaminated procedure; in horses with an upper airway obstruction, surgery should not be delayed to sterilely prepare the incision site.
For More Information
Also see Pet Health content regarding emergency care for horses.