Broken Back
Fracture or dislocation of lumbar vertebrae with compression or severing of the spinal cord is common in both pet and commercial rabbits. The predisposition to a fractured back highlights the importance of adequate and proper restraint skills by the handler. If a rabbit struggles during restraint, it is often best to carefully release the grip and relax the rabbit instead of fighting against the forceful movements of the scared animal. Common signs include posterior paresis or paralysis and urinary and fecal incontinence due to loss of sphincter control. Initial signs of paralysis may resolve within 3–5 days as swelling around the cord diminishes. Supportive therapy includes anti-inflammatory medication to reduce damage from swelling. In acute cases, methylprednisolone sodium succinate might be beneficial. The rabbit should be hospitalized and medical treatment, including pain management, IV fluid therapy, nutritional support, and cage rest should be initiated; with this approach, the severe clinical signs of paraplegia can gradually resolve over 3 months of conservative therapy. Although these cases may appear "hopeless," rabbits can improve to the point of being able to voluntarily move both hindlimbs and to ambulate by walking and hopping. Intense nursing and management are required.
Cannibalism
Young does may kill and eat their young for several reasons, including nervousness, neglect (failure to nurse), and severe cold. Any significant form of stress (eg, dogs or predators entering a rabbitry) can cause nervous does to kill and eat the young. Cannibalism of the dead young occurs as a natural, nest-cleaning instinct. If all management practices are proper and the doe kills two litters in a row, she should be removed from the breeding program or spayed.
Dental Disease


Courtesy of Dr. Joerg Mayer.

Courtesy of Dr. Joerg Mayer.


Courtesy of Dr. Joerg Mayer.
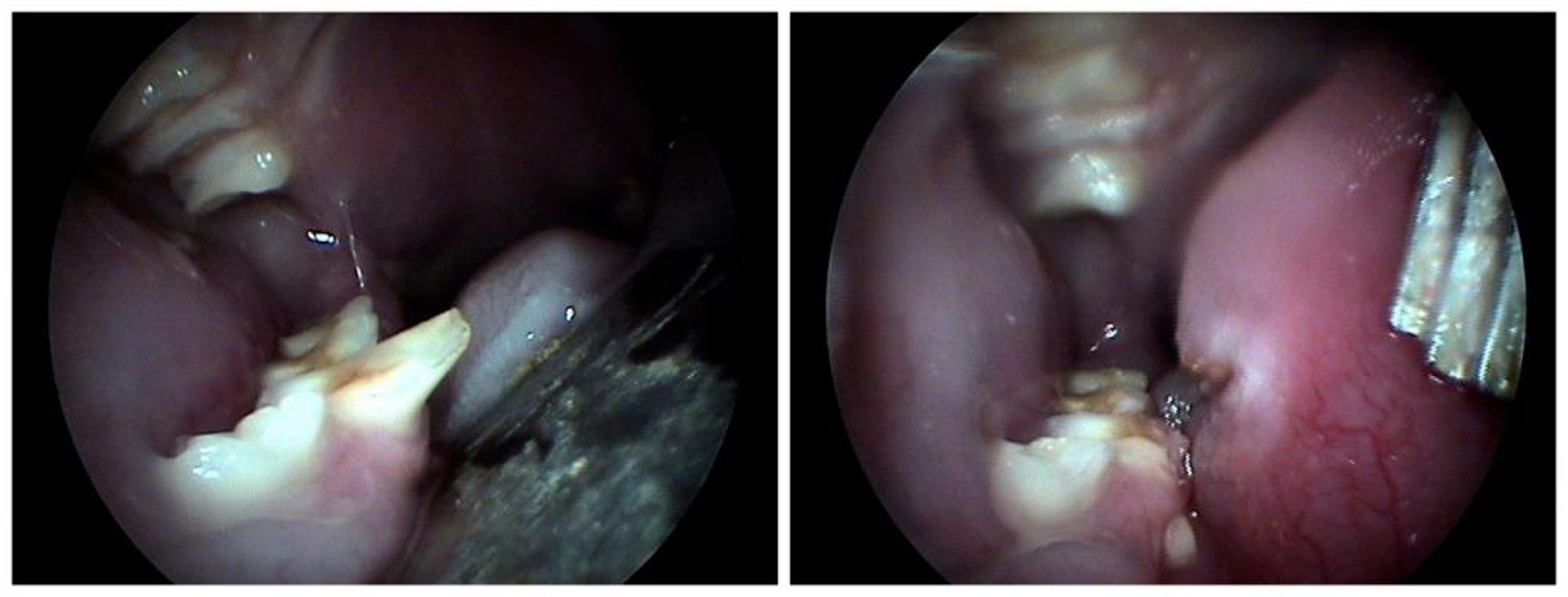
Dental disease may present as excess salivation (slobbers), teeth grinding, or anorexia. Oral examination and palpation along the ventral surface of the jaw should be a part of routine physical examinations of rabbits. Dental abscesses may develop as a consequence of foreign bodies (eg, plant material embedded between the tooth and gum), pulp exposure after tooth trimming, inappropriate diet, or other diseases. Dental abscesses also may appear as retrobulbar abscesses. Hence, a rabbit that presents for primarily ophthalmologic signs such as epiphora or exophthalmus should receive a full dental examination. Rabbit incisors may wear differently depending on diet, and a pelleted diet may predispose the rabbit to dental disease. Multiple teeth are commonly affected. A thorough oral examination under heavy sedation or full anesthesia and diagnostic radiographs are indicated. Often, a skull CT provides significantly more information because of the complexity of the lesions and the 3D structure of the head (which is difficult to fully image with plain radiographs).
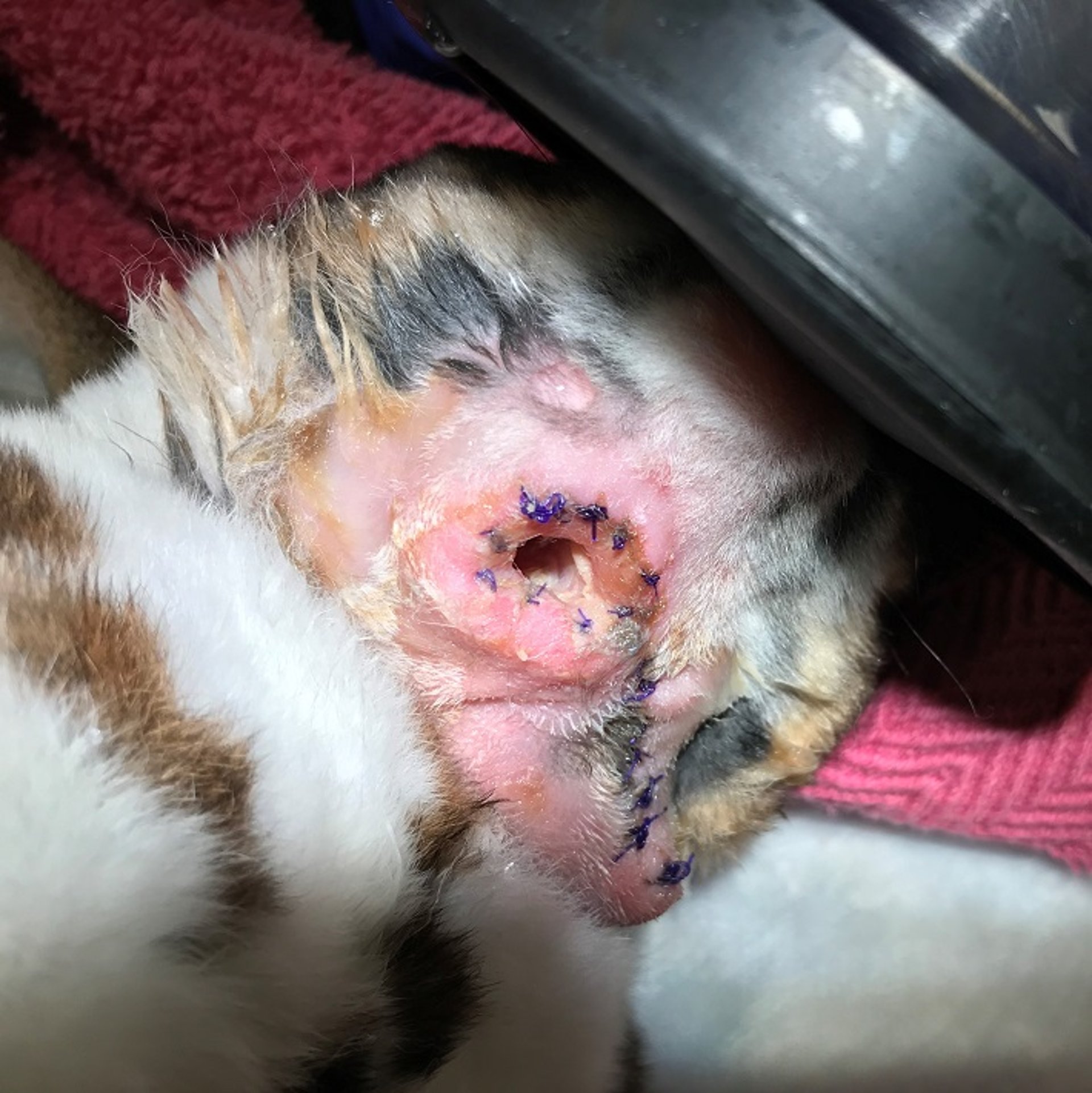
Dental extractions may be accomplished using a fine-tipped dental elevator worked along the root to free the tooth. Incisors are curved and require use of a specialized rabbit incisor luxator or similar curved instrument for removal. Curettage of the alveolus to destroy the apical germinal tissue is required to prevent regrowth of the tooth. Regrowth is unlikely if the pulp remains in the extracted tooth, but followup radiographs in 2–3 months will confirm successful extraction. After lavage, infected sockets can be filled with doxycycline gel or antibiotic-impregnated polymethyl methacrylate (PMMA) beads. PMMA beads are sometimes available from compounding pharmacies or can be self-manufactured. Care has to be taken to choose an antibiotic that is heat stable (eg, gentamicin) in the beads.
Other treatment options following tooth extraction include leaving the surgical site open and marsupializing the skin to allow healing by secondary intention and to facilitate local antibiotic therapy. Antibiotics can be instilled into the open wound by eye drops or by packing the wound with antibiotic-impregnated gauze. Gingival tissues can be sutured closed if needed or can remain open to avoid development of an anaerobic environment. It is important to avoid any cutting of the teeth with wire cutters or even dental pliers. The pressure of such cutters can be transmitted through the tooth and fracture the whole tooth, which will result in further problems. An elongated tooth should always be drilled down by a dedicated dental burr. Defect treatment with calcium hydroxide paste results in tissue necrosis and is contraindicated.
Extraction of cheek teeth involves delicate elevation and luxation if the dental anatomy is normal. Extraction of multiple cheek teeth carries a very poor prognosis for recovery, although some pet rabbits do well with very few molars if the diet is suitably modified. Continued monitoring of the occlusal surface and followup adjustment is expected. Pain management and extended-duration (4 weeks to months) systemic antibiotic therapy based on culture and sensitivity are indicated.
Dental Malocclusion in Rabbits
The incisors, premolars, and molars of rabbits grow throughout life. The normal length is maintained by the wearing action of opposing teeth. Malocclusion (mandibular prognathism, brachygnathism) probably is the most common inherited disease in rabbits and leads to overgrowth of incisors with resultant difficulty in eating and drinking. Overgrowth or malocclusion of the cheek teeth is usually due to malnutrition or other mistakes in husbandry. If overgrowth or malocclusion of the cheek teeth is present, the incisors will eventually also be impacted. Because normal occlusion of the mouth is no longer possible, the self trimming of the incisors does not occur. Dental trimming is often done with combined anesthesia of diazepam (1–5 mg/kg, IM) followed by or in combination with ketamine (10–20 mg/kg, IM), or a combination of ketamine and dexmedetomidine ( see Surgery).


Courtesy of Dr. Joerg Mayer.

Courtesy of Dr. Joerg Mayer.
Occasionally, the cheek teeth overgrow and cause severe tongue or buccal lesions. Cheek teeth malocclusion is generally considered to be related to husbandry issues (eg, inadequate nutrition), rabbits with this condition should be thoroughly assessed regarding their husbandry. For example, young rabbits can damage their incisor teeth by pulling on the cage wire, which results in misalignment and possibly malocclusion as the teeth grow. This condition is difficult to differentiate from genetic malocclusion, and these rabbits should also not be bred. Genetic malocclusion generally can be detected in rabbits 3–8 weeks old, whereas malocclusion due to husbandry will often take much longer to develop. If incisors are suddenly overgrown in an adult rabbit, it is not enough to trim the incisors down. The problem commonly originates in the back of the mouth, and a full assessment of the cheek teeth is warranted. The dental procedure needs to be done under full anesthesia and with special equipment. Rabbit dentistry is very different from that in dogs and cats because of the differences in anatomy and physiology. Special training and literature about rabbit dentistry is readily available, and dental procedures in rabbits should be performed only by those with specific training.
Gastric Stasis, Hair Chewing, and Hairballs
The GI tract of the rabbit is similar to that of the horse, with an anatomy and physiology that often leads to clinical complications. One of the most frequent presentations is gastric stasis, which has a variety of causes, including stress and/or pain. The initial phase of the problem commonly goes unrecognized by the owner or untrained veterinarian. Because they are a prey species, rabbits do not overtly show signs of discomfort or pain and remain quiet and inactive. Rabbits are commonly presented in an advanced state of stasis that has already led to dehydration, pain, and hepatic lipidosis. Decreased food intake has a large impact on the health of rabbits and affects many other factors of homeostasis. When food intake is decreased, water intake is also commonly decreased. The GI contents lose the typical slurry-like consistency and become pasty. As the rabbit becomes dehydrated, water is absorbed from the GI tract into the vascular space, which masks the typical hematologic signs of dehydration (eg, no increase in PCV). A decrease in energy uptake will produce hepatic lipidosis relatively quickly in rabbits, which in turn decreases food intake. It is of utmost importance to realize the seriousness of the condition and to counteract the downward spiral.
Rabbits groom themselves constantly, so the stomach contents often contain hair. When the GI contents are of normal, slurry-like consistency, the hair normally passes through the GI tract and is excreted with the fecal pellets. A high-fiber diet helps to create a fiber mesh that prevents the GI contents from becoming too dense so that hair can more easily pass through the upper GI tract along with the mesh of fiber. Hair chewing is generally a result of low fiber in the diet and can be corrected by increasing the fiber or feeding hay along with the pellets. Adding magnesium oxide to the diet at 0.25% also may be helpful. In some cases, hair chewing is a result of boredom because of lack of fiber or chew substrate. Providing environmental enrichment often halts this behavior.
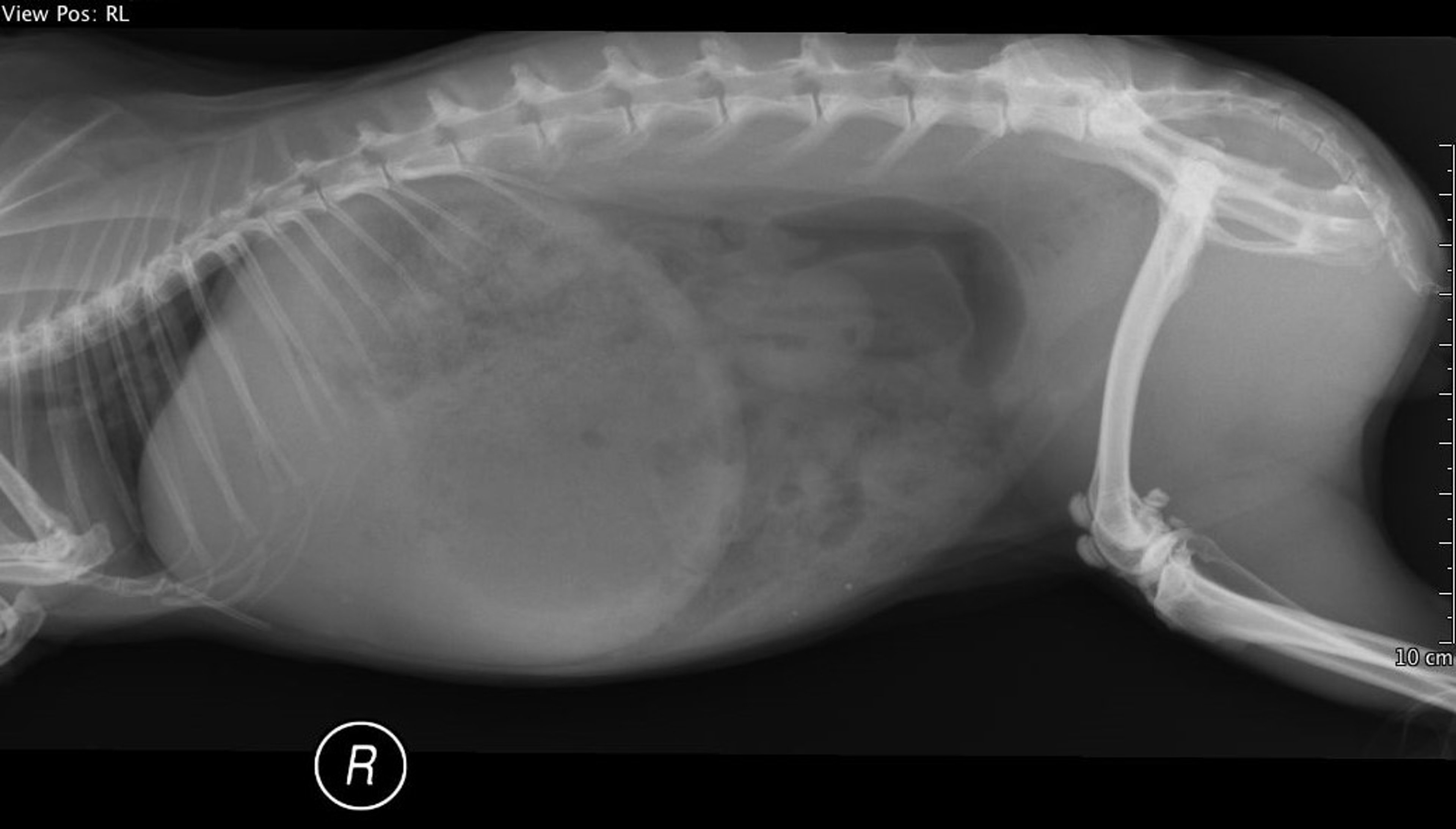
The hair becomes a problem only if excess amounts are consumed or if it accumulates in the stomach and blocks the pylorus. If this happens, the rabbit becomes anorectic, loses weight, and dies within 3–4 weeks. Premortem diagnosis of pyloric obstruction can be difficult, because palpable hairballs can be an incidental finding and radiography is often nondiagnostic. Because rabbits will usually chew their food significantly, GI foreign body obstructions are not as frequent as with carnivores or omnivores. The radiologic signs of a GI obstruction are often similar to the typical pattern (eg, increased lumen of a small GI loop). The most common site of a possible obstruction is the proximal duodenum, because the diameter of the lumen suddenly decreases significantly. The second most common site is the ileocecal valve (sacculus rotundus), because this is a structure that works as a unidirectional valve to prevent GI contents from moving from the cecum back into the small intestine. The diagnosis of this obstruction is commonly made by ultrasonography.
Once GI stasis affects the emptying of the stomach, gas accumulation creates further visceral distention and pain (ie, colic presentation). The resulting decreased food intake and GI hypomotility cause an increased cecal pH and altered cecal microflora, creating cecal dysbiosis. Alterations in water and electrolyte balance result in systemic ketoacidosis and hepatic lipidosis. Gastric ulceration and even gastric rupture may occur.

Courtesy of Dr. Joerg Mayer.
The goals of treatment are to:
remove the obstruction
stimulate motility
restore GI microorganism balance
relieve dehydration and anorexia
Most cases can be managed by aggressive fluid management (maintenance is 100–120 mL/kg/24 hr), with affected rabbits receiving double the rate of maintenance fluids (10 mL/kg/hr) IV. Pain medication (eg, oxymorphone or hydromorphone, 0.2 mg/kg every 4–6 hours) is essential to relieve the GI discomfort. With aggressive fluid and pain management, the rabbits usually feel better within 24 hours. Because the GI tract is either full or distended with contents, oral force feeding should be discouraged. Energy can be provided by adding dextrose to the IV fluids. Food should be available at all times and in different forms (eg, hay, vegetable matter, supportive care formula). Rabbits often start to eat on their own after they are properly hydrated and received analgesia for visceral pain. If the rabbit does not eat because of advanced stages of hepatic lipidosis, assist syringe feeding should be started. Once a true GI obstruction has been excluded, treatment can then include a motility stimulant such as metoclopramide (0.5 mg/kg, PO or SC, three to four times daily) or cisapride (0.5 mg/kg, PO, two to three times daily); however, this should not be started before hydration and pain management. Reestablishment of GI microflora may be assisted by probiotic treatment or cecotrophs from healthy rabbits.
Mineral oil and laxatives do not effectively remove the hair mass. Roughage (hay or straw) should be fed during the treatment to help carry the hair fibers through the GI tract and out with the feces. Surgical treatment should be considered only if medical management has not resulted in improvement.
Prevention of GI stasis is the best option and can be accomplished by providing a high-fiber diet, avoiding stress and obesity, providing environmental enrichment, and combing daily to remove loose hair. Rabbits also consume significantly more water when offered by bowl vs sipper bottle. Clinical research does not support routine doses of mineral oil, wetting agents, or proteolytic enzymes as effective preventives.
Liver Lobe Torsion


Courtesy of Dr. Joerg Mayer.

Courtesy of Dr. Joerg Mayer.
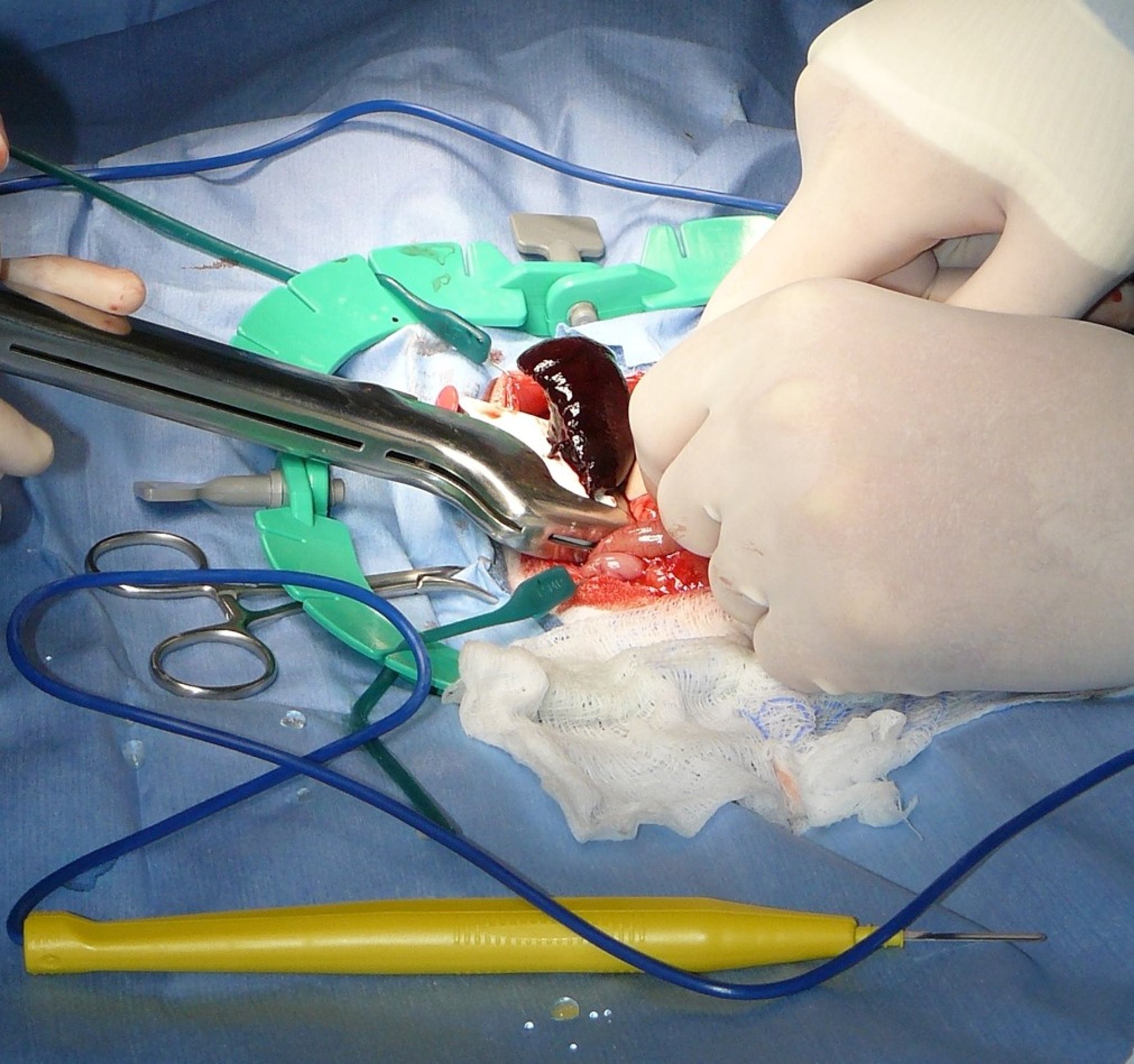
Liver lobe torsions in rabbits can be observed as a sudden, peracute condition. The rabbit will present with cranial abdominal pain and be anorectic. It is important to diagnose this condition rapidly, because the liver lobe is cut off from circulation, and subsequent endotoxin release can be fatal. Diagnosis is by ultrasonography of the liver, specifically the caudate lobe. If a lack of blood flow is detected, immediate surgery is indicated. Computed tomography is also a useful means of diagnosis. The prognosis for these cases is directly correlated with the speed of detection of the condition.
Heat Exhaustion
Rabbits are sensitive to heat. Hot, humid weather, along with poorly ventilated hutches or transport in poorly ventilated vehicles, may lead to the death of many rabbits, particularly pregnant does. Affected rabbits stretch out and breathe rapidly. Hutches should be constructed so that they can be sprinkled in hot, humid weather. Free access to cool water should be provided. When the environment can be controlled, optimal conditions are a temperature of 50°–70°F (15.5°–21°C) and a relative humidity of 40%–60%, with 10–20 air changes/hour. As a rule of thumb, the sum of the temperature in Fahrenheit and the humidity in percent should not be over 150. For example, a temperature of 80°F with a humidity of 80% would be 160 and therefore not appropriate for a rabbit. Wire cages are preferable to solid hutches. Treatment consists of immersing rabbits in cold water during the heat of the day, especially those that will kindle in the next day or two. Breeding bucks may lose a majority of viable sperm and might not breed successfully for several weeks until new sperm production replaces the sperm killed by thermal stress.
Hutch Burn

Courtesy of Dr. Joerg Mayer.

Courtesy of Dr. Joerg Mayer.
Prolonged irritation of the bladder mucosa with calcium sediment can cause a cystitis that can manifest in incontinence and soiled fur ( see Urolithiasis). A wet perianal area often causes additional problems such as fly strike and dermatitis. This condition is often referred to as hutch burn, Hutch burn is often confused with treponematosis and can be truly differentiated only by the absence of spirochetes on darkfield microscopy and by the lack of antibodies to Treponema paraluiscuniculi. It is caused by wet and dirty hutch floors and affects the anus and external genitalia. Also, rabbits that lack adequate sphincter control of the bladder constantly dribble urine and may be affected. The membranes of the anus and genital region become inflamed and chapped. The area soon becomes secondarily infected with opportunistic pathogenic bacteria. Brownish crusts cover the area, and a hemorrhagic, purulent exudate may be present. Keeping hutch floors clean and dry and applying nitrofurazone or an antibiotic ointment to the lesions hastens recovery.
Ketosis
Ketosis is a rare disorder in rabbits that may result in death of does at or 1–2 days before kindling. The condition is more common in first-litter does. Predisposing factors include obesity and lack of exercise. The probable cause is starvation. Other signs are dullness of eyes, sluggishness, respiratory distress, prostration, and death. The most significant lesions are fatty liver and kidneys. The body mobilizes fat and transports it to the liver to be broken down for energy, thus the fatty liver. Diagnosis depends on a detailed history and physical examination and clinical signs. A key clinical sign is clear urine; the urine of healthy rabbits is usually cloudy. Injection of fluids that contain glucose and assisted syringe feeding may help correct the disorder.
Moist Dermatitis
Female rabbits have a heavy fold of skin on the ventral aspect of the neck. As the rabbit drinks, this skin may become wet and soggy (“slobbers”), which leads to inflammation. Contributing factors include dental malocclusion, open water crocks, and damp bedding. The hair may slip, and the area may become infected or flyblown. The area often turns green if infected with Pseudomonas spp. Automatic watering systems with drinking valves generally prevent wet dewlaps. If open water receptacles are used, they should have small openings or be elevated. Once the area is infected, the hair should be clipped and antiseptic dusting powder applied. In severe cases, parenteral antibiotics and analgesics are necessary.
Ophthalmologic Disease
Corneal ulceration is the most common ophthalmic problem of rabbits. Rabbits appear predisposed to this condition for two main reasons:
the globe and surface of the cornea are significantly larger in rabbits than in most other domesticated pets
rabbits do not blink as frequently as other species, which leaves the cornea less moist
Many potential underlying issues should be excluded, although environmental causes and trauma are the most frequent causes. The cornea should be carefully protected during anesthetic procedures. The lack of tear production associated with keratoconjunctivitis sicca or dry eye may further increase the risk of corneal damage. Exophthalmia as a result of orbital or dental disease or facial paralysis associated with encephalitocytozoonosis can make blinking difficult and lead to corneal damage.
Superficial ulcers can be treated with broad-spectrum ophthalmic antibiotic solutions. Treatment progress should be assessed in 1–2 days. Epithelial "lips" indicate a nonhealing ulcer. Such ulcers should be debrided after application of a topical anesthetic, followed by the same treatment as for a superficial ulcer. If the ulcer does not respond to topical treatment, collagen shields or even contact lenses have been used successfully. In severe cases, surgery and placement of a conjunctival pedicle graft may be required. Differential diagnoses of corneal lesions in rabbits include corneal occlusion (overgrowth of conjunctival tissue) and limbic or corneal dermoid (skin-like tissue in an abnormal location over the cornea). Hair may protrude from a limbic dermoid. These growths do not appear painful.
Pseudopterygium, an aberrant growth of conjunctival membrane tissue, is sometimes seen in rabbits. The cause is not known, and the condition is slowly progressive. The conjunctival membrane extends from the bulbar conjunctiva and slowly grows onto the cornea, giving the eye an opaque appearance. Surgical removal of the overgrown conjunctiva is straightforward but leads to recurrence. Daily administration of topical cyclosporine 0.2% in the affected eye might help slow down recurrence.
Phacoclastic uveitis secondary to Encephalitozoon cuniculi ( see Encephalitozoonosis) has been recognized to present as iridal swelling and white or pink nodules on the iris. The nodules are bacterial iridal or corneal stromal abscesses and give the typical appearance of cotton candy in the anterior chamber. Spores replicating in the lens may result in cataract formation and even lens rupture, leading to a painful uveitis. Diagnosis is confirmed by presence of the organisms on histopathology of excised tissue or DNA probe on removed lens material. Treatment involves lens removal by phacoemulsification or enucleation. Spontaneous lens regeneration may occur. Prosthetic lens insertion is not recommended. The prognosis is guarded without surgery; glaucoma develops in most affected rabbits. Topical treatment includes NSAIDs and mydriatic and antibiotic medications. After starting topical medications, progress and intraocular pressure should be checked in 5–7 days. Monitoring should continue every 2–3 weeks for the next 2 months. Systemic therapy for Encephalitozoon should be started.
Inherited glaucoma is discussed below ( see Buphthalmia).
Ulcerative Pododermatitis

Courtesy of Dr. Joerg Mayer.


Courtesy of Dr. Louise Bauck.
Ulcerative pododermatitis does not involve the hock but the plantar surface of the metatarsals and, less commonly, the volar surface of the metacarpal-phalangeal region. The cause is either pressure on the skin from bearing the body weight on wire-floored cages or trauma to the skin from stamping, with secondary infection of the necrotic skin. Several factors, including accumulation of urine-soaked feces, nervousness, posterior paralysis after a spinal cord injury, and the type of wire used, may influence development. Genetics are also involved. The Rex appears to be predisposed because of the lack of the longer guard hairs that usually act as a cushion over the predisposed area of the hock. Heavy-breed rabbits such as the Flemish Giant and the Checkered Giant are also susceptible.
Affected rabbits sit in a peculiar position with their weight on their front feet; if all four feet are affected, they tiptoe when walking. Various debriding agents can be used to clean the lesion, followed by topical antibiotic treatment along with parenteral antibiotics. Radiographs exclude osteomyelitis with severe lesions. The rabbit must be removed from the cage or given a solid floor (board or mat) on which to sit or rest. Treatment is often difficult and time consuming, with application of bandages that need frequent changing. Low-level laser therapy has shown some benefits as a treatment. Husbandry improvement should focus on providing soft, dust-free bedding. In many cases, weight management is also indicated. Because large feet and thick footpads are hereditary, selection of breeding stock for these traits has reduced the incidence of pododermatitis.
Urolithiasis
Courtesy of Dr. Katherine Quesenberry.
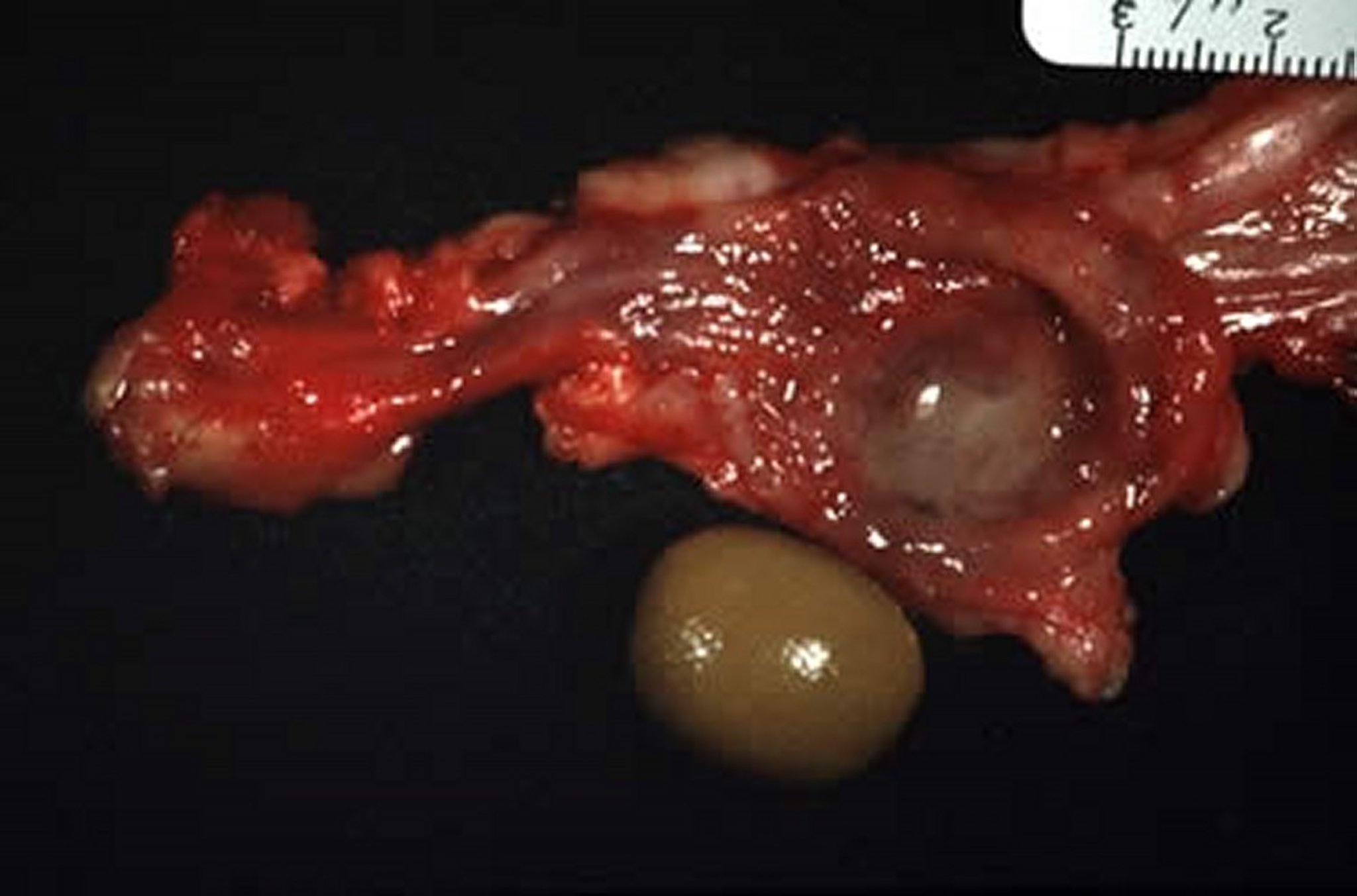
Urolithiasis is seen routinely in pet rabbits and occasionally in commercial rabbitries. It is generally suspected when hematuria is seen. (A dipstick can quickly exclude normal pigment causes of red urine.) The rabbit's calcium metabolism is significantly different from that in other vertebrates. Rabbits do not require vitamin D3 to absorb calcium from the gut into the bloodstream. The vast majority of dietary calcium is readily absorbed into the bloodstream, leading to relatively higher blood calcium levels (up to 16 mg/dL [4 mmol/L] can be normal). Renal elimination of calcium is much higher in rabbits (as high as 60%) than in other vertebrates (2%–5%). This often gives the urine a cloudy appearance, which is normal. Feeding a calcium-rich diet for a prolonged time to a metabolically inactive rabbit (ie, not growing, pregnant, or lactating) can lead to an abnormal hypercalciuria, and calcium can precipitate out as bladder sludge or form uroliths. Small stones are often voided, but surgery is frequently needed to remove larger urinary stones.
Uroliths are caused by calcium carbonate and triple phosphate crystals precipitating out of normal urine when the pH increases to 8.5–9.5. Normal rabbit urine has an average pH of 8.2. Several factors have been incriminated in urolithiasis, including nutritional imbalance (especially the calcium:phosphorus ratio), genetic predisposition, infection, inadequate water intake, and metabolic disorders. Short-term treatment involves surgically removing the uroliths, whereas longterm treatment focuses on reducing dietary calcium intake. Because alfalfa is high in calcium and one of the main dietary components of regular rabbit pellets, switching to timothy-based pellets and to grass or timothy hay and rolled oats helps to prevent recurrence.
Heritable Diseases
Buphthalmia in Rabbits
Buphthalmia is an autosomal trait with incomplete penetrance that results in variable clinical severity. Intraocular pressures begin to rise as early as 3 months. One or both eyes may be affected. Glaucoma can be treated medically (dorzolamide 2%; 1 drop three times daily) or by surgical enucleation. Affected rabbits should not be bred.
Splay Leg in Rabbits
Splay leg is presumed to be an inherited disorder presenting with abduction of one or more legs as early as 3–4 weeks of age. The right rear limb is most commonly affected, although the condition may be unilateral or bilateral. Hip dysplasia can occur during postnatal development among rabbits housed on slick nest boxes or flooring.
Neoplasia
By far, the most common tumor in rabbits is uterine adenocarcinoma of intact females. The incidence can be as high as 60% in intact does >3 years old. The disease may present with multicentric tumors that involve both horns of the uterus. The masses can often be palpated as globular polypoid structures. The tumor often metastasizes to the liver, lungs, and other organs; cystic mastitis may develop concurrently. This disease is the primary reason to recommend spaying of nonbreeding female rabbits at the age of 4–6 months.
Lymphoma and other neoplastic disorders of lymphoid tissue are common tumors that occur in all ages of pet rabbits. Malignant lymphomas (lymphosarcoma) are relatively common and may occur in rabbits < 2 years old. The manifestation can be extremely varied, ranging from ocular lesions, to skin, to leukemic forms. Lymphosarcoma presents with a tetrad of lesions, including enlarged kidneys, splenomegaly, hepatomegaly, and lymphadenopathy. Treatment of lymphoma can be attempted by chemotherapy, but prognosis is often poor due to the often aggressive form of the disease. Rabbits can be treated with "typical" chemotherapeutic agents, and adverse effects to these drugs appear less common than in other domesticated pets.

Courtesy of Dr. Joerg Mayer.
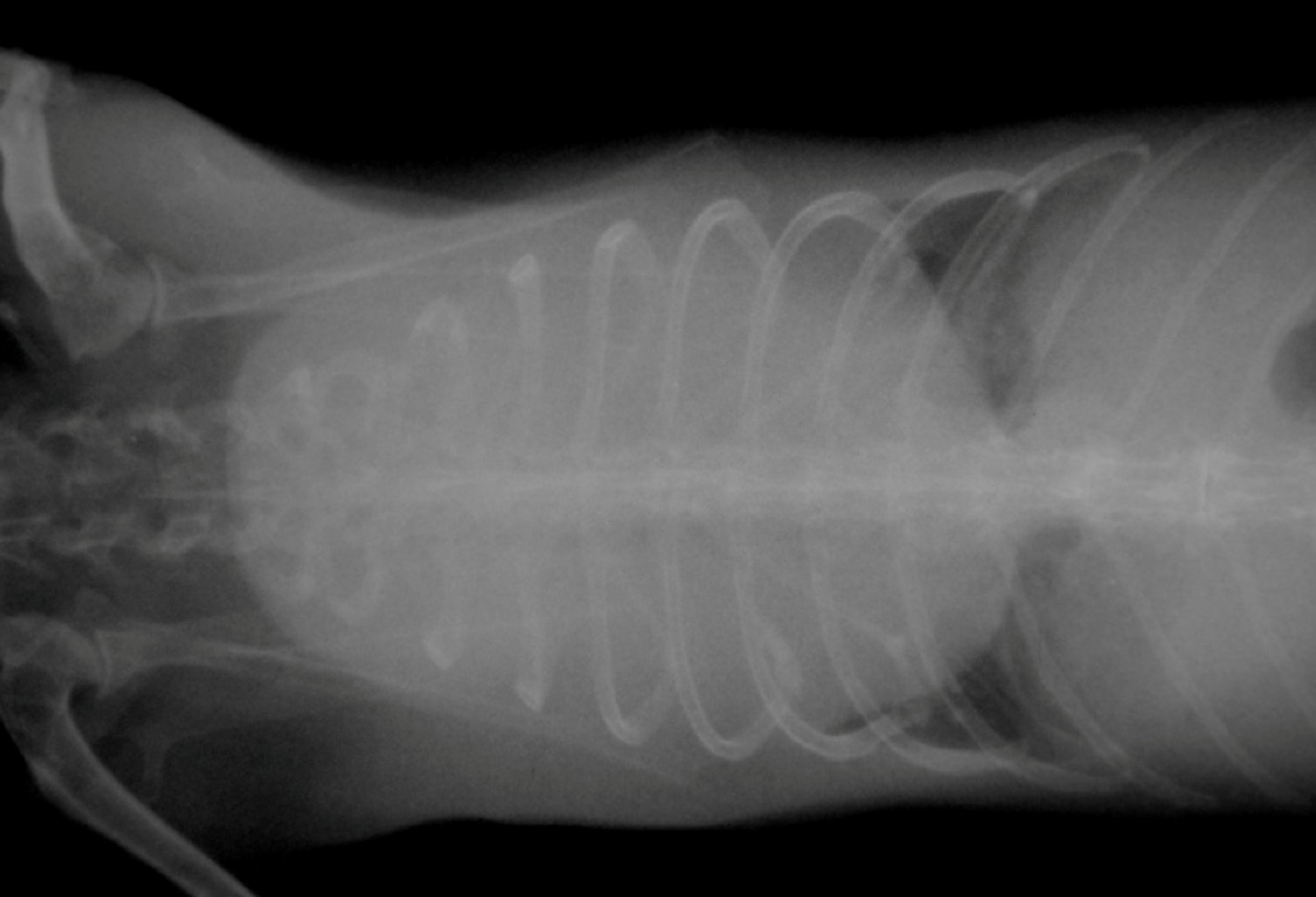
Thymoma and thymic lymphoma are the most common mediastinal masses in rabbits. Differentiation between the two is difficult and usually requires a fine-needle aspirate or a biopsy of the chest mass. The typical clinical sign for a chest mass in rabbits is intermittent or permanent exophthalmos. Because of the impaired venous return from the head through the chest, the venous sinuses behind the globe expand and cause the exophthalmos. A chest radiograph to scan for masses should be performed in all rabbits with exophthalmos. The thymoma can sometimes be removed surgically relatively easily, because it does not involve other major structures in the chest cavity. In the case of thymic lymphoma, surgery is often less successful, because the structure is often not possible to be removed in toto. Radiation of the thorax has been described as an effective therapy, and animals have survived for years after the treatment. If no advanced therapy is an option, oral prednisolone (1mg/kg, PO, once to twice daily) has been used in a few cases with success.
Cardiovascular Disease
With pet rabbits living to be significantly older than a few years ago, cardiovascular disease is increasingly diagnosed. Anatomically there are a few differences in the rabbit heart compared with other mammals, which makes them a bit more sensitive to cardiac problems. For example, the myocardium has a very limited collateral circulation, which could lead to sudden death during an ischemic event. A variety of myocardial, valvular, and vascular diseases have been described in rabbits. It is beyond the scope of this reference to discuss the diagnosis and treatment of each condition in detail.
The basic concepts for other species regarding diagnosis and therapy of cardiovascular diseases should be used as a foundation. Often, drug dosages can be extrapolated from canine and feline dosages as a starting point. Often, higher doses may be needed if the starting dose does not resolve or improve the condition. This is in line with metabolic scaling. Based on this, an accurate diagnosis is of utmost importance when treating a rabbit for cardiovascular disease.
Normal radiographic anatomy and normal ECG values have been published, which makes the evaluation of the rabbit heart fairly standard. Rabbits also produce the enzyme atropinase, which makes the use of atropine in cases with arrhythmias less effective. Instead, glycopyrrolate should be used to increase the heart rate in rabbits with bradycardia or as a premedication for surgery.
For More Information
Feldman ER, Singh B, Mishkin NG, Lachenauer ER, Martin-Flores M, Daugherity EK. Effects of Cisapride, Buprenorphine, and Their Combination on Gastrointestinal Transit in New Zealand White Rabbits. J Am Assoc Lab Anim Sci 2021;60(2):221-228.