




When a neurologic disorder is suspected, doctors usually evaluate all of the body systems during the physical examination, but they focus on the different parts of the nervous system. Examination of the nervous system—the neurologic examination—includes evaluation of the following:
Doctors may evaluate some areas more thoroughly than others depending on what type of disorder they suspect. For example, the neurologic examination can also help identify the cause of a muscle malfunction (such as weakness or paralysis) because normal muscle contraction depends on stimulation by a nerve (see figure Using the Brain to Move a Muscle).
A neurologic examination differs from a psychiatric examination, which focuses on a person's behavior. However, the two examinations overlap somewhat because abnormalities in the brain can cause abnormal behavior. Abnormal behavior can be a clue to a physical problem in the brain.
Mental Status
Doctors evaluate the following:
Attention
Orientation to time, place, and person
Memory
Various abilities, such as thinking abstractly, following commands, using language, and solving math problems
Mood
The mental status evaluation consists of a series of questions and tasks, such as naming objects, recalling short lists, writing sentences, and copying shapes. The person’s answers are recorded and scored for accuracy. If the person reports feeling depressed, doctors ask if there have been any thoughts of suicide.
Cranial Nerves
There are 12 pairs of cranial nerves, which connect the brain with the eyes, ears, nose, face, tongue, throat, neck, upper shoulders, and some internal organs (see table Viewing Cranial Nerves). How many nerves doctors test depends on what type of disorder they suspect. For example, the 1st cranial nerve (the nerve of smell) is not usually tested when a muscle disorder is suspected, but it is tested in people recovering from serious head trauma (because smell is often lost).
A cranial nerve may be damaged anywhere along its length as a result of any of the following:
An injury
Impaired blood flow
An autoimmune disorder
A tumor
An infection
Increased pressure in the skull (intracranial pressure)
The exact site of the damage can often be identified by testing the functions of a particular cranial nerve.
Motor Nerves
Motor nerves carry impulses from the brain and spinal cord to voluntary muscles (muscles controlled by conscious effort), such as muscles of the arms and legs. Muscle weakness or paralysis of a muscle may indicate damage to any of the following:
The muscle itself
A motor nerve
The nerve's connection to the muscle (neuromuscular junction)
The brain
The spinal cord
Doctors look for abnormalities such as the following:
A decrease in muscle size (wasting, or atrophy)
An increase in muscle size
Tremor (rhythmic shaking of a body part) and other unintended (involuntary) muscle movements
Muscle twitching
An increase (spasticity or rigidity) or a decrease in muscle tone
Weakness, particularly which body parts are affected (pattern of weakness)
Loss of dexterity (the ability to use the hands skillfully and nimbly)
The doctor inspects the muscles for size, unusual movements, tone, strength, and dexterity.
Change in muscle size
A muscle wastes away (atrophies) when the muscle or the nerves supplying it are damaged or when the muscle has not been used for months for other reasons (such as being in a cast).
A muscle may increase in size (hypertrophy) because it is working harder to compensate for the weakness of another muscle. Muscles can appear to increase is size when normal muscle tissue is replaced by abnormal tissue, as occurs in amyloidosis and some inherited muscle disorders (such as Duchenne muscular dystrophy). The abnormal tissue increases the apparent size but not the strength of the muscle.
Involuntary movements
Muscles may move without the person meaning them to (involuntarily). The following are examples of involuntary movements:
Fasciculations are tiny, subtle muscle twitches, which may look ripples under the skin. Fasciculations may indicate nerve damage to the affected muscle.
Myoclonus refers to sudden jerking (contractions) of a muscle or a group of muscles, such as those in the hand, arm, or leg. The muscles move as if the person had just received an electric shock. Myoclonus may occur normally, as when people are falling asleep, or may be caused by a disorder that affects the spinal cord or brain.
Tics are purposeless, repetitive but not rhythmic involuntary movements, such as blinking or jerking the head. Tics often also include involuntary, abrupt, often repetitive sounds and/or words.
Hemiballismus usually involves the sudden involuntary flinging of one arm and/or one leg.
Chorea refers to quick fidgety involuntary movements that start in one part of the body and often move abruptly and unpredictably to another part.
Athetosis refers to continuous slow, writhing involuntary movements.
Dystonia refers to long-lasting (sustained) involuntary muscle contractions that may force people into abnormal, sometimes painful positions.
Involuntary movements may indicate damage in the areas of the brain (basal ganglia) that control motor coordination.
Muscle tone
To evaluate muscle tone, doctors first ask the person to completely relax muscles in a limb. Then doctors move the person’s limb to determine how much the relaxed muscle involuntarily resists being moved—called muscle tone. How muscle tone reacts to being moved suggests possible causes, as follows:
Uneven muscle tone that suddenly increases as the relaxed muscle is moved (spasticity): Possibly due to a stroke or spinal cord injury
Evenly increased muscle tone: Possibly due to a disorder of the basal ganglia, such as Parkinson disease
Severely reduced muscle tone (flaccidity): Possibly due to a disorder of the nerves outside of the brain and spinal cord (peripheral nerves), such a polyneuropathy (a disorder that affects many nerves throughout the body)
Flaccidity may be present for a short time after an injury that causes paralysis, such as a spinal cord injury. When flaccidity results from such a spinal cord injury, muscle tone often gradually increases over days to weeks, eventually resulting in spasticity.
If people are afraid or confused during the examination, they may not be able to relax the muscles. In such cases, muscle tone may vary, making it hard for doctors to evaluate.
Muscle strength
Doctors test muscle strength by asking the person to push or pull against resistance or to do maneuvers that require strength, such as walking on the heels and tiptoes or rising from a chair. Doctors then rate muscle strength from 0 (no muscle contraction) to 5 (full strength).
Sometimes muscle weakness is evident when a person uses one limb more than another. For example, a right-handed person may gesture mostly with the left hand during a conversation. A weak arm may swing less while walking or drift downward when the arms are held up and the eyes are closed.
Knowing which body parts are weak (the pattern of weakness) can help doctors identify what the problem is, as in the following cases:
The shoulders and hips are weaker than the hands and feet: The cause may be a disorder that affects muscles (myopathy). Myopathies tend to affect the largest muscles first. People may have difficulty raising their arms to comb their hair, climbing stairs, or getting up from a seated position.
The hands and feet are weaker than the shoulders, arms, and thighs: The problem is often a polyneuropathy (the malfunction of many peripheral nerves throughout the body). Polyneuropathies tend to affect the longest nerves first (those going to the hands and feet). People may have a weak grip and have trouble with fine finger movements (dexterity). People may have difficulty fastening a button, opening a safety pin, or tying their shoes.
Weakness is limited to one side of the body: Doctors suspect a disorder affecting the opposite side of the brain, such as a stroke.
Weakness occurs below a certain level of the body: The cause may be a spinal cord disorder. For example, an injury to the part of the spine in the chest (thoracic spine) causes the legs but not the arms to be paralyzed. An injury in or above the neck causes paralysis of all four limbs.
Muscle weakness may also occur in other patterns, such as the following:
Weakness occurs in only one relatively small area: This type of weakness suggests that only one or a few peripheral nerves are damaged. In such cases, weakness may also impair dexterity.
Weakness becomes apparent only when muscles that are used to do the same activity over and over become weak more quickly than usual. For example, people who once could use a hammer well become weak after hammering for several minutes. Myasthenia gravis can cause this type of weakness.
Weakness accompanied by increased muscle tone (making arms or legs stiff) and exaggerated reflexes suggest a problem in the central nervous system. Weakness accompanied by decreased muscle tone (making arms or legs feel loose or floppy), decreased or absent reflexes, and intermittent twitching in the muscle suggest a problem in the peripheral nervous system.
Sensory Nerves
Sensory nerves carry information from the body to the brain about such things as touch, pain, heat and cold (temperature), vibration, the position of body parts, and the shape of objects. Each of these senses can be tested. Abnormal sensations or reduced perception of sensations may indicate damage to a sensory nerve, the spinal cord, or certain parts of the brain.
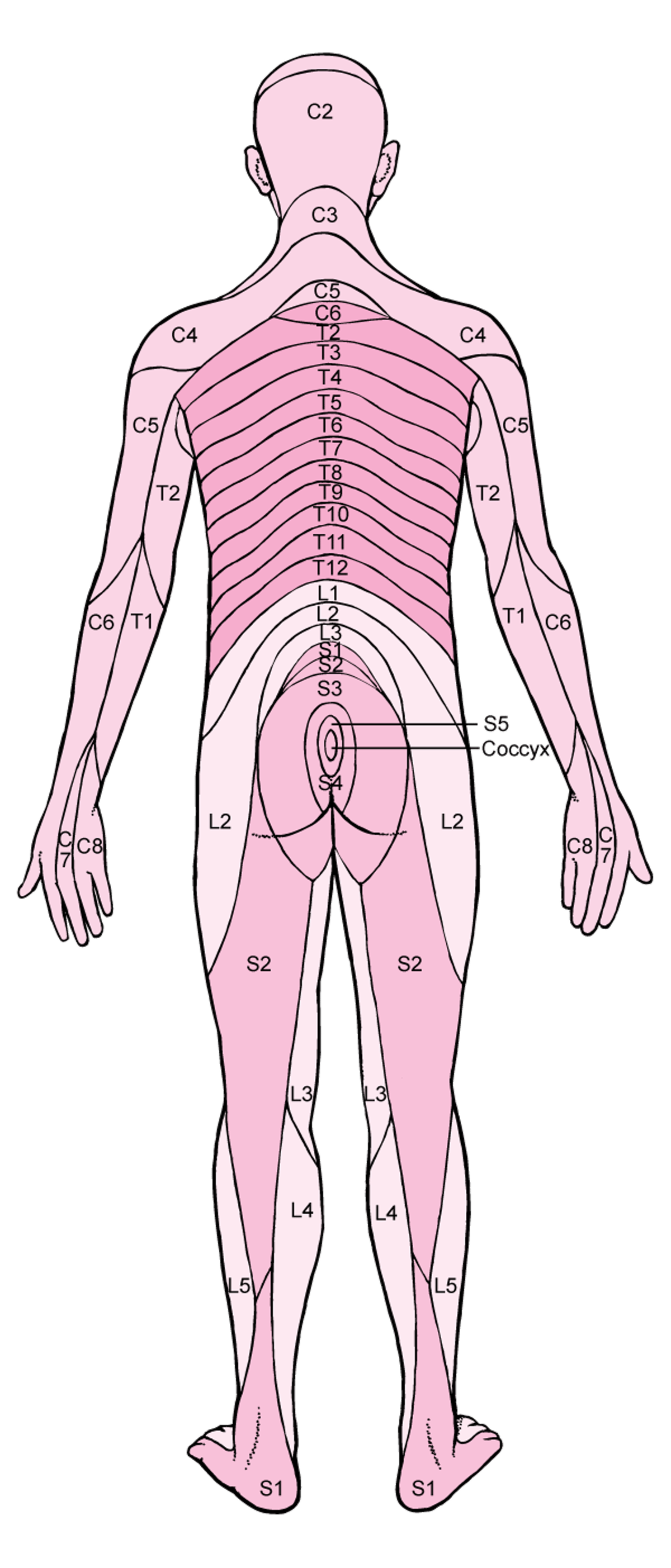
Information from specific areas on the body’s surface, called dermatomes, is carried to a specific location (level) in the spinal cord, then to the brain. Thus, doctors may be able to pinpoint the specific level of damage to the spinal cord by identifying the areas where sensation is abnormal or lost.
Dermatomes
The surface of the skin is divided into specific areas, called dermatomes. A dermatome is an area of skin whose sensory nerves all come from a single spinal nerve root. Sensory nerves carry information about such things as touch, pain, temperature, and vibration from the skin to the spinal cord. Spinal roots come in pairs—one of each pair on each side of the body. There are 31 pairs:
There are dermatomes for each of these nerve roots. Sensory information from a specific dermatome is carried by sensory nerve fibers to the spinal nerve root of a specific vertebra. For example, sensory information from a strip of skin along the back of the thigh, is carried by sensory nerve fibers to the 2nd sacral vertebra (S2) nerve root. |

Sensation in the skin is tested. Usually, doctors concentrate on the area where the person feels numbness, tingling, or pain. The best screening test for loss of sensation involves touching the skin of the face, body, and all four limbs with a pin and a blunt object (such as the head of a safety pin) to see if the person can feel them and tell the difference between sharp and dull. Doctors test both sides of the body. If doctors detect loss of sensation in a specific area, they test nearby areas to estimate the extent of the loss. This approach enables them to determine the abnormality's location in the brain, spinal cord, or peripheral nervous system.
Gentle (light) touch is tested with a cotton wisp.
Temperature sense (the ability to feel hot and cold) is tested with a tuning fork. Both prongs are cold, so the examiner warms one of them slightly by rubbing it. Then each of the prongs is touched to the person's skin.
Vibration sense is also tested with a tuning fork. The fork is lightly tapped to make it vibrate. It is then placed on the joint of a finger to determine whether and how long the person feels the vibration.
To test position sense, doctors move the person’s finger or toe up or down and ask the person to describe its position without looking.
The ability to identify the shape of an object is tested by placing a familiar object, such as a key or safety pin, in a person's hand and asking the person to identify it without looking. Or doctors may trace letters or numbers on the palm of the person's hand and ask the person to identify them. If a person cannot identify them, the cortex of the brain (the outer layer of the cerebrum, the largest part of the brain) may be damaged. This part of the brain integrates and interprets sensory information from different sources.
Reflexes
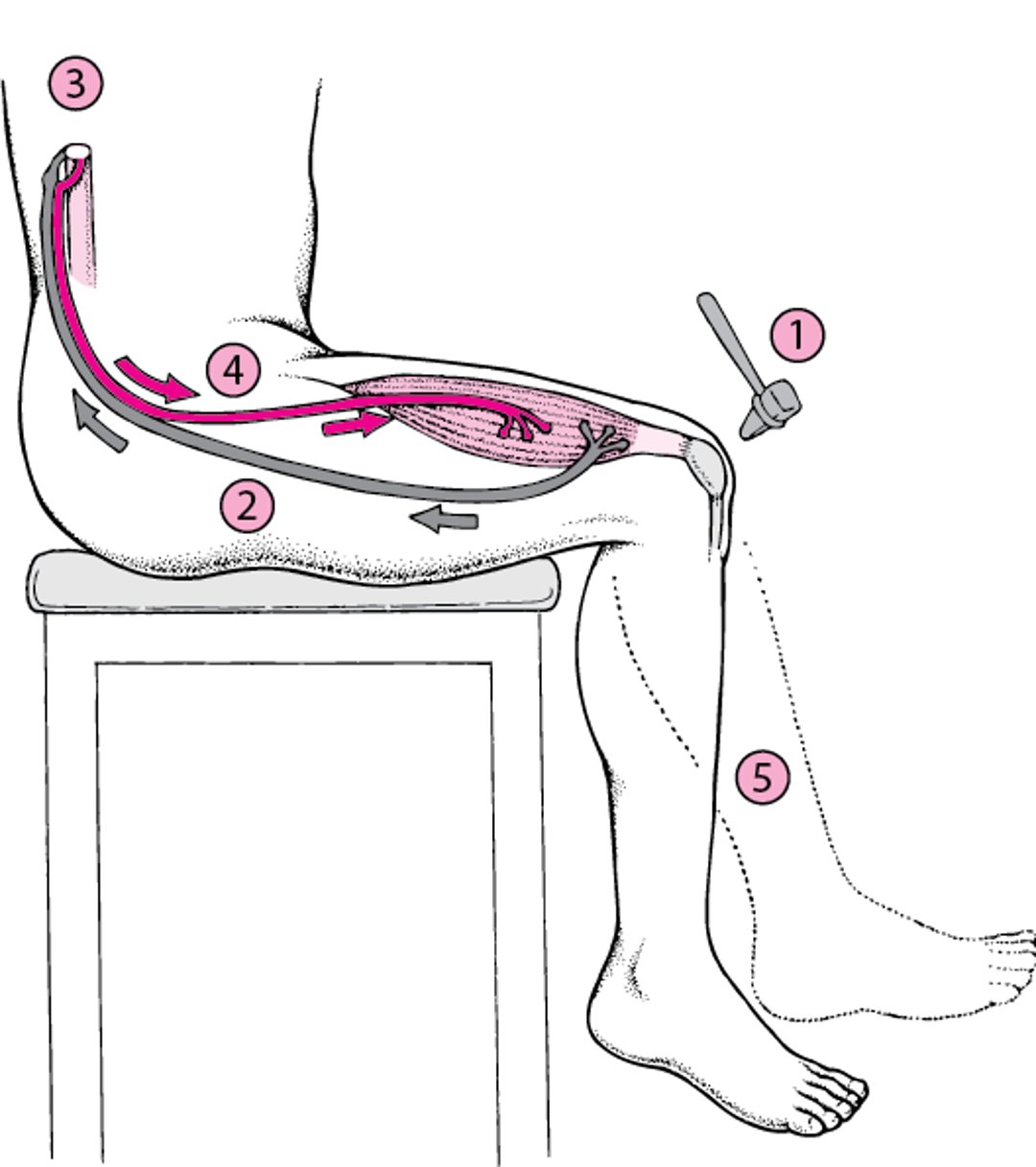
A reflex is an automatic response to a stimulus. For example, the lower leg jerks when the tendon below the kneecap is gently tapped with a small rubber hammer. The pathway that a reflex follows (reflex arc) does not directly involve the brain. The pathway consists of the sensory nerve to the spinal cord, the nerve connections in the spinal cord, and the motor nerves back to the muscle, causing the knee to jerk.
Doctors test reflexes to determine whether all parts of this pathway are functioning. The reflexes most commonly tested are the knee jerk and similar reflexes at the elbow and ankle.
The plantar reflex may help doctors diagnose abnormalities in the nerve pathways involved in the voluntary control of muscles. It is tested by firmly stroking the outer border of the sole of the foot with a key or other object that causes minor discomfort. Normally, the toes curl downward, except in infants aged 6 months or younger. Having the big toe go upward and the other toes spread out is a sign of an abnormality in the brain or spinal cord.
Testing other reflexes can provide important information. For example, doctors learn the extent of injury in a comatose person by noting the following:
Whether the pupils constrict when light is shined on them (pupillary light reflex)
Whether the eyes blink when the cornea is touched with a wisp of cotton (corneal reflex)
How the eyes move when the person’s head is turned or when water is flushed into the ear canal (caloric testing)
Whether the person gags when the back of the throat is touched, for example, with a tongue depressor (gag reflex)
Doctors also check whether the anus tightens (contracts) when it is lightly touched (called the anal wink). If this reflex is present in a person paralyzed after a spinal cord injury, the injury may be incomplete, and the chance of recovery is better than if the reflex were absent.
Reflex Arc: A No-Brainer
A reflex arc is the pathway that a nerve reflex, such as the knee jerk reflex, follows.
|

Coordination, Balance, and Gait
Coordination and walking (gait) require integration of signals from sensory and motor nerves by the brain and spinal cord.
To test walking, doctors ask a person to walk normally and in a straight line, placing one foot in front of the other. Abnormalities may help identify which part of the nervous system is not functioning normally. For example, if a person takes wide, unsteady steps (called ataxia), the cerebellum may be damaged or malfunctioning. (The cerebellum is the part of the brain that coordinates voluntary movements and controls balance.)
To test coordination, doctors may ask the person to use the forefinger to reach out and touch the doctor’s finger, then the person’s own nose, and then to repeat these actions rapidly. The person may be asked to do these actions first with the eyes open, then with the eyes closed.
The Romberg test is done to test position sense. The person stands still with both feet together as close as possible without losing balance. Then the eyes are closed. If balance is lost, information about position from the legs may not be reaching the brain, usually because the nerves or spinal cord is injured. However, abnormalities may also result from malfunction of the cerebellum or the balance system in the inner ears or its connections with the brain.
Autonomic Nervous System
The autonomic (involuntary) nervous system regulates internal body processes that require no conscious effort, such as blood pressure, heart rate, breathing, and temperature regulation through sweating or shivering. An abnormality of this system may cause problems such as the following:
A fall in blood pressure when a person stands up (orthostatic hypotension)
Reduction or absence of sweating
Sexual problems such as difficulty initiating or maintaining an erection (erectile dysfunction)
A pupil that does not widen or narrow in response to changes in light
Doctors may do a variety of tests, such as the following:
Measuring blood pressure and heart rate while the person is lying down, sitting, and standing
Examining the pupils for abnormal responses or lack of response to changes in light
Doing sweat testing
Removing and examining a small sample of skin (skin punch biopsy) to see whether the number of nerve endings has decreased, as occurs in some polyneuropathies that affect small nerves, including autonomic nerves
Blood Flow to the Brain
A severe narrowing of the arteries to the brain reduces blood flow and increases the risk of stroke. The risk is higher for people who are older, who smoke cigarettes, or who have high blood pressure, high cholesterol levels, diabetes, or disorders of the arteries or heart.
The best way to diagnose disorders of the arteries is to do an imaging test such as ultrasonography, magnetic resonance angiography (MRA), computed tomography angiography (CTA), or cerebral angiography.
Blood pressure may be measured in both arms to check for blockages in the large arteries that branch off from the aorta. Such blockages sometimes result in stroke.







