




Percutaneous coronary interventions (PCI) include percutaneous transluminal coronary angioplasty (PTCA) with or without stent insertion. Primary indications are treatment of
Angina pectoris (stable or unstable)
Myocardial ischemia
Acute myocardial infarction (particularly in patients with developing or established cardiogenic shock)
PTCA and stent placement within 90 minutes of onset of pain is the optimal treatment of transmural ST-segment elevation myocardial infarction (STEMI). Elective PCI may be appropriate for post–myocardial infarction (MI) patients who have recurrent or inducible angina before hospital discharge and for patients who have angina and remain symptomatic despite medical treatment.


GJLP/CNRI/SCIENCE PHOTO LIBRARY
Percutaneous transluminal angioplasty (PTA) is also used to treat peripheral arterial disease.
Procedure for PCI
PTCA is done via percutaneous femoral, radial, or brachial artery puncture. The radial approach reduces patient discomfort, improves time to ambulation, and reduces the incidence of some complications (eg, bleeding, pseudoaneurysm formation).
A guiding catheter is inserted into a large peripheral artery and threaded to the appropriate coronary ostium. A balloon-tipped catheter, guided by fluoroscopy or intravascular ultrasonography, is aligned within the stenosis, then inflated to disrupt the atherosclerotic plaque and dilate the artery. Angiography is repeated after the procedure to document any changes. The procedure is commonly done in 2 or 3 vessels as needed.
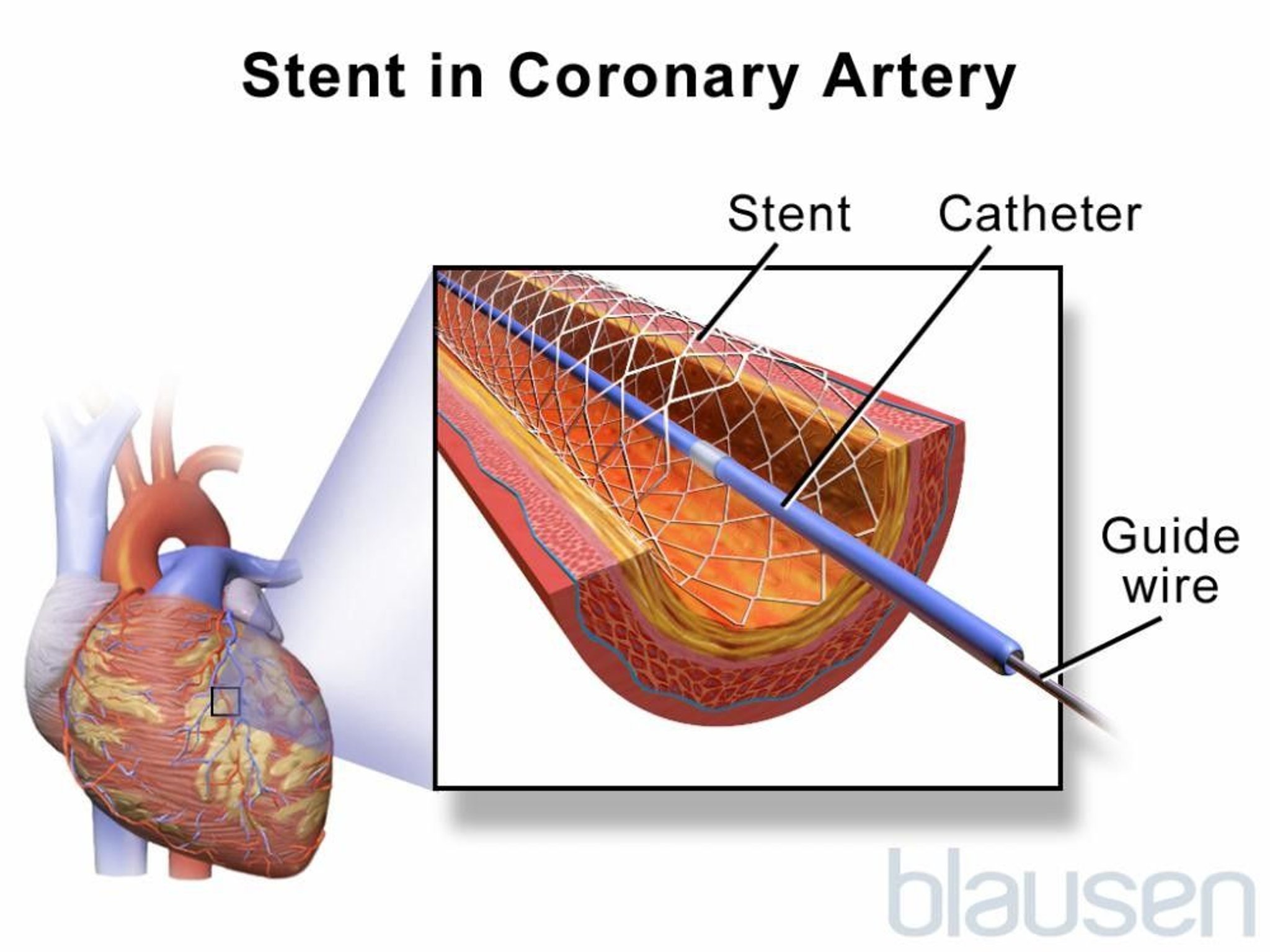
Stents for PCI
Stents for coronary arteries are expandable wire mesh cylinders that help hold stenotic areas open. Stents are most useful for
Short lesions in large native coronary arteries not previously treated with PTCA
Focal lesions in saphenous vein grafts
Treatment of abrupt closure during PTCA

Stents are used frequently for acute myocardial infarction, ostial or left main disease, chronic total occlusions, and bifurcation lesions.
Types of stents
1).
Stent reference
1. Iglesias JF, Muller O, Heg D, et al. Biodegradable polymer sirolimus-eluting stents versus durable polymer everolimus-eluting stents in patients with ST-segment elevation myocardial infarction (BIOSTEMI): a single-blind, prospective, randomised superiority trial. Lancet 2019;394(10205):1243-1253. doi:10.1016/S0140-6736(19)31877-X
Anticoagulation and ancillary therapy
Various anticoagulation and antiplatelet regimens are used during and after PCI to reduce the incidence of thrombosis at the site of balloon dilation and stent placement.
Bivalirudinheparin in patients with heparinaspirin) are continued for at least 6 to 12 months after PCI to decrease the risk of in-stent thrombosis until endothelialization of the stent has occurred.
For patients who require anticoagulation for another reason (eg, atrial fibrillation
Contraindications to PCI
Relative contraindications to PCI include
Coagulopathy
A single diseased vessel providing all perfusion to the myocardium
Critical left main coronary stenosis without collateral flow from a native vessel or previous bypass graft to the left anterior descending artery
Diffusely diseased vessels without focal stenoses
Hypercoagulable states
Lack of cardiac surgical support
Stenosis < 50%
Total occlusion of a coronary artery
Although lack of cardiac surgical support is sometimes considered an absolute contraindication to PCI, many experts advocate that when revascularization is required urgently in STEMI, experienced operators in approved catheterization laboratories should proceed with PCI even if surgical backup is not available.
Although bypass is typically preferred for patients with critical left main coronary stenosis without collateral flow from either a native vessel or previous bypass graft, PCI is often and increasingly being used in this scenario in selected patients.
Complications of PCI
The main complications of balloon angioplasty and stent placement are
Arterial dissection
Bleeding caused by adjunctive anticoagulation
Restenosis
Standard complications of cardiac catheterization and coronary angiography
Thrombosis and distal embolization
Overall, risks of undergoing PCI are comparable to those of CABG. Overall mortality rate is < 1%, but varies based on individual risk factors and tends to be similar to that of CABG; Q wave MI rate is < 1%. In < 1% of patients, intimal dissection causes obstruction requiring emergency CABG. Risk of stroke with PCI is lower than with CABG. A meta-analysis of 19 randomized trials reported a higher risk of stroke in patients undergoing CABG (1.2%) than PCI (0.34%,) at 30 days (1). Risk of bleeding is 1 to 2%.
Of all angiographic procedures, PCI has the highest risk of contrast nephropathy (due to increased contrast load and procedural time); this risk can be reduced by preprocedural hydration and possibly by use of a nonionic contrast agent or hemofiltration in patients with preexisting renal insufficiency.
Compared to coronary angiography without angioplasty or stent placement, risk of death, MI, and stroke is greater.
Thrombosis
Stent thrombosis causes complete blockage and may occur at any time:
Acutely (immediately during or after the procedure)
Subacutely (within 30 days)
Late (> 30 days)
Very late ( > 1 year)
Stent thrombosis may be due to inadequate stent expansion or incomplete stent apposition at the time of the procedure, discontinuation of dual antiplatelet therapy (eg, due to nonadherence, need for noncardiac surgery), or both. Rarely, the stent may break up an intracoronary clot (ie, as may be present in acute MI), which may embolize distally and cause myocardial infarction. Use of protection strategies (eg, temporarily blocking blood flow within the artery using a balloon and then aspirating the emboli, deploying a small filter distal to the site of PCI to capture emboli) may improve outcome in PCI done on a previous saphenous vein graft but is not commonly done.
With balloon angioplasty alone, risk of acute thrombosis is about 5 to 10%.
Use of stents has almost eliminated the need for emergency coronary artery bypass grafting following PCI; the rate of acute and subacute thrombosis is < 1%. However, using a drug-eluting stent increases risk of late stent thrombosis, about 0.6%/year up to 3 years.
Restenosis
Restenosis is typically due to collagen deposition and thus does not occur until several weeks after the procedure or later; it may cause partial or, less commonly, complete vessel blockage.
With balloon angioplasty alone, the risk of subacute restenosis is about 5%, and the overall restenosis rate is about 30 to 45%.
With stent use, the rate of subacute restenosis is < 1%. With bare-metal stents, risk of late restenosis is 20 to 30%. Use of a drug-eluting stent lowers late restenosis risk significantly.
Arterial dissection
In < 1% of patients, intimal dissection causes obstruction requiring emergency CABG. Arterial dissection is usually detected immediately as various abnormal patterns of contrast filling within the coronary arteries. Insertion of another stent often reopens the dissected segment.
Stroke
Risk of stroke with PCI is lower than with CABG. A meta-analysis of 19 randomized trials reported a higher risk of stroke in patients undergoing CABG (1.2%) than PCI (0.34%,) at 30 days (1).
Complications reference
1. Palmerini T, Biondi-Zoccai G, Reggiani LB, et al: Risk of stroke with coronary artery bypass graft surgery compared with percutaneous coronary intervention. J Am Coll Cardiol 60(9):798–805, 2012. doi:10.1016/j.jacc.2011.10.912






