With few exceptions, mastitis occurs when microbes enter the teat via the teat canal. Almost any microbe can opportunistically invade the teat canal and cause mastitis. However, most infections are caused by various species of streptococci (or similar gram-positive cocci), staphylococci, and gram-negative rods, especially lactose-fermenting organisms of enteric origin, commonly termed coliforms. From an epidemiologic standpoint, the primary reservoirs of infection for most pathogens may be regarded as contagious or environmental, although this separation can be ambiguous for some pathogens.
Except for Mycoplasma spp, which may spread from cow to cow through aerosol transmission and invade the udder subsequent to bacteremia, contagious spread of pathogens occurs during milking, through such pathways as milkers’ hands or the liners of the milking unit. Species that primarily use this mode of transmission include Staphylococcus aureus, Streptococcus agalactiae, and Corynebacterium bovis. Most other species are opportunistic invaders from the cow’s environment, although other streptococci and staphylococci may also have a contagious component.
Additionally, contagious transmission infrequently occurs for pathogens typically associated with environmental reservoirs, eg, through the development of host-adapted virulence factors (Escherichia coli) or by shedding of overwhelming numbers of bacteria from infected udders (Trueperella [formerly Arcanobacterium] pyogenes, and Lactococcus spp). Contagious transmission has also been identified as a possible means of infection for the algae Prototheca zopfii.
The bedding used to house cattle is the primary source of environmental pathogens, but contaminated teat dips, intramammary infusions, water used for udder preparation before milking, water ponds or mud holes, skin lesions, teat trauma, and flies have all been incriminated as sources of infection.
Intramammary infections (IMIs) are often described as subclinical or clinical mastitis. Subclinical mastitis is the presence of an infection without apparent signs of local inflammation or systemic involvement. Although transient episodes of abnormal milk may appear, subclinical mastitis is, for the most part, asymptomatic. If the infection persists for at least two months, the infection is termed chronic. Once established, many of these infections persist for entire lactations or the life of the cow, although this varies with the causative pathogen.
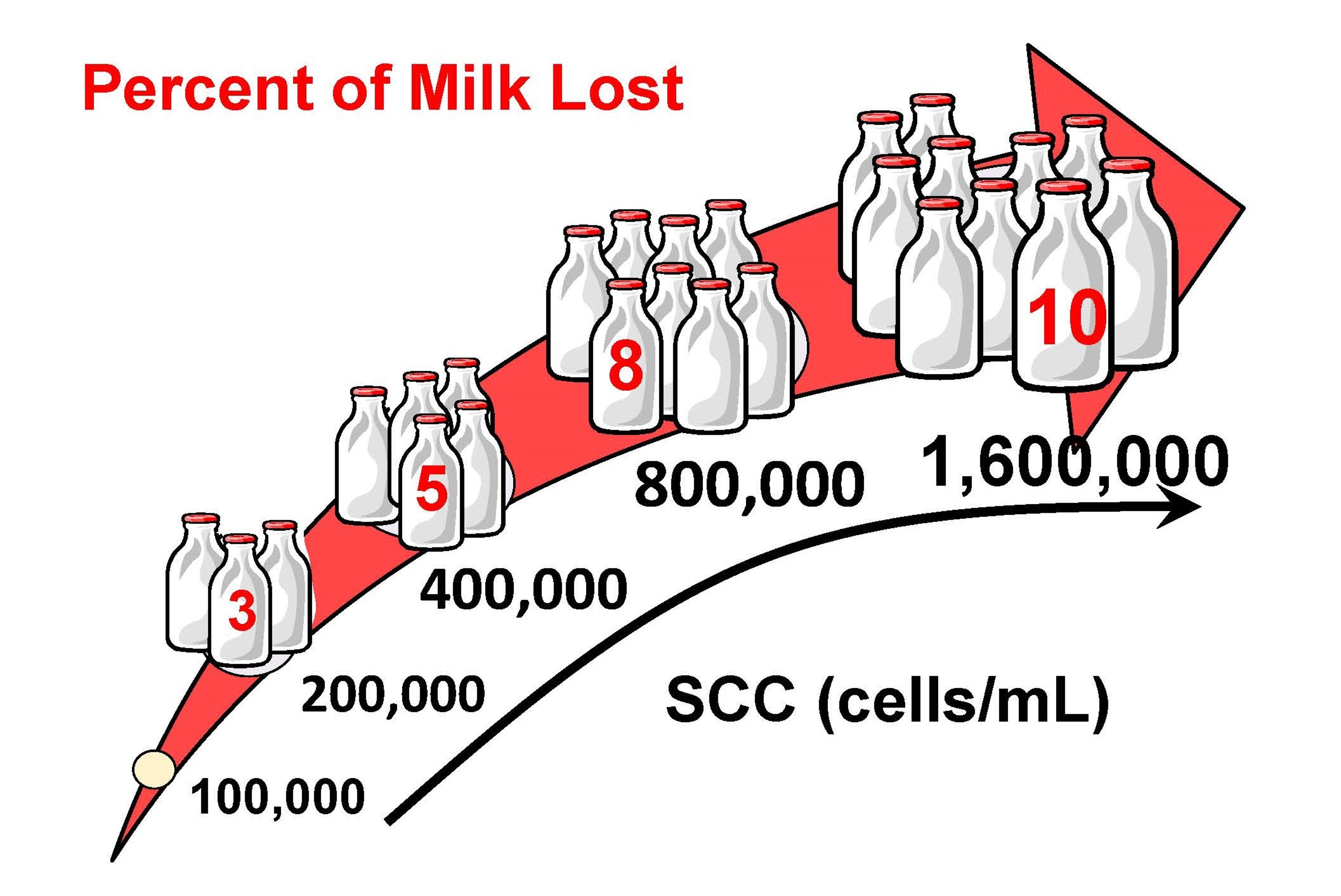
Detection of subclinical mastitis is best done by testing milk for somatic cell counts (SCCs) (predominantly leukocytes) using either the California Mastitis Test or automated methods provided by dairy herd improvement organizations. SCCs are positively correlated with the presence of infection. Inflammatory changes and decreases in milk quality may start with SCCs as low as 100,000 cells/mL. Although variable (especially if determined on a single analysis), an SCC of ≥200,000 cells/mL in a cow indicates a high likelihood of infection. Likewise, the higher the SCC in a herd bulk tank, the higher the prevalence of infection in the herd. Herd SCCs < 200,000 cells/mL are considered desirable, and lower counts can be attained.
Milk yield decreases in cows with subclinical mastitis. The loss of milk from inflammation is directly proportional to the individual cow SCC; as SCC rises, milk production decreases. These losses can be especially significant if an IMI occurs in early lactation and persists as a chronic infection throughout lactation.

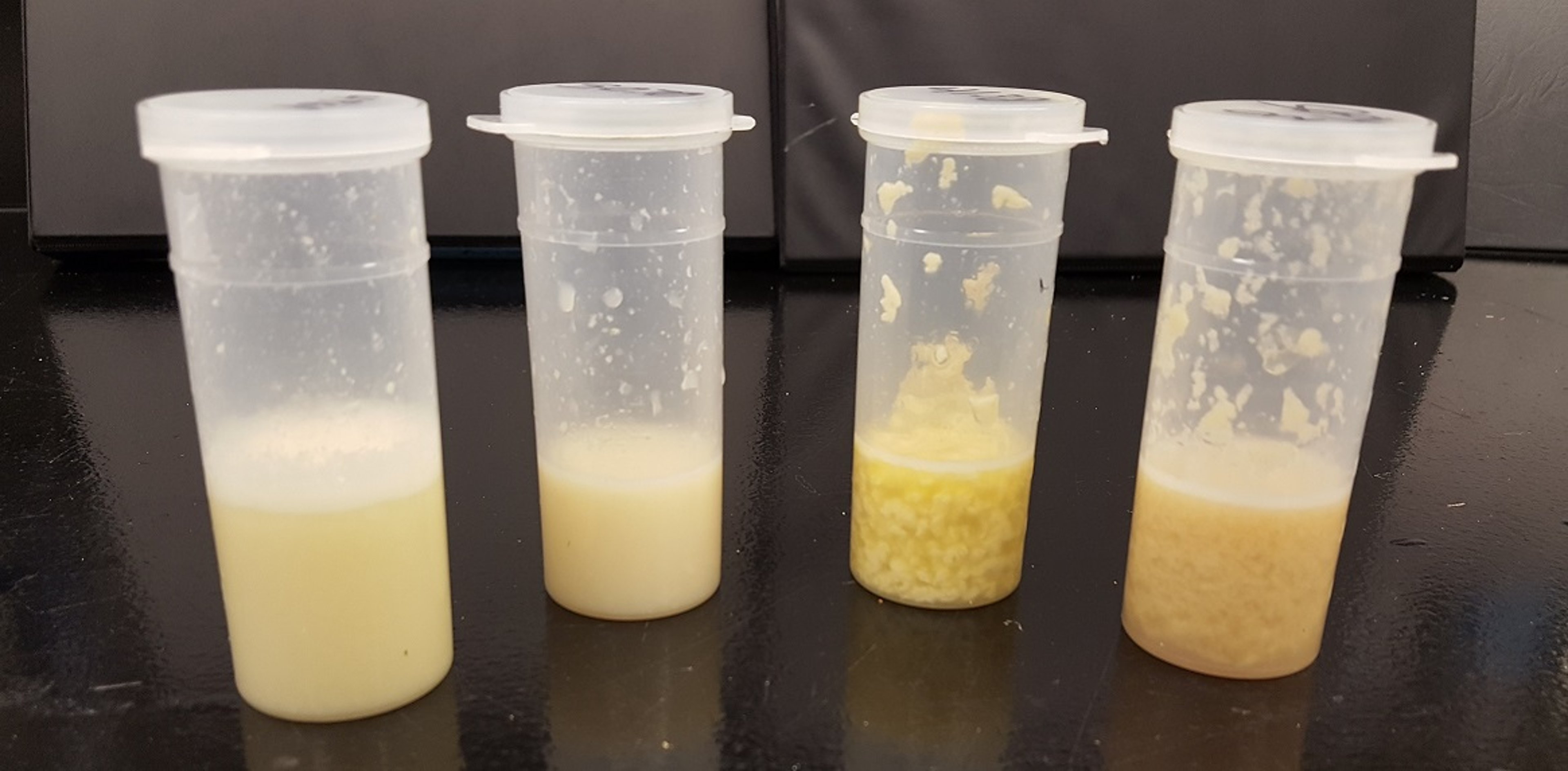
Courtesy of Dr. Ronald Erskine.
Clinical mastitis is an inflammatory response to infection causing visibly abnormal milk (eg, color, fibrin clots). As the extent of the inflammation increases, changes in the udder (swelling, heat, pain, redness) may also be apparent. Clinical cases that include only local signs are referred to as mild or moderate. If the inflammatory response includes systemic involvement (fever, anorexia, shock), the case is termed severe. If the onset is very rapid, as often occurs with severe clinical cases, it is termed acute or severe mastitis. More severely affected cows tend to have serous secretions in the affected quarter.
Although any number of quarters can be infected simultaneously in subclinical mastitis, typically only one quarter will display clinical mastitis. However, it is not uncommon for clinical episodes caused by Mycoplasma to affect multiple quarters. Gangrenous mastitis can also occur, particularly when subclinical, chronic infections of S aureus become severe at times of immune dysfunction (eg, at parturition). As with subclinical mastitis, culture of milk samples collected from affected quarters is the only reliable method to determine the etiology of clinical cases.
Herd size, and the proportion of milk that is produced by large herds, is increasing in the US and global dairy industry. Thus, the reliance on hired employees, as well as immigrant labor, to perform critical tasks such as milking cows, is also increasing. Additionally, many dairy managers are likely to have limited human resource knowledge and management experience. Thus, they tend not to perceive themselves as employee trainers; this often leads to frustration with protocol drift—and a sense that employees are not motivated to engage in the success of the farm beyond prescribed instructions. Taken together, this has resulted in a gap between the human resource needs arising within the industry and the capacity of producers and managers to address them.
Although extensive research and clinical trials have determined the foundations for mastitis control, employee knowledge of these concepts is often lacking compared with herd managers. The best milk quality protocols will fail if the compliance with the protocols is inconsistent. Contrary to popular belief, the majority of employees have stated in surveys that they are willing to learn more about not just how protocols should be performed, but why they are important. Thus, veterinarians have an opportunity to help with employee training and education and serve as "on-farm science teachers."
Subclinical Mastitis
Epidemiology of Subclinical Mastitis in Cattle
All dairy herds have cows with subclinical mastitis; however, prevalence of infected cows varies from 5%–75%, and quarters from 2%–40%. Many different pathogens can establish a chronic infection in which clinical signs of mastitis will manifest only occasionally. Historically, subclinical mastitis control focused on the contagious pathogens S agalactiae and S aureus, as well as other gram-positive cocci, most notably Streptococcus dysgalactiae (which may also be contagious or an environmental pathogen), Streptococcus uberis, enterococci, and numerous other nonaureus staphylococci (previously termed coagulase-negative staphylococci), including Staphylococcus hyicus, S epidermidis, S xylosus, and S intermedius. Herds have been identified that have considerable subclinical mastitis caused by gram-negative rods such as Klebsiella sp, Serratia marcescens, Pseudomonas aeruginosa, and other atypical pathogens such as Candida spp. and Prototheca zopfii. Because of increasing herd size throughout the dairy industry, and more fluid movement of cattle between herds and geographic locations, Mycoplasma spp, especially M bovis, has been recognized as a frequent pathogen in some herds, with cows exhibiting both subclinical and clinical signs.
For contagious pathogens, adult lactating cattle are most at risk of infection. The primary reservoir of infection is the mammary gland; transmission occurs at milking with either milkers’ hands or milking equipment acting as fomites. Primiparous heifers have been reported to be infected with staphylococci and streptococci before calving, although the prevalence varies greatly among herds and geographic regions. Teat-end dermatitis caused by the horn fly, Haematobia irritans, which can harbor S aureus, has been associated with increased risk of infection in heifers, especially in warmer climates.
For S agalactiae, S aureus, and nonaureus staphylococci, there is little or no seasonal variation in incidence of infection.
Treatment of Subclinical Mastitis in Cattle
Therapy for subclinical mastitis is given on the premise that treatment costs will be outweighed by production gains after elimination of infection and that prevention is always preferred. Also, immune function of leukocytes in a lactating gland is impaired compared with other tissues, such as the lung. For these reasons, expectations and the need to treat IMI should be carefully considered, and in lactating cows, generally avoided. This is especially the case if treatment does not consider the causative agent or duration of infection.
In the case of contagious pathogens, elimination may result in a decrease of the reservoir of infection for previously noninfected cows. No significant economic losses will occur as a result of delaying therapy until bacterial culture can be completed. However, many subclinical IMI are chronic, and, particularly in the case of S aureus, prediction of therapeutic outcome by in vitro testing is unreliable. Drug distribution after intramammary administration may not be adequate because of extensive fibrosis and microabscess formation in the gland. Cows with a long duration of infection (>3 months), more than one quarter infected, or infected with pathogens resistant to antimicrobials typically used in intramammary infusions are likely to be refractive to therapy.
An unusual opportunity for successful therapy of subclinical IMI is possible with S agalactiae. Prevalence of IMI caused by this pathogen can be rapidly reduced by treating all the infected cows in a herd with antimicrobials. All four quarters of infected cows should be treated to ensure elimination of the pathogen and to prevent possible cross-infection of a noninfected quarter. Cure rates often range from 75% to 90%. Labeled use of commercial intramammary products that contain amoxicillin, penicillin, or cephalosporins is preferred. Use of drugs originating from multiple-dose vials (labeled for systemic therapy) should not be used for intramammary therapy, because commercial intramammary preparations have superior quality control standards for sterility and better reliability to predict withholding periods for milk and meat after treatment. It is critical to apply strict aseptic techniques (eg, use of alcohol-soaked pads for teat-end preparation) whenever any intramammary infusion product is administered.
Herds undergoing extensive therapy for S agalactiae must be monitored by SCCs and subsequent milk culture to further identify cows not treated or cured during the initial therapy. Usually, 30-day monitoring intervals are successful. A small percentage of cows will not respond to therapy and are best segregated or culled. In addition, failure to use postmilking teat dipping and blanket dry cow treatment to prevent new infections will ultimately result in reinfection of the herd.
Most other streptococci also display in vitro susceptibility to numerous antimicrobials, especially beta-lactam drugs. Despite this apparent susceptibility, many streptococcal infections are not as easily cured as those caused by S agalactiae. Generally, subclinical infections caused by S uberis and S dysgalactiae should be preferentially treated at the end of lactation with intramammary infusions of commercial dry cow products. Cure rates at this time may exceed 75%. Other streptococcal-like organisms such as Lactococci and Enterococci are often refractory to therapy.
S aureus intramammary infections result in deep-seated abscesses. Therapy is difficult, because resistance to antimicrobials (particularly beta-lactams) is more common than with streptococcal infections, and S aureus may survive intracellularly after phagocytosis. Intramammary infusions may cure only 20%–40% of infections, and less for chronic infections.
The success rate of therapy for chronic subclinical IMI caused by S aureus may be increased by using both parenteral and intramammary therapy. However, systemic therapy involves extralabel drug use, and milk and meat withholding periods must be determined. Additionally, therapy should be administered for periods long enough (7–10 days) to allow effective clearance of the pathogen. Dry cow therapy is more economical and least likely to result in residues in milk compared with lactating cow therapy. Depending on susceptibility testing, lipophilic antimicrobial drugs that distribute well into mammary tissue, such as oxytetracycline (11 mg/kg/day), are the best candidates for systemic administration, although several studies have found oxytetracycline (administered for 4 days or less) to be ineffective. Cure rates may not be much better than those attained from spontaneous cure, and cure must be defined critically (ie, longterm impact on SCC and milk production).
Occasionally, premature agalactia will occur in chronically infected quarters. Culling may be a practical option for these cows. Alternatively, it is common to dry off the infected quarter and continue to milk the cow. This may have some benefit for genetically superior animals within a herd or for cows that are to be maintained until calving. The goal is to eliminate the infection by causing fibrosis of the affected quarter, thus reducing the risk of infection for other cows. Additionally, such cows will no longer be contributing high-SCC milk (from the infected quarter), thus helping to maintain quality of the marketed milk. Drying off quarters, culling, or therapy as a means to reduce SCC contributions from infected cows is a palliative approach to mastitis control, which would be better addressed by prevention of infections.
Dry Cows
The dry period of the lactation cycle is a critical time for the udder health of dairy cows. The mammary gland undergoes marked biochemical, cellular, and immunologic changes. Involution of the mammary parenchyma begins 1–2 days after the end of lactation and continues for 10–14 days. During this time, the gland is particularly vulnerable to new IMI. However, the involuted mammary gland offers the most hostile immune environment for bacterial pathogens. Consequently, the dry period is an ideal time to attain synergy between antimicrobial therapy and immune function, without incurring the extensive costs typical of lactating cow therapy.
Numerous commercial products are available for dry cow treatment and include penicillin, cloxacillin, cephapirin, ceftiofur, or novobiocin. One tube per quarter is sufficient and should be administered immediately after the last milking of lactation. Therapy should not be repeated by intramammary infusion; if there is a perceived need to extend therapy, systemic administration should be used as an adjunct to the intramammary infusion. In addition to eliminating existing subclinical infections, one of the most critical roles of dry cow therapy is to prevent new infections.
Internal teat sealants, as a supplemental infusion after antimicrobial infusions at dry off, serve as a physical barrier to help reduce new infections. In some cases, new IMI during the dry period have been further reduced by 50% compared with antimicrobial therapy alone. This positive effect may be due in part to the level of milk production at dry off in dairy cows, which has increased considerably over time. Increased milk production at dry off delays involution and results in a greater proportion of teat canals that are patent during the entire dry period. As with lactating cow infusions, it is important to follow strict aseptic technique for any infusion at dry off.
Blanket dry cow therapy (BDCT; treating all quarters of all cows at dry off) has been a foundation of mastitis control for more than 50 years. However, despite the high degree of success of BDCT in preventing and curing IMI over the dry period, the landscape of mastitis has changed, including a lower prevalence of S agalactiae and S aureus in many herds and higher prevalence of environmental pathogens. Also, most of the dry cow products target gram-positive cocci, which may not be the predominant pathogens in a particular herd. Finally, advances in housing and bedding, nutritional management, and internal teat sealants have all helped reduce the rate of IMI during the dry period. Thus, selective dry cow therapy (SDCT; treating only cows that are identified as infected at dry off) could be considered as an alternative to BDCT. The biggest caveat in choosing BDCT versus SDCT is that each herd has unique challenges and management approaches to their operation, so a dry cow therapy program must be tailored to fit their needs.
Herds that struggle with basic mastitis control (bulk tank SCC > 200,000 cells/mL) are not the best candidates for SDCT. Additionally, both metrics for outcomes and protocols to select cows for dry cow therapy should be rigorously followed. Herd-specific algorithms should include, at the very least, both clinical mastitis history and individual cow SCC during the lactation before dry off and after calving. In the USA, fewer herds are using dairy herd improvement SCC testing and thus have difficulty monitoring subclinical mastitis. Also, because of greater emphasis on so-called parlor efficiency, ie, the rate of cow throughput in many larger dairies, the ability of milking operators to correctly identify clinical mastitis, let alone strip milk from teats, is suspect.
Thus, the ability to determine the efficacy of a dry cow therapy program, such as new and cured IMI over the dry cow period, and clinical mastitis in the first 30 to 60 days in milk, will be tenuous in some herds. Although culture of milk samples, either before drying off or from clinical cases, is a useful part of any herd mastitis control program, especially for those choosing SDCT, there is reluctance on the part of most dairy producers to use milk cultures. The bottom line for the decision to use SDCT is to ensure that the tools and the willingness are in place to properly select cows and monitor changes in milk quality.
Recombinant bovine granulocyte colony-stimulating factor (rbG-CSF) covalently bound to polyethylene glycol administered twice subcutaneously, to cows before and within 24 hours after calving, increases circulating numbers of polymorphonuclear leukocytes. This induced neutrophilia is hypothesized to permit a more robust and timely response for cows that may be prone to postpartum infectious diseases, including mastitis. However, the results from subsequent field trials in dairies found inconsistent impacts on the rate of clinical mastitis during the first 30 days after calving. Also, rbG-CSF did not impact subclinical mastitis (SCC) in treated vs nontreated cows. This technology may help transition cows overcome polymorphonuclear leukocyte-related immune dysfunction, although there are other pathways of postpartum immune dysfunction (eg, metabolic stress) that may not be impacted by this approach. Clinical benefits may be limited in herds that already have a low incidence of postpartum clinical mastitis. Finally, rbG-CSF should not be used as a substitute for other sound transition cow management practices, including housing hygiene and control of metabolic and heat stress.
Heifers
Most IMI in calving heifers are caused by staphylococcal species other than S aureus, which have a high rate of spontaneous cure. However, under some herd conditions, a substantial portion of heifers have more intractable infections, including those caused by S aureus. Potential sources include milk (fed to calves) and body sites such as tonsils and skin. There is also a geographic risk factor: fly bite dermatitis of the teat end, which compromises this important physical barrier to infection, may play a role in the pathogenesis.
Intramammary infusions of beta-lactam antibacterial drugs 7–14 days before expected calving dates have been reported to reduce the prevalence of IMI at calving. However, longterm benefits on SCCs, milk production, and incidence of clinical mastitis during lactation were found to be highly variable by herd and not consistent. Strict teat-end antisepsis should be followed before infusion to prevent contamination; thus, labor to handle animals for treatment can be extensive. This is not a recommended management program for many dairies. However, if herd records indicate that the prevalence of IMI in first-lactation animals at calving is high (>20%), particularly with staphylococci, this regimen may be considered.
Prevention of Subclinical Mastitis in Cattle
New infections are prevented by focusing management efforts on reducing the presence of pathogens on the teat end. Thus, clean and dry bedding, clean and dry udders at the time of milking, not using water during the milking protocols (except to maintain hygiene of milking units), as well as maintaining teat-end health all have a positive effect on control.
For contagious pathogens, the single most important management practice to prevent transmission of new infections is the use of an effective germicide as a postmilking teat dip. These products should be applied as a dip (rather than a spray) immediately after milking. Other practices that augment teat hygiene include use of individual towels to dry teats, gloves for milkers’ hands, use of a premilking germicide (spray or dip), attachment of units at the proper time after teat stimulation (60–120 seconds), not overmilking, cleaning milking units after an infected cow has been milked, or segregation of infected cows. This last option may be unrealistic for cattle in free housing that are normally segregated for nutritional or reproductive reasons. Routine milking equipment evaluations should be conducted to ensure teat-end vacuum is operating at a proper level and remains stable during milking. Proper pulsator function is critical, and liners and rubber air hoses should be replaced as needed.
Milking hygiene also reduces the new infection rate of environmental pathogens. However, more importantly, cows should be provided dry, clean housing. Inorganic bedding supports less bacterial growth than cellulose-based material; thus, sand is preferred over sawdust, straw, recycled paper, or manure. In particular, a higher incidence of infections caused by Klebsiella has been associated with sawdust bedding. However, bacterial numbers can vary greatly depending on moisture and presence of organic matter (such as in sand after recycling). Thus, control of environmental mastitis should not be based solely on the choice of bedding material. Practices that have a positive impact on environmental mastitis control include:
regular cleaning or changing of bedding
reducing heat stress
removing udder hair
preventing teat trauma
reducing udder edema in periparturient cows by nutritional management of potassium and sodium intake
avoidance of areas that accumulate water
maintenance of stalls for proper lying behavior
preventing frostbite and fly exposure
Clinical Mastitis
When the balance between host defenses and invading pathogens causes a marked inflammatory response, clinical signs become apparent. Infections from any pathogen can be clinical or subclinical, depending on the duration of infection, host immune status, and pathogen virulence. Control of clinical mastitis usually focuses on prevention and elimination of pathogens that arise from an environmental reservoir. Thus, the epidemiology and prevention of clinical mastitis is similar to control of subclinical mastitis.


Courtesy of Dr. Ronald Erskine.
Epidemiology of Clinical Mastitis in Cattle
Except for outbreaks of Mycoplasma, clinical mastitis in most dairy herds is caused by environmental pathogens. In addition, many clinical mastitis cases are transient, especially those that are initial episodes for a cow and quarter. Thus, assessment of clinical mastitis is based on incidence and not prevalence.
Methods to monitor subclinical mastitis, ie, routine SCCs and culture of cows with increased SCCs, are inconsistent predictors of clinical mastitis cases. Cows with high SCCs caused by chronic infections may occasionally display clinical mastitis, although it is usually mild. However, cows with low SCCs are also prone to develop clinical mastitis.
Cow history from each case (eg, season, age, stage of lactation, and previous episodes) should be recorded to help determine risk factors. Milk samples should be collected from affected quarters and, when feasible, antimicrobial susceptibility testing performed. For well-managed herds in which mastitis caused by contagious pathogens has been controlled, a goal for the incidence of clinical mastitis should be 1–2 cases/100 cows milking/month. Severe mastitis cases should be in the range of 1–2 cases/100 cows milking/year.
Typically, 30%–40% of milk samples collected from clinical mastitis cases yield no organisms on culture. However, of the samples that do yield organisms, 90%–95% of the isolated bacteria include a wide variety of streptococci, staphylococci, or coliforms. If this is not the case, especially if noncoliform, gram-negative rods, mycotic, or algal (Prototheca sp) pathogens predominate, a point source of infection should be considered.
Severe Clinical Mastitis in Cattle
Coliforms (lactose-fermenting gram-negative rods of the family Enterobacteriaceae) are the most common cause of this form of mastitis. Most coliform infections are cleared from the gland with few or mild clinical signs. However, severe mastitis (systemic signs) occurs when bacterial concentrations in milk increase enough to stimulate a marked immune response.


Courtesy of Dr. Ronald Erskine.
Severe mastitis caused by coliforms results in a higher incidence of cow death or agalactia-related culling (30%–50% of cases) than mastitis caused by other pathogens (5%–10% of cases). Prognosis for cases of Klebsiella infection should be particularly guarded, because affected cows are twice as likely to be culled or die than those infected by other coliforms. Thus, primary therapy for severe clinical mastitis should be directed against coliform organisms, although secondary consideration must be given for other causative agents. Supportive care, including fluids, is likely the most beneficial component of the therapeutic regimen. Antimicrobial therapy is ideally based on identification of the causative pathogen; however, this is not attainable for some hours after initial case recognition. In addition, systemically administered antimicrobial regimens administered for severe clinical mastitis are not labeled in the USA by the FDA.
After infection, coliform numbers in milk increase rapidly, often attaining peak concentrations within a few hours. A rapid decline in bacteria follows neutrophil migration into the gland.
Inflammatory and systemic changes that result during severe coliform mastitis are caused by release of lipopolysaccharide (LPS) endotoxin from the bacteria and subsequent activation of cytokine and arachidonic acid-derived mediators of inflammation; this causes the acute phase response (sepsis). By the time therapy is initiated, much of the LPS exposure has occurred. Thus, the primary therapeutic concern is the treatment of LPS-induced shock with fluids, electrolytes, and anti-inflammatory drugs. The IV route is preferred as the initial method of fluid administration.
If isotonic saline is administered, 30–40 L are necessary throughout a 4-hour period, which can be difficult under farm conditions. A practical alternative is 2 L of 7% NaCl (hypersaline) administered IV. This induces rapid fluid uptake from the body compartment into the circulation. Cows should then be offered free-choice water to drink, and if at least 8 to 10 gallons is not consumed, 5–7 gallons should be pumped into the rumen. Many cows with endotoxic shock are marginally hypocalcemic; thus, 500 mL of calcium borogluconate should be administered SC (to avoid potential complications of IV administration). Alternatively, rapid absorption calcium gels, designed for periparturient hypocalcemia, can be given. If the cow remains in shock, continued fluid therapy should be administered PO or IV as isotonic, not hypertonic, fluids.
If administered early in the course of disease, glucocorticoids may be helpful in cases of mastitis caused by endotoxin-producing coliforms. These compounds inhibit many proinflammatory pathways related to the acute-phase response. Administration of dexamethasone (30 mg, IM) to dairy cows immediately after introduction of E coli into the mammary gland has been reported to reduce mammary gland swelling and improve rumen motility. Care should be exercised in administering these drugs to pregnant animals; however, severe clinical mastitis in and of itself may cause pregnancy loss in cattle.
There is little published research on the use of glucocorticoids for mastitis caused by gram-positive bacteria. It is reasonable to expect that gram-positive infections would be less likely to benefit from the anti-inflammatory activities of glucocorticoids and may even be adversely affected. Intramammary glucocorticoid administration to reduce local inflammation has been considered as a therapeutic option. Although products that combine antimicrobial and glucocorticoid drugs for intramammary administration exist in Europe, it is not clear whether clinical benefit is gained when compared with antimicrobial therapy alone. As a general guideline, glucocorticoid treatment should be reserved for severe cases of gram-negative mastitis, with a single dose administered early in the disease course.
NSAIDs are widely used in treatment of acute mastitis. Flunixin meglumine, flurbiprofen, carprofen, meloxicam, and ketoprofen have been used as treatments for experimental coliform mastitis or endotoxin-induced mastitis. Systemic use of these drugs is preferred over orally administered aspirin, which is not likely to attain effective concentrations in tissue or lead to beneficial results. Dipyrone use in food animals is specifically prohibited by the FDA. Phenylbutazone is prohibited in dairy cattle >20 months old; the tolerance level for phenylbutazone is zero, and detection of any concentration is an illegal residue. Thus, these two drugs should not be used for anti-inflammatory therapy for mastitis in cattle.
Ketoprofen is available as a veterinary product for use in horses, has a high therapeutic index, has favorable pharmacokinetics for use in lactating dairy cattle, and is approved for use in cattle in some countries; however, it is not labeled for food animal use in the USA. The Food Animal Residue Avoidance Databank (FARAD) recommends withdrawal intervals of 7 days for slaughter and 24 hours for milk, with IV or IM administration, for dosages up to 3.3 mg/kg/day, for up to 3 days.
Flunixin meglumine is labeled for beef and dairy cattle. It is the only NSAID labeled for use in cattle in the USA and is therefore the most logical choice to treat severe clinical mastitis. In field studies, increased survival and improved milk production have not been demonstrated after treatment of clinical acute mastitis with flunixin meglumine at a dosage of 1.1 mg/kg. However, in studies of experimental mastitis, flunixin meglumine reduced the severity of clinical signs such as fever, depression, heart and respiratory rates, and udder pain. The FDA-approved withdrawal intervals are 4 days for slaughter and 36 hours for milk when used as labeled by IV administration. Because of extensive and unpredictable withdrawal periods, this drug should not be administered by IM injection. As with the glucocorticoids, NSAIDs may provide symptomatic relief and promote well-being. Administration early in the course of infection is likely to increase clinical benefit.
Antimicrobial therapy may be of secondary importance relative to immediate supportive treatment of endotoxic shock, but it remains an integral part of a therapeutic regimen. Occasionally, coliform infections do result in chronic mastitis. Bacteremia occurs in >50% of severe coliform cases. In addition, numerous other pathogens, including gram-positive cocci, cause severe clinical mastitis, which can be difficult to distinguish from cases caused by coliforms at initial presentation.
Selection of an appropriate antimicrobial for the treatment of severe coliform mastitis depends primarily on the susceptibility of the organism to the selected drug and the ability to maintain effective concentrations at the primary pharmacologic target (which, in the case of coliform mastitis, is the plasma compartment of the cow).
Cows experimentally challenged with E coli and treated with 500 mg of intramammary gentamicin bid did not have lower peak bacterial concentrations in milk, duration of infection, convalescent SCCs or serum albumin concentrations in milk, or rectal temperatures than untreated challenged cows. In addition, gentamicin readily diffused through the milk-blood barrier, resulting in drug residues in the kidney that could extend beyond 18 months. Because of zero tolerance for aminoglycoside residues at slaughter, the use of this class of drugs in dairy cattle is not recommended.
Oxytetracycline (11 mg/kg/day, IV) improved outcome of cows with clinical coliform mastitis (not necessarily severe) as compared with cows that did not receive systemic antibacterials. Ceftiofur sodium (2.2 mg/kg/day, IM ) decreased mortality and cull rates of cows with severe coliform mastitis, as well as enhanced recovery of milk production. This drug distributes poorly to the mammary gland, supporting the importance of targeting therapy for bacteremia in addition to the mammary gland.
Intramammary infusion of antimicrobials should be administered to cows with severe clinical mastitis. This treatment may not affect the outcome of coliform cases but will likely improve outcomes for cases caused by gram-positive cocci. The need for continued antimicrobial therapy in cows with grossly abnormal milk, but with improved appetite, attitude, and milk production, should be evaluated critically. Unnecessary extension of therapy in these instances results in increased discarded milk expenses and risk of antimicrobial residues in marketed milk.
Mild Clinical Mastitis in Cattle

Courtesy of Dr. Ronald Erskine.
As previously stated, microorganisms are not isolated from 30%–40% of bacteriologic cultures of milk samples collected from cows with clinical mastitis. Many mild mastitis cases that fail to yield bacteria on culture are coliform intramammary infections that resolve before treatment is necessary. In addition, numerous mild clinical mastitis cases are temporary setbacks in the balance between pathogen and host defenses that occurs in chronic IMI.
Common sense and individual herd history should determine the course of therapy for mild clinical mastitis cases in dairy herds. Use of approved commercial intramammary infusions is the best option. The foundation of success is bacteriologic cure but will be more practically based on return to normal milk. The frequency of relapsed cases should be monitored as the best measure of therapeutic efficacy, because many cases will be deemed to have been successfully treated in the short term but relapse later in lactation. If mastitis recurs regularly in affected quarters in the absence of systemic signs, repeated treatment of what now has become a chronic IMI is not warranted.
Additionally, augmentation with parenteral therapy for these cases has not been demonstrated to be effective and will not likely overcome the expense of discarded milk, other related treatment costs, and the increased risk of residues in milk and meat. Previous history of clinical cases ("repeat offenders"), long duration of infection (as exhibited by high individual SCCs or extended periods of increased SCCs), and infections caused by nonresponsive pathogens are the greatest risk factors for poor therapeutic outcome. Practitioners should develop a protocol with dairy clients to reduce unnecessary treatment of poor-risk cases as listed above and not rely on continued unsuccessful therapy or seeking a "better drug."
If standard regimens achieve less than desired results, it would be better to extend initial therapy for a prolonged period rather than to change to other antimicrobial drugs or increase the amount of each dose. Studies have demonstrated improved cure rates for gram-positive cocci, especially coagulase-negative staphylococci and streptococci, when infected quarters were treated with intramammary infusions for up to 8 days as compared with 2 days. However, results will vary with the bacteriology of the herd. Care should be especially exercised in aseptic preparation of the teat for extended therapy because of the increased risk of nosocomial infections.
The most efficient use of antimicrobial therapy, and the best option to reduce unnecessary use, is to apply "culture-based therapy" decision-making as part of the therapeutic protocol on a farm. Therapy is withheld from an affected quarter (mild clinical mastitis) until results from a bacteriologic culture of a milk sample are obtained, usually within 24–48 hours. Culture-dependent treatment decisions may vary from farm to farm, but in general, antimicrobial therapy does not improve the outcome of cases that yield no organism, Gram-negative organisms, and unusual pathogens (eg, Pseudomonas spp). Thus, by excluding cases that yield these culture results, dairy herds can reduce antimicrobial use for mild clinical therapy by 50%–75%.
Additionally, the "waiting period" between clinical onset and treatment decisions (after culture results) does not adversely impact bacterial cures, relapses, milk production, or SCCs for cows selected for therapy. Simple milk bacteriology that identifies gram-positive from gram-negative pathogens, as well as no isolation, can be performed in veterinary clinics, or with proper training, on the farm.
Unusual Pathogens in Clinical Mastitis in Cattle
Pseudomonas aeruginosa may cause outbreaks of clinical mastitis. Generally, a persistent infection occurs, which may be characterized by intermittent acute or subacute exacerbations. The organism is found in soil-water environments common to dairy farms. Herd infections have been reported after extensive exposure to contaminated wash water in the milking parlor, teat cup liners, or intramammary treatments administered by milkers. Failure to use aseptic techniques for udder therapy or use of contaminated milking equipment may lead to P aeruginosa IMI. Severe peracute mastitis with toxemia and high mortality may occur in some cows, whereas subclinical infections may occur in others. The organism has persisted in a gland for as long as five lactations, but spontaneous recovery may occur. Other than supportive care for severe episodes, therapy is of little value. Culling is recommended for persistently symptomatic cows.
Trueperella (formerly Arcanobacterium) pyogenes is common in suppurative processes of cattle and pigs and produces a characteristic mastitis in heifers and dry cows. It occasionally infects lactating udders after teat injury, and it may be a secondary invader. The inflammation is typified by the formation of profuse, foul-smelling, purulent exudate. Mastitis due to T pyogenes is common among dry cows and heifers that are pastured during the summer months on fields and that have access to ponds or wet areas. The vector for animal-to-animal spread is the fly Haematobia irritans. Control of infections is attained by limiting the ability to stand in water and by controlling flies. Therapy is rarely successful, and the infected quarter is usually lost to production. Infected cows may be systemically ill, and cows with abscesses usually should be slaughtered. (Also see Actinomycosis.)
Mycoplasma spp can cause a severe form of mastitis that may spread rapidly through a herd with serious consequences. M bovis is the most common cause. Other significant species include M californicum, M canadense, and M bovigenitalium. Onset is rapid, and the source of infection is often endogenous after outbreaks of respiratory disease in heifers or cows. The disease is often seen in herds undergoing expansion in which animals from outside sources have been added. Typically, introduced animals will be asymptomatic carriers and then shed the organism via respiratory or intramammary transmission. Some or all quarters become involved. Loss of production is often dramatic, and the secretion is soon replaced by a serous or purulent exudate. Initially, a characteristic, fine granular or flaky sediment may be seen in the material removed from infected glands.
Despite the severe local effects on udder tissue, cows usually do not manifest signs of systemic involvement. The infection may persist through the dry period. Identification of all infected cows in a herd can be difficult because of the frequent propensity of these cows to become asymptomatic carriers and intermittently shed the organism in milk.
Because there is no satisfactory treatment, affected cows should be segregated during active outbreaks. Routine screening of the bulk tank and milk strings may help identify the presence of infected cows. However, milk culture of cows with clinical mastitis, or recently calved cows, offers the most reliable surveillance. If cows continue to display clinical mastitis or systemic signs, they should be culled. Sanitary measures should be strictly enforced, especially at milking and in hospital/treatment areas. Milk from Mycoplasma-infected cows should not be fed to calves, because this may result in pneumonia or otitis media. Milk replacer or pasteurized milk, rather than discarded milk, should be fed to calves in herds with Mycoplasma.
Nocardia asteroides causes a destructive mastitis characterized by acute onset, high temperature, anorexia, rapid wasting, and marked swelling of the udder. Typically, a granulomatous inflammation of the udder occurs that leads to extensive fibrosis and formation of palpable nodules. Infection of the udder may be associated with failure to ensure asepsis in intramammary treatment of the common forms of mastitis. Slaughter is recommended for infected cows.
Serratia mastitis may arise from contamination of milk hoses, teat dips, water supply, or other equipment used in the milking process. The organism is resistant to disinfectants. Cows with this form of mastitis that continue to display clinical signs should be culled.
Mastitis due to various mycotic organisms (yeasts) has appeared in dairy herds, especially after the use of penicillin in association with prolonged repetitive use of antimicrobial infusions in individual cows. Yeasts grow well in the presence of penicillin and some other antimicrobials; they may be introduced during udder infusions of antibiotics, multiply, and cause mastitis. Yet, heifers that have never received intramammary infusions may develop yeast mastitis. Signs may be severe, with a fever followed either by spontaneous recovery in ~2 weeks or, more rarely, by a chronic destructive mastitis. Other yeast infections cause minimal inflammation and are self-limiting. If mastitis due to yeast is suspected, antibiotic therapy should be stopped immediately.
A chronic mastitis similar to that caused by the tubercle bacillus has been reported to be caused by acid-fast Mycobacterium spp derived from the soil, such as M fortuitum, M smegmatis, M vaccae, and M phlei when such organisms are introduced into the gland along with antibiotics (especially penicillin) in oil or "home remedy" vehicles. These organisms otherwise tend to be saprophytic and to disappear from infected quarters, at least by the next lactation. In the meantime, mastitis is usually moderate. Distinct outbreaks do occur and several have been reported, especially with M fortuitum and M smegmatis.
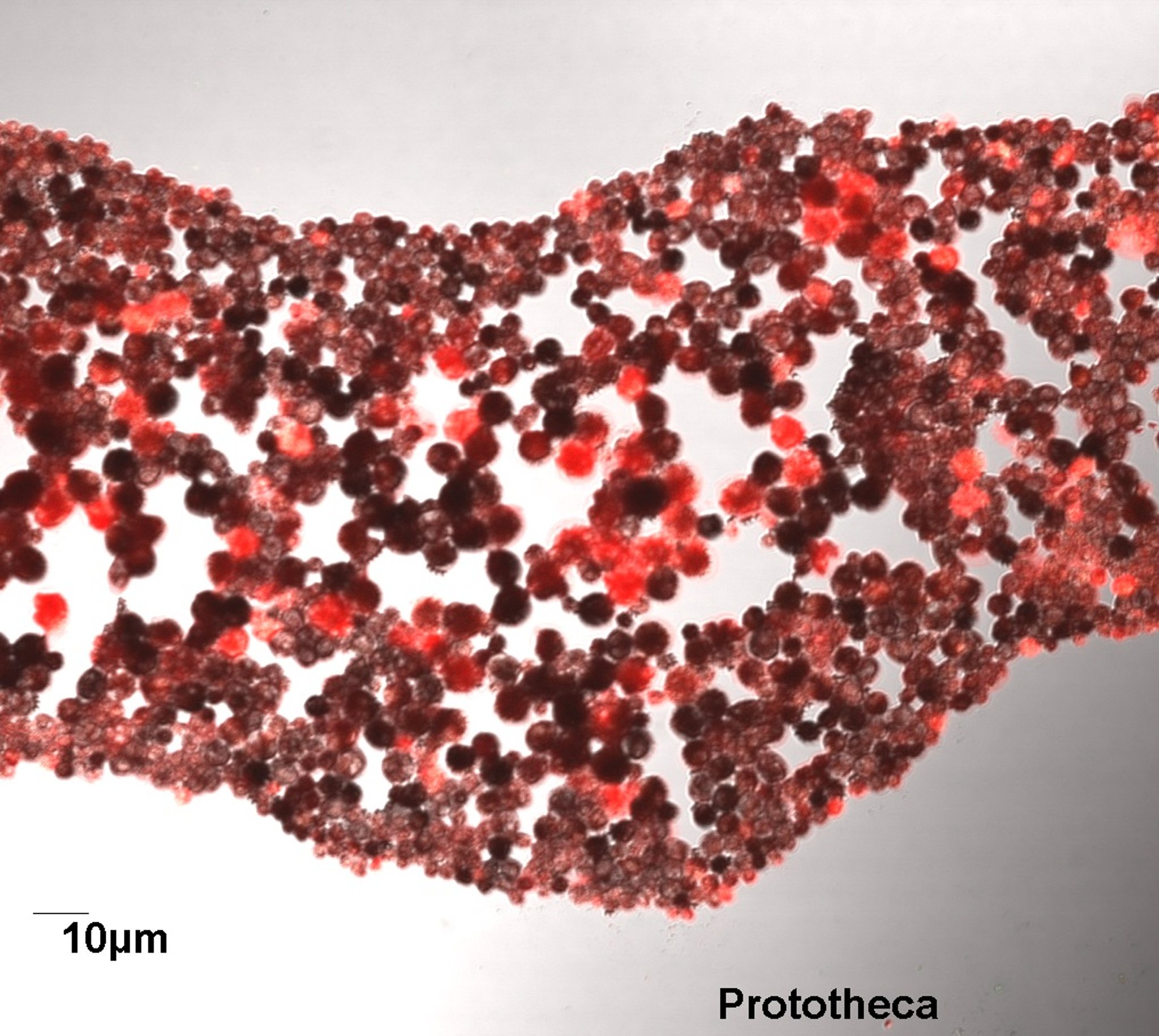
Prototheca sp are nonpigmented unicellular algae commonly found in wet environments such as streams, stagnant ponds, and marine waters, particularly in humid habitats with organic matter in the soil. In dairy farm environments, they are especially abundant in muddy or wet outdoor runs or lots, resting areas, paths where animals are driven, and pastures contaminated with slurry. Infections during the dry period are possible, especially in cows exposed to manure pack bedding or outside lots. Additionally, poor infusion asepsis and use of multidose antimicrobial products not intended for intramammary infusion have been linked to outbreaks. Case reports suggest that should IMI in a herd reach critical levels, contagious transmission of Prototheca during milking may also occur.
Protothecal mastitis in dairy cattle is often chronic and asymptomatic with increased SCCs, although sporadic severe infections occur. Infections may spontaneously resolve, but longterm carriage with intermittent shedding is common. After initially causing clinical mastitis, infections may be undetectable by culture of milk for several months, only to recur during the subsequent lactation, particularly soon after calving. Therapeutic interventions are unrewarding. Thus, dairy producers have limited ability to predict the progression or affect the outcome of protothecal mastitis and are constrained to management options similar to those used to manage chronic mastitis caused by other pathogens. Therefore, prevention is the primary focus rather than mitigation of infections. To reduce pathogen exposure to other noninfected cows in the herd, chronic mastitis cows are often culled.
The primary causative agent of protothecal mastitis in cattle has been identified as P zopfii. Other reports have challenged the absolute exclusivity of P zopfii as the etiologic agent of protothecal mastitis, but on a practical basis, cows identified as having mastitis caused by Prototheca sp are managed in similar fashion, regardless of species or genotype. Often, Prototheca are misidentified on routine milk culture, and either selective media, or the use of a gram stain to identify large organisms (relative to typical bacteria), should be used.
Mastitis caused by Bacillus spp has much the same origin, clinical presentation, and methods of prevention as do other unusual pathogens. As with other organisms in this category, treatment is not generally successful.

Courtesy of Dr. Ronald Erskine.
Prevention of Clinical Mastitis in Cattle
Prevention for clinical mastitis is essentially identical to that for subclinical mastitis, ie, reducing microbe exposure to the teats. Because most clinical mastitis is caused by pathogens that are predominately environmental in origin, decreasing exposure from bedding, housing, or in outdoor lots and pastures is critical. However, good premilking hygiene to ensure teats are clean and dry before a milking unit attachment, including use of germicides (premilking teat dips) is beneficial.
With the exception of bacterins that target gram-negative pathogens, particularly coliforms, immunization to reduce the effects of mastitis has been largely unsuccessful or, at best, variable. Core-antigen technology based on J5 mutant E coli can help reduce the severity of clinical mastitis caused by coliforms. Immunization with these bacterins should minimally include multiple doses during the dry period to reduce the incidence of clinical coliform mastitis frequently associated with early lactation. Protocols for extended numbers of immunizations of these bacterins may be warranted in herds with high rates of severe mastitis beyond 60 days in milk, because protection often wanes 50–60 days after the last immunization. It is important to note that these bacterins reduce the severity of clinical mastitis cases caused by gram-negative pathogens only. Also, although severity of clinical signs can be reduced, these bacterins do not prevent infections.
The success of core-antigen bacterins relies on five fundamental principles:
Validate that coliform organisms are the primary cause of severe clinical mastitis in a herd by culture of milk samples.
Determine whether the incidence of severe coliform mastitis is >1% of the herd each year.
Describe the animals at risk, eg, days in milk and lactation.
Decrease other herd risk factors for coliform mastitis, such as inadequate bedding.
Develop a vaccination protocol that targets animals at risk.
Recently, a vaccine that targets Klebsiella spp by immunization against siderophore (iron-trapping) proteins that are an important virulence factor for gram-negative pathogens has shown promise for reducing the severity of clinical mastitis caused by this subgroup of pathogens.