Fowlpox is a worldwide viral infection of chickens and turkeys. Nodular lesions on unfeathered skin are common in the cutaneous form. In the diphtheritic form, which affects the upper GI and respiratory tracts, lesions occur from the mouth to the esophagus and in the tracheal mucosa. Diagnosis is by observing characteristic gross and microscopic lesions and by PCR assay to detect the fowlpox virus-specific genes. Vaccination can prevent the disease and limit spread in affected flocks.
Fowlpox is a slow-spreading viral infection of chickens and turkeys. Fowlpox is an economically important disease of commercial poultry.
Etiology of Fowlpox
The etiologic agent of fowlpox is the fowlpox virus, the type virus of the genus Avipoxvirus in the family Poxviridae.
Classification of viral genome: Fowlpox virus has a large (~ 300 kb), linear double-stranded DNA genome with a hairpin loop at each end, encoding > 200 genes (including for DNA polymerase, NTPaseI, uracil glycosylase, and thymidine kinase) expressed in different temporal classes: immediate, early, and late.
Field strains associated with outbreaks and vaccine strains show differences in their genomic profiles, although the strains can be differentiated to some extent by restriction endonuclease analysis, nucleotide analysis of specific genes, and immunoblotting. Molecular analyses of vaccine and field strains of fowlpox viruses have shown noteworthy differences.
Structure: Avipoxviruses have complex, multilayered virions. The brick-shaped capsid measures ~330 × 280 × 200 nm and is enveloped by one or more membranes enclosing a biconcave core that contains the genome in a nucleoprotein complex (see Fowlpox virus lesion).

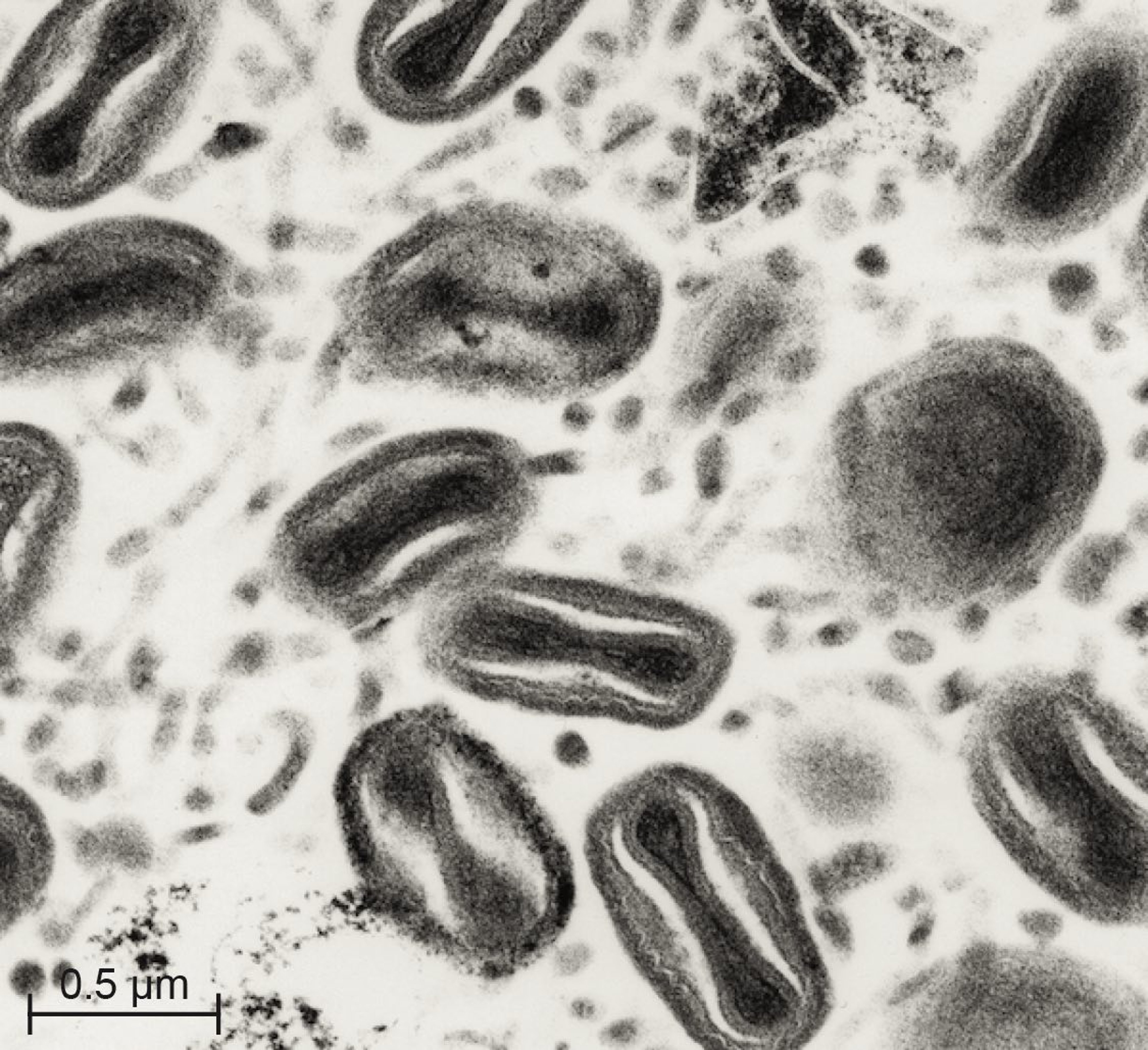
Courtesy of Dr. Deoki Tripathy.
Replication: For entry, the virus binds to glycosaminoglycan receptors on the host cell surface.
In common with other poxviruses, fowlpox virus replicates in cytoplasm. Avian poxviruses form extracellular enveloped virus directly by budding of mature virions through the plasma membrane.
Pathogenic mechanisms: The large DNA virus present in fowlpox lesions (an in the Poxviridae family) is resistant to normal environment and may survive for extended periods in dried scabs. Photolyase and A-type inclusion body protein genes in the genome of fowlpox virus appear to protect the virus from environmental insults.
Avian poxviruses may be sequestered within inclusion bodies.
Epidemiology of Fowlpox
Incubation period:The incubation period for fowlpox in chickens and turkeys is typically 4–10 days.
Morbidity and mortality: Cutaneous infections alone ordinarily cause low or moderate mortality rates, and these flocks generally return to normal production after recovery. Mortality rates are usually high in diphtheritic or systemic infections by some virulent strains.
Geographic distribution: Fowlpox is present worldwide.
Host range: Fowlpox virus affects mainly chickens and turkeys and has been reported to infect ducks, geese, pheasants, quail, canaries, and hawks. Mammals are not susceptible to natural infection with fowlpox virus or any of other avipoxviruses.
Transmission: The virus is usually transmitted by contact through abrasions of the skin.
Skin lesions (scabs) shed from recovering birds in poultry houses can become a source of aerosol exposure for susceptible birds. Mosquitoes and other biting insects may serve as mechanical vectors. Transmission within a susceptible flock is rapid when mosquitoes are plentiful.
The disease tends to persist for extended periods in multiple-age poultry complexes because of slow spread of the virus and availability of susceptible birds.
Clinical Findings of Fowlpox
Fowlpox occurs in different clinical forms. Fowlpox in chickens and turkeys is characterized by proliferative lesions in the skin that progress to thick scabs (cutaneous form) and by lesions in the upper GI and respiratory tracts (diphtheritic form). Virulent strains may cause lesions in the internal organs (systemic form).
The cutaneous form of fowlpox is characterized by nodular lesions on various parts of the unfeathered skin of chickens and on the head and upper neck of turkeys. Generalized lesions of feathered skin may also occur. In some cases, lesions are limited chiefly to the feet and legs.
The lesion is initially a raised, blanched, nodular area that enlarges, becomes yellowish, and progresses to a thick, dark scab. Multiple lesions usually develop and often coalesce. Lesions in various stages of development may be found on the same bird.
Localization around the nostrils may cause nasal discharge. Cutaneous lesions on the eyelids may cause complete closure of one or both eyes. Only a few birds develop cutaneous lesions at one time. Lesions are prominent in some birds and may substantially decrease flock performance.


Courtesy of Dr. Jean Sander.


Courtesy of Dr. Jean Sander.


Courtesy of Dr. Jean Sander.
In the diphtheritic form of fowlpox, lesions develop on themucous membranes of the mouth, esophagus, pharynx, larynx, or trachea (wetpox or fowl diphtheria). Occasionally, lesions occur almost exclusively in one or more of these sites.
Caseous patches firmly adherent to the mucosa of the larynx and mouth, or proliferative masses may develop. Mouth lesions interfere with feeding. Tracheal lesions cause difficulty in respiration. Laryngeal and tracheal lesions in chickens must be differentiated from those of infectious laryngotracheitis, which is due to a herpesvirus that produces intranuclear inclusions.
In cases of systemic infection due to virulent fowlpox virus strains, lesions may be present in internal organs. More than one form of the disease (cutaneous, diphtheritic, or systemic) may occur in a single bird.
Often, the course of the disease in a flock is protracted (2–8 weeks). Extensive infection in a layer flock results in decreased egg production.
Diagnosis of Fowlpox
Characteristic gross and microscopic lesions
PCR assay for detection of the fowlpox virus-specific genes
Cutaneous fowlpox infections usually produce characteristic gross and microscopic lesions. When only small cutaneous lesions are present, it is often difficult to distinguish them from abrasions due to fighting.
Microscopic examination of affected tissues stained with H&E reveals eosinophilic cytoplasmic inclusion bodies. This is the most commonly used method in diagnostic laboratories.
The cytoplasmic inclusions are also detected by fluorescent antibody and immunohistochemical methods (using antibodies against fowlpox virus antigens). The elementary bodies (Borrel bodies) in the inclusion bodies (Bollinger bodies) can be detected by light microscopy in smears from lesions stained by the Gimenez method. Viral particles with typical poxvirus morphology can be demonstrated by negative-staining electron microscopy as well as in ultrathin sections of the lesions.
The virus can be isolated by inoculating chorioallantoic membrane of developing chicken embryos, susceptible birds, or cell cultures of avian origin. Chicken embryos (9–12 days old) from an SPF flock are the preferred and convenient host for virus isolation.
The genomic profiles of field isolates and vaccine strains of fowlpox virus can be compared by restriction fragment length polymorphism (RFLP). Detailed genetic analysis reveals differences between vaccine strains and field strains responsible for outbreaks of fowlpox in previously vaccinated chicken flocks. Whereas vaccine strains of fowlpox virus contain remnants of long terminal repeats of reticuloendotheliosis virus (REV), most field strains contain full-length REV in their genome.
Although nucleic acid probes derived from cloned genomic fragments of fowlpox virus have been used for differentiation of the diphtheritic form of fowlpox (involving the trachea) from infectious laryngotracheitis, PCR amplification of virus-specific genomic fragments is becoming more convenient where facilities are available.
PCR assay has been used effectively to differentiate field and vaccine strains of the virus, whether or not full-length REV is present in those strains that are associated with outbreaks in vaccinated birds. In this regard, DNA isolated from the formalin-fixed tissue sections of birds with histopathologic findings consistent with fowlpox can be used for PCR amplification of genomic fragments using specific primers.
Because most outbreaks of fowlpox in previously vaccinated chickens are due to strains with a genome that contains full-length REV, use of REV envelope-specific primers to determine the presence of full-length REV is helpful in such cases.
Two monoclonal antibodies that recognized different fowlpox virus antigens were developed. These monoclonal antibodies were useful for strain differentiation by immunoblotting.
The complete nucleotide sequences of the genomes of fowlpox virus, canarypox virus, and some other avian poxviruses have been determined. This information is useful for comparing the sequences of selected genes of other avian poxviruses as well as in their phylogenetic analysis.
Naturally infected and vaccinated birds develop both humoral and cell-mediated immune responses. Humoral immune response can be measured by ELISA, agar gel precipitation (AGP), or virus neutralization tests. AGP is a very simple and convenient test; however, its sensitivity is low compared with ELISA.
Treatment and Prevention of Fowlpox
Vaccination
There is no specific effective treatment for birds infected with fowlpox virus; therefore, prevention is key. Disease control is best accomplished by vaccination.
Where fowlpox is prevalent, chickens and turkeys should be vaccinated with a live-embryo- or cell-culture-propagated virus vaccine. The most widely used vaccines are live, attenuated fowlpox virus and pigeonpox virus isolates of high immunogenicity and low pathogenicity.
In high-risk areas, vaccination with a live, attenuated virus vaccine of cell-culture origin in the first few weeks after hatching and revaccination at 12–16 weeks old is often sufficient.
Health of birds, extent of exposure, and type of operation determine the timing of vaccinations. Because the infection spreads slowly, vaccination is often useful to limit spread in affected flocks if administered when < 20% of the birds have lesions.
Passive immunity may interfere with multiplication of vaccine virus; progeny from recently vaccinated or recently infected flocks should be vaccinated only after passive immunity has declined.
Vaccinated birds should be examined 1 week later for swelling and scab formation (“take”) at the site of vaccination. Absence of vaccine take indicates lack of potency of vaccine, passive or acquired immunity, or improper vaccination. Revaccination (with another vaccine lot number) may be indicated.
Zoonotic Risk of Fowlpox
There is no zoonotic risk associated with fowlpox virus. Avian poxviruses cause a productive infection in avian species but a nonproductive infection in mammalian hosts. Consequently, avian poxviruses have been used as vectors for expression of genes from mammalian pathogens in the development of safe recombinant vaccines.
Key Points
Fowlpox is a disease of economic importance in chickens and turkeys.
Diagnosis is commonly made on the basis of histopathologic findings in infected tissue.
Live vaccines are available for prevention.
For More Information
Tripathy DN, Reed WM. Pox. In: Swayne DE, Boulianne M, Logue CM, et al, eds. Diseases of Poultry. 14th ed. Wiley; 2019: 364-381. doi:10.1002/9781119371199.ch10
World Organisation for Animal Health. 2023. https://www.woah.org/en/disease/fowl-pox/