

In inflammatory bowel disease, the intestine (bowel) becomes inflamed, often causing recurring abdominal pain and diarrhea.
The 2 primary types of inflammatory bowel disease (IBD) are
These 2 diseases have many similarities and sometimes are difficult to distinguish from each other. However, there are several differences. For example, Crohn disease can affect almost any part of the digestive tract, whereas ulcerative colitis almost always affects only the large intestine.
The cause of IBD is not known, but evidence suggests that normal intestinal bacteria inappropriately trigger an immune reaction in people with a genetic predisposition. Several risk other risk factors have been identified.
IBD affects people of all ages but the incidence usually peaks between the ages of 15 and 30. A few people have their first attack during the second period of peak incidence, between the ages of 50 and 70.
IBD is most common among people of North America and Northern Europe. It is 2 to 4 times more common among people of Ashkenazi Jewish ancestry from Central or Eastern Europe than among non-Jewish White people from the same region. Both sexes are roughly equally affected, although there may be differences specific to age, geographic region, and ulcerative colitis versus Crohn disease. The incidence is lower eastern and southern Europe than in western and northern Europe. First-degree relatives (mother, father, sister, or brother) of people with IBD have a 4- to 20-fold increased risk of developing IBD, although their absolute risk for IBD is about 5 to 7%. The tendency to run in families is much higher in Crohn disease than ulcerative colitis.
In general, risk factors for inflammatory bowel disease include a history of current or past cigarette smoking, current use of oral contraceptives, living in an urban setting, exposure to antibiotics in childhood, and vitamin D deficiency. In general, risk factors for inflammatory bowel disease include a history of current or past cigarette smoking, current use of oral contraceptives, living in an urban setting, exposure to antibiotics in childhood, and vitamin D deficiency.
Factors that may protect against inflammatory bowel disease include breastfeeding, Helicobacter pylori infection, and a high folate level.
Current cigarette smoking seems to contribute to the development or worsening of Crohn disease, but it decreases the risk of ulcerative colitis. Appendectomy performed to treat appendicitis also appears to lower the risk of ulcerative colitis, but it may be a risk factor for Crohn disease. Nonsteroidal anti-inflammatory drugs (NSAIDs) may also make IBD worse.
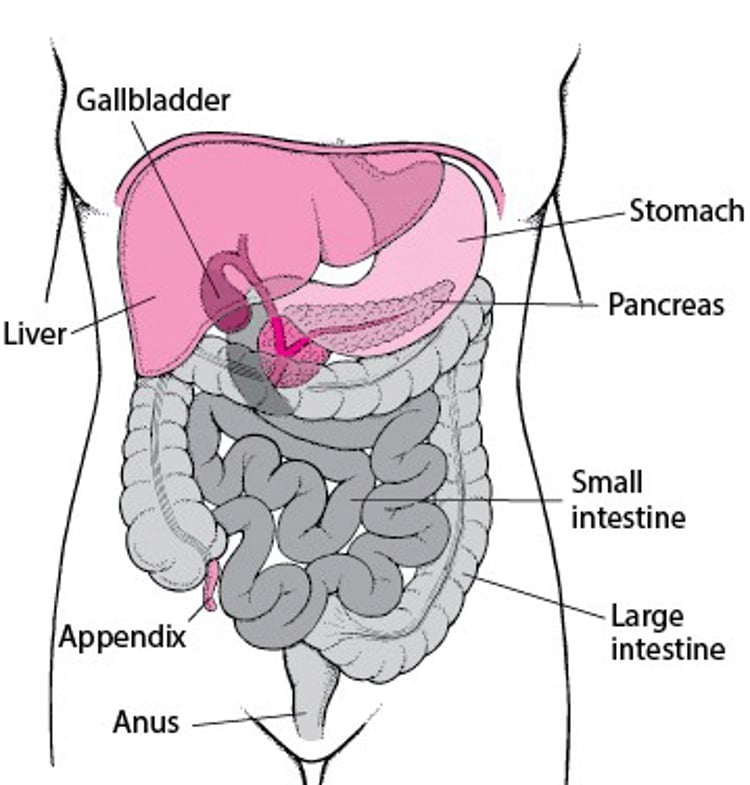
Locating the Small and Large Intestines

Symptoms of Inflammatory Bowel Disease
The symptoms of IBD vary depending on which part of the intestine is affected and whether the person has Crohn disease or ulcerative colitis. People with Crohn disease usually have chronic diarrhea and abdominal pain. People with ulcerative colitis usually have intermittent episodes of abdominal pain and bloody diarrhea. In both diseases, people with longstanding diarrhea may lose weight and become undernourished.
Sometimes IBD can affect other parts of the body such as the joints, eyes, mouth, liver, gallbladder, and skin. IBD also increases the risk of cancer in areas of the intestine that are affected.
Did You Know...
|
Diagnosis of Inflammatory Bowel Disease
Stool and blood tests
Endoscopy with tissue biopsy
Sometimes imaging tests (CT or MRI)
To make a diagnosis of IBD, a doctor must first exclude other possible causes of inflammation. For example, infection with parasites or bacteria may cause inflammation. Therefore, the doctor does several tests.
Stool samples are analyzed for evidence of a bacterial or parasitic infection (acquired during travel, for example), including a type of bacterial infection (Clostridioides difficile infection [formerly Clostridium difficile]) that can result from antibiotic use.
Tests may also be done to detect sexually transmitted infections of the rectum, such as gonorrhea, herpesvirus infection, and chlamydial infection.
Tissue samples may be taken from the lining of the digestive tract during endoscopy (an examination of the digestive tract using a viewing tube) and examined microscopically for evidence of other causes of inflammation of the colon (colitis) or inflammation of the last part of the small intestine (ileum). This removal and examination of tissue is called a biopsy.
Doctors also consider other disorders that cause similar abdominal symptoms such as irritable bowel syndrome, ischemic colitis (which occurs more often in people older than 50), malabsorption syndromes, including celiac disease, and certain gynecologic disorders in women. The doctor may do imaging studies, such as x-rays, computed tomography (CT), or magnetic resonance imaging (MRI) of the abdomen to identify the extent of disease, or to exclude other disorders. The doctor may do video capsule endoscopy to evaluate the intestines of people who have symptoms that suggest Crohn disease.
Health Maintenance in Inflammatory Bowel Disease
Inflammatory bowel disease puts people at increased risk of developing certain infections and disorders, particularly in the presence of stress, poor nutrition, underlying disease, or use of medications that alter immune system function. (These medications are called immunomodulators or immunomodulating therapies.) Vaccinations, diagnostic tests, and regular monitoring can help lessen the risk of inflammatory bowel diseases.
People at risk of decreased bone density (osteoporosis) should have a dual-energy x-ray absorptiometry (DXA) scan.
Diet and stress management
Most people and their families are interested in diet and stress management. Although some people feel that certain diets (including those with rigid carbohydrate restrictions) have helped improve their IBD, diets have not been shown to be effective in clinical trials. Doctors sometimes recommend stress-management techniques to help people deal with the stress of having a chronic disease.
Immunizations
The influenza vaccine is needed every year to help protect against the flu. The pneumococcal vaccine helps protect against bacterial infections caused by Streptococcus pneumoniae and should be given to people over the age of 50, and to people between the ages of 19 and 49 years who are taking immunomodulating therapies and have not yet received the pneumococcal vaccine. People who are age 50 and older should receive the shingles vaccine, as should people between the ages of 19 and 49 who are taking immunomodulating therapies. The shingles vaccine should be given before people start taking immunomodulating medications whenever possible.
People should also receive routine tetanus-diphtheria, hepatitis A, hepatitis B, and human papillomavirus vaccines if appropriate. It is also recommended that people with IBD, including those who are taking immunomodulating medications, receive an mRNA COVID-19 vaccine.
Cancer prevention and monitoring
All patients with IBD should undergo surveillance for colorectal cancer beginning 8 years after symptom onset, regardless of age. One exception is for patients with primary sclerosing cholangitis who should begin annual surveillance immediately at the time of diagnosis, regardless of inflammatory bowel disease duration.
Women who have IBD and who are taking immunomodulating medications should be screened for cervical cancer every year within a year of the onset of sexual activity. Women who have IBD and who are not taking immunomodulating medications should have cervical cancer screening every 3 years. Sexually active women younger than 30 who are taking immunomodulating medications should be screened yearly, but once they have tested negative for cervical cancer for 3 consecutive years, they may be able to switch to screening once every 3 years.
People who have IBD and are taking or plan to take an immunomodulating medication or biologic agent should be screened for skin cancer every year and should use sunscreen and wear protective clothing.
Treatment of Inflammatory Bowel Disease
Medications
Sometimes surgery
Although there is no cure for IBD, many medications (see table and table ), including aminosalicylates, steroids (sometimes called corticosteroids or glucocorticoids), medications that act on the body's immune system (immunomodulating medications, biologic agents, small-molecule agents), and antibiotics, can help reduce inflammation and relieve the symptoms of IBD.
People with very severe disease sometimes need surgery.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
Drugs Mentioned In This Article





