In small animals, zinc toxicosis is usually a result of ingestion of objects that contain or are coated with zinc, most commonly US pennies. In large animals, the main causes are contaminated pastures and excess dietary supplementation. Clinical signs vary depending on species, source, and amount of zinc; however, GI signs are common initially, with intravascular hemolysis, organ damage, and DIC occurring in a second phase. Lameness may be seen in foals and swine. Diagnosis is based on history of exposure, abnormalities on laboratory testing (which may include measurement of serum zinc concentration), and identification of a suspicious object on abdominal radiographs in small animals. Treatment consists of removal of the source of zinc and supportive therapy; chelation therapy is controversial.
Zinc is an essential trace element used by the body in the synthesis of several hundred enzymes. It plays an important role in an effective immune system and contributes to a number of normal bodily functions, including musculoskeletal growth, vision, and normal wound healing. It is ubiquitous in nature and exists in many forms. The ingestion of some forms of zinc causes the creation of toxic zinc salts in the acidic environment of the stomach. Zinc toxicosis has been documented in humans and in a wide range of large, small, exotic, and wild animals.
Exposure to zinc in dogs, cats, and other small animals typically stems from dietary indiscretion involving metals that either contain zinc or are coated with zinc. Galvanized metals are metals that are coated with zinc to prevent rusting. US pennies, specifically pennies minted since 1982, are a key source because they contain 97.5% zinc. This concentration is equivalent to 2,440 mg of elemental zinc per penny. US dollar coins also contain zinc, although at a much lower concentration (6%). Some international coins similarly contain zinc. Additional sources of zinc include automotive parts, galvanized nails/nuts/bolts, wire/hardware, polyhedral game dice, zippers, toys, aluminum galvanized cookware, galvanized metal cages (eg, coated birdcages), BB pellets, jewelry, and zinc-coated garland and tinsel decorations. The primary sources of zinc for large/production animals are contaminated pastures and excess supplementation of zinc in the diet.
Pathogenesis of Zinc Toxicosis in Animals
The low pH in the stomach causes the release of free zinc, which then forms soluble, caustic zinc salts, causing zinc toxicosis. Initially, irritation and possibly GI ulceration develop; however, the longer the object stays in the stomach, the more zinc is systemically absorbed via the small intestine. Overall, about 25% to 50% of ingested zinc is absorbed. Zinc then rapidly accumulates in the liver, kidneys, pancreas, and spleen. The liver extracts only about one third of the zinc from circulating blood, releasing the remainder back into the bloodstream. Zinc is eliminated chiefly through feces.
The exact means by which zinc causes intravascular hemolysis has not been completely established. In theory, acute overdoses cause direct damage to the membranes of RBCs, as well as oxidative damage to the cells. The mechanism of action by which zinc causes liver, kidney, or pancreatic damage is likewise not known, though zinc can have direct cytotoxic effects, and hemoglobinuria can cause acute kidney injury.
The LD50 of zinc salts in cases of acute toxicosis in small animals has been reported to be ~100 mg/kg. Diets containing high levels of zinc have been reported to cause chronic zinc toxicosis in large animals. The maximum tolerable amount of zinc in the diet of large animals varies, depending on the species. Zinc salts interfere with the metabolism of other ions, such as copper, calcium, and iron, and can lead to dietary deficiencies of these minerals.
Clinical Findings and Lesions of Zinc Toxicosis in Animals
The nature and severity of the clinical signs of zinc toxicosis vary, depending on both the source and the species of animal involved in the exposure. Acute ingestion of zinc oxide ointment or cream, zinc lozenges, or zinc supplements represents a low toxicity risk and rarely causes more than dose-dependent GI upset (nausea, vomiting, diarrhea). Occasionally, zinc oxide cream or ointment may also cause an allergic reaction (facial swelling, hives, erythema, pruritus). Ingestion of metal objects containing zinc or high dietary levels of zinc cause the more classic clinical signs of zinc toxicosis (eg, intravascular hemolysis).
Gross pathologic findings in dogs and cats include nonspecific hepatomegaly; splenomegaly; pancreatic nodules; red-brown kidneys; and inflammation, edema, or ulceration of the GI mucosa. Histopathology findings can include hemoglobin nephropathy, pancreatic acinar cell necrosis, pancreatic interstitial fibrosis, and hepatic necrosis with pigment accumulation. Macrophages in multiple organs may contain large amounts of hemosiderin. Gross lesions in horses manifest in all limb joints as severe generalized osteochondrosis. Possible lesions in cows include renal hemorrhages, pancreatic lesions, hepatic degeneration, and pulmonary emphysema.
Clinical signs of zinc toxicosis in dogs and cats develop in two phases. An initial phase is characterized by vomiting, diarrhea, anorexia, lethargy, and weight loss, which can progress to ulcers and melena. These GI signs can develop within minutes to several hours or even several days, depending on the source of the zinc. A second phase develops several hours to several days after the GI phase, because metallic objects can take days for zinc leaching to cause clinical signs. This phase is characterized by intravascular hemolysis, anemia (with or without an associated heart murmur), tachycardia, icterus, hemoglobinuria, hemoglobinemia, acute kidney and/or liver failure, pancreatitis, and DIC. Death can result.
Pet birds suffering from acute zinc toxicosis can present with shallow respirations, partially fluffed feathers, and closed eyes. They are reluctant to move, and they sit on the floor of the cage. Anorexia, ataxia, vomiting and regurgitation, recumbency, weight loss, and polyuria/polydipsia can occur. Liver and kidney injury, pancreatitis, and death are possible. Chronic exposure results in a different presentation, with more intermittent clinical dullness and dysphagia. Death is less common with chronic zinc toxicosis.
Ferrets can develop the same GI clinical signs of zinc toxicosis as dogs and cats, plus GI bleeding, kidney injury, and pancreatitis.
Foals are extremely susceptible to zinc toxicosis from chronic exposure. Joint enlargement progressing to painful joint erosions, weakened cartilage, lameness, and limb deformities may develop over the course of several weeks.
Swine exposed to excess zinc show reduced weight gain, lameness, decreased litter size, GI irritation/inflammation, and an unthrifty appearance.
Ruminants with acute zinc toxicosis can develop weight loss, diarrhea, decreased appetite, decreased milk production, polyuria with secondary dehydration, and generalized listlessness. Chronic overdosing of zinc in ruminants (via dietary zinc / zinc supplements) can lead to cellular degeneration of the liver, pancreas, and kidneys. Pregnant and young animals are at greatest risk.
In laying hens, zinc toxicosis can cause decreased egg production, decreased appetite, and weight loss.
Diagnosis of Zinc Toxicosis in Animals
History of exposure
Laboratory testing (eg, CBC, serum chemistries, urinalysis, clotting tests)
Abdominal radiographs
Serum zinc concentration

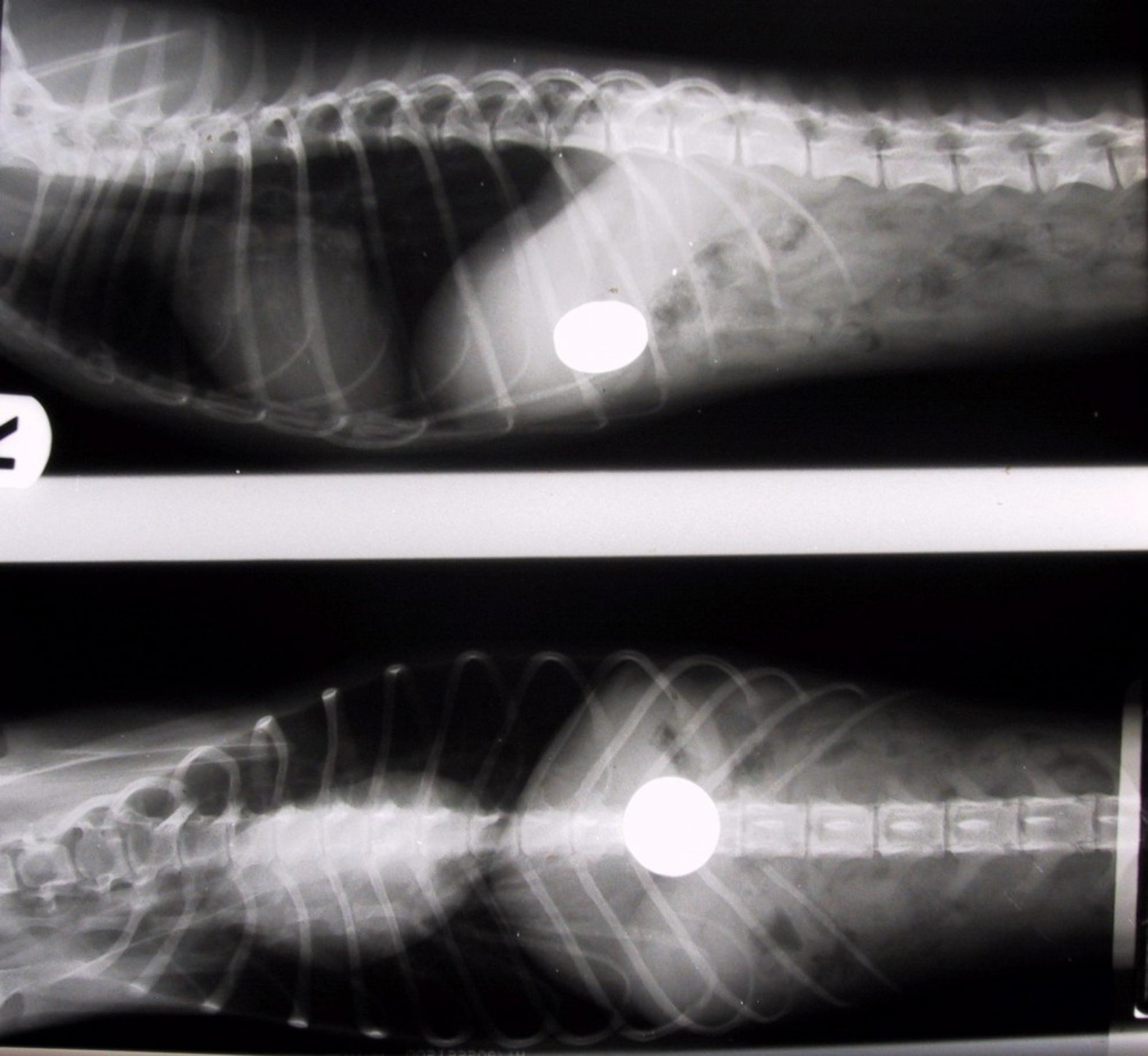
Courtesy of Dr. Raymond Cahill-Morasco.
Diagnosis of zinc toxicosis is based on history of exposure, laboratory abnormalities, and abdominal radiographs. A CBC may show intravascular hemolysis with a regenerative anemia, spherocytes, and Heinz bodies. A leukocytosis with neutrophilia and a left shift, monocytosis, and lymphopenia may be present. Platelets may be mildly decreased. Serum chemistry abnormalities include increased AST, AST, pancreatic enzymes, and bilirubin. The BUN may be disproportionately high compared with creatinine concentration, secondary to blood loss and/or dehydration. A Coombs test can be positive, although a saline agglutination test is usually negative. Urinalysis can show proteinuria, hemoglobinuria, and bilirubinuria, with tubular casts seen on examination of sediment. Coagulation tests (prothrombin time, partial thromboplastin time) may be prolonged secondary to liver damage.
Abdominal radiographs may show a radiodense foreign body (eg, a coin); however, the lack of a visible foreign body does not exclude zinc toxicosis as the diagnosis. If no metal is visible on radiographs or if the patient is not responding to supportive care, blood should be collected in a royal blue top tube (trace mineral testing) for determination of serum zinc concentration (>5 ppm is consistent with zinc toxicosis in dogs and cats, >6 ppm in birds).
Treatment and Prevention of Zinc Toxicosis in Animals
Antacids every 2-4 hours until removal of the zinc foreign body
Supportive treatment
For small animal patients, antacids (eg, calcium carbonate) should be administered every 2–4 hours until the zinc foreign body can be surgically or endoscopically removed from the GI tract. Supportive treatment should be administered as needed, including proton pump inhibitors, sucralfate (if GI bleeding is suspected), intravenous fluids, blood transfusion, treatment for pancreatitis, etc. Laboratory testing (e.g. CBC, serum biochemistry to monitor liver and kidney function) should be performed every 24 hours initially and then as needed until normalized.
For horses and other large animals, copper supplementation can be considered, especially if copper deficiency has been noted.
Chelation therapy is controversial. Although it can enhance elimination of zinc and promote faster recovery, it can also increase zinc absorption from the GI tract. This is especially true if a metallic foreign body is still present in the body. Chelation may be considered if the patient is not recovering as expected after removal of the zinc object(s). Ca-EDTA is the recommended chelation agent. Baseline serum zinc concentrations should be measured and rechecked after chelation.
With early diagnosis and treatment, the outcome is usually favorable for animals with zinc toxicosis. Eliminating exposure to zinc either in the environment or via excessive dietary supplementation is essential to prevent recurrence.
Key Points
Acute ingestion of zinc oxide products, zinc lozenges, or zinc supplements is a low toxicity risk.
Ingestion of metal objects containing zinc or high doses of zinc in an animal’s diet cause the more classic clinical signs of zinc toxicosis (eg, intravascular hemolysis).
For More Information
Also see pet health content regarding zinc poisoning.