





A fibroid is a noncancerous tumor of the uterus that is composed of muscle and fibrous tissue.
Uterine fibroids are very common, occurring in approximately 70% of White women and 80% of Black women by age 50 in the United States.
Fibroids may cause no symptoms or can cause abnormal uterine bleeding or pressure or pain in the pelvis, and sometimes constipation, an urge to urinate frequently, infertility, or pregnancy complications.
Doctors do a pelvic examination and usually ultrasound to confirm the diagnosis.
Treatment is necessary only if fibroids cause problems.
Doctors may prescribe medications to control the symptoms, but surgery or a procedure to destroy or remove the fibroids is often needed to relieve symptoms or to improve fertility.

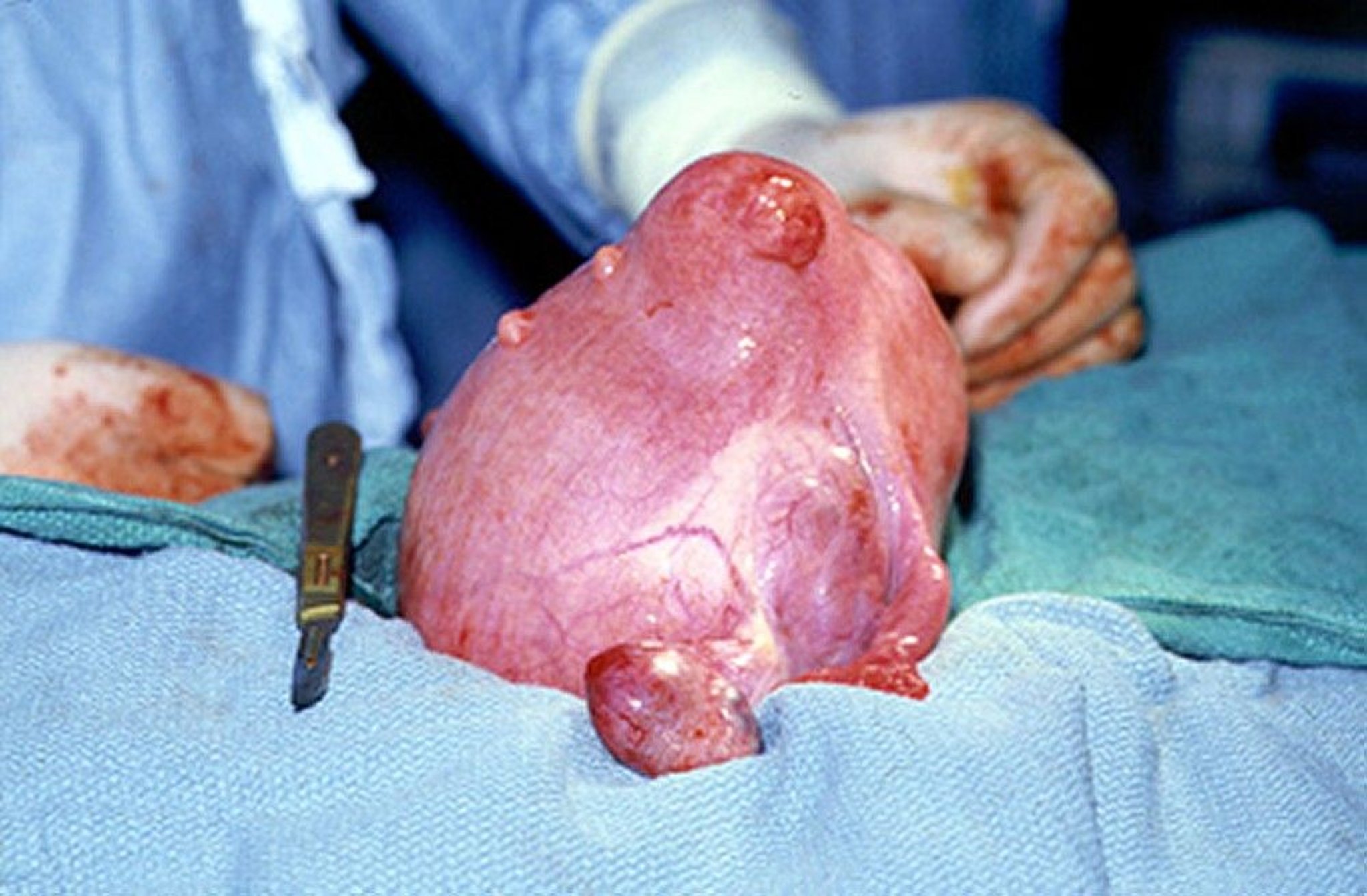
The uterus is enlarged and has an irregular shape because several fibroids are present.
(U.S. Navy photograph)
Fibroids are also called leiomyomas or myomas.


Fibroids in the uterus are the most common noncancerous tumor (mass) of the female reproductive tract. Many fibroids are small and cause no symptoms, but approximately 15 to 30% of women with fibroids develop severe symptoms.
The cause of fibroids is unknown. High levels of estrogen and possibly progesterone (female hormones) seem to stimulate their growth. Fibroids may become larger during pregnancy (when levels of these hormones increase), and fibroids tend to shrink after menopause (when levels decrease drastically).
Fibroids may be microscopic or as large as a basketball. Most women with a fibroid have more than one fibroid. Sometimes, if fibroids grow too large, the fibroids may not be able to get enough blood. As a result, they begin to degenerate (tissue starts to die without enough blood supply), and this causes pain.
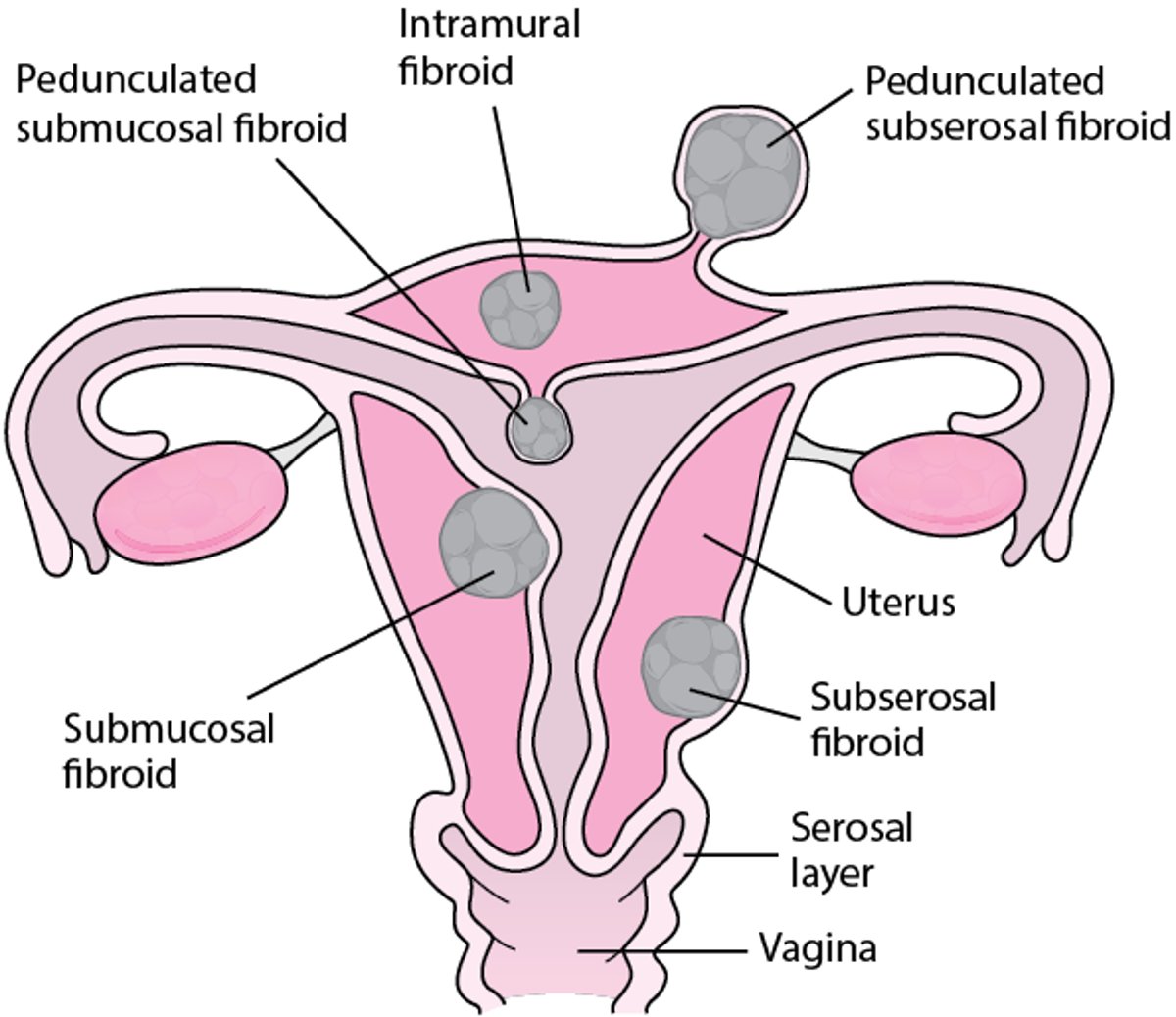
Fibroids may grow in different parts of the uterus, usually in the wall (which has three layers):
Under the outer surface of the uterus (subserosal fibroids)
In the wall of the uterus (intramural fibroids)
Under the inside layer (lining or endometrium) of the uterus (submucosal fibroids)
Sometimes fibroids grow in other locations, such as the cervix (bottom part of the uterus) or the broad ligament (connective tissue that surrounds the uterus).
Fibroids may be contained completely within the wall of the uterus, or they may protrude into other areas of the body. Fibroids can vary in shape. Some fibroids grow from a stalk (called pedunculated fibroids) and can protrude into the abdominal cavity, which can cause pressure on surrounding organs, such as the intestines or bladder. Some fibroids extend into the interior of the uterus (called intracavitary fibroids).
Some cancerous tumors of the uterus look similar to fibroids on imaging studies and may cause similar symptoms, such as abnormal bleeding. These cancerous tumors are rare, occurring in fewer than 1% of women with uterine masses that look similar to fibroids. Doctors do further evaluation if cancer is suspected. Based on current research, it is not thought that the typical type of fibroid changes and develops into cancer.
Where Uterine Fibroids Grow
Fibroids can grow in different parts of the uterus:
Some fibroids grow on a stalk and can protrude into the abdomen or the uterine cavity. They are called pedunculated fibroids. |

Symptoms of Fibroids
Symptoms depend on
Location in the uterus
Size
Number of fibroids
Most fibroids do not cause symptoms. The larger the fibroid, the more likely it is to cause symptoms.
A common symptom of fibroids is abnormal uterine bleeding. This can be heavy menstrual periods or periods that last longer than usual (more than 8 days in a cycle). Sometimes fibroids cause bleeding between periods. Bleeding may be severe and can result in anemia.
Fibroids in the wall of the uterus (intramural) may cause heavy bleeding by making it difficult for the uterus to contract. Contracting is how the uterus controls blood flow during a menstrual period or other episodes of uterine bleeding.
Fibroids located under the lining of the uterine cavity (submucosal) cause bleeding by changing the surface of the uterine cavity and the lining, which is shed during a menstrual period. Fibroids that protrude into the cavity of the uterus (intracavitary) cause the most change in the surface and usually cause more severe abnormal bleeding. Changes in the uterine cavity may also cause infertility by blocking the fallopian tubes or making it difficult for a pregnancy to implant, which can interfere with getting pregnant or increase the risk of miscarriage.
Large fibroids may cause pain, pressure, or a feeling of heaviness in the pelvic area during or between menstrual periods. This may be because the fibroids make the uterus larger overall, causing the abdomen to distend (stick out), or the uterus may press on surrounding organs, such as the intestines or bladder. Pedunculated fibroids that protrude into the abdomen can also press on surrounding organs and tissues and cause pressure or pain. Fibroids may press on the bladder, making a woman need to urinate more frequently or more urgently. Sometimes they press on other parts of the urinary tract and can block the flow of urine. They may press on the rectum, causing discomfort and constipation.
A fibroid growing on a stalk may twist, cutting off its blood supply, and cause severe pain.
Fibroids that are growing or degenerating can cause pressure or pain. Pain due to degenerating fibroids can last as long as they continue to degenerate.
Fibroids that cause no symptoms before pregnancy may cause problems during pregnancy. Problems include
Abnormal positioning (presentation) of the baby before delivery
Excessive blood loss after delivery (postpartum hemorrhage)
Diagnosis of Fibroids
Imaging, usually ultrasound
Doctors may suspect fibroids based on symptoms or results of a pelvic examination. However, imaging tests are often needed to confirm the diagnosis of uterine fibroids.
Imaging tests include
Transvaginal ultrasound: An ultrasound device is inserted into the vagina.
Saline infusion sonography (sonohysterography): If doctors suspect submucosal fibroids, they do ultrasound after infusing a small amount of fluid into the uterus to outline its interior.
Occasionally, those test results are unclear, and magnetic resonance imaging (MRI) is done.
If women have had abnormal bleeding, such as very heavy or prolonged menstrual periods or bleeding between periods, doctors may want to exclude cancer of the uterus. So they may do the following:
A biopsy of the uterine lining (endometrial biopsy)
Dilation and curettage (D & C), which is a procedure to take samples of the tissue in the uterine cavity, sometimes along with hysteroscopy)
For hysteroscopy, a viewing tube is inserted through the vagina and cervix into the uterus. A local, regional, or general anesthetic is often used for patients undergoing a D & C or hysteroscopy.
Treatment of Fibroids
Medications to relieve symptoms or shrink fibroids
Sometimes surgery to remove the entire uterus or only the fibroids
Sometimes procedures to destroy the fibroids
For most women who have small fibroids but no bothersome symptoms or other problems, treatment is not required. They are reexamined every 12 months so that doctors can determine whether symptoms are worsening or lessening and whether fibroids are growing.
Several treatment options, including medications and surgery, are available if bleeding or other symptoms worsen or if fibroids enlarge substantially.
Medications to treat fibroids
A few medications may be used to relieve symptoms or to shrink fibroids, but their effects are only temporary. No medication can treat fibroids so that they permanently resolve.
Medications used to treat fibroids may be hormonal or nonhormonal.
For control of abnormal uterine bleeding due to fibroids, oral hormonal or nonhormonal medications may be used. These medications do not decrease fibroid size, and thus do not treat bulk symptoms such as pelvic pain and pressure. The first medications given to decrease bleeding are easy to use and well-tolerated, including
Estrogen-progestin contraceptives
Progestins (for example, a levonorgestrel-releasing intrauterine device [IUD])
Tranexamic acid
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Progestins given alone without estrogen (such as medroxyprogesterone acetate or megestrol) can control bleeding in some women, but these medications do not shrink fibroids. They reduce bleeding by preventing the lining of the uterus from growing too much. When the uterine lining grows too much, there is more of it to break down and be shed during menstruation. As a result, menstrual bleeding may be heavier than usual. Progestins are taken by mouth. They may be taken every day or only for 10 to 14 consecutive days each menstrual cycle. Or doctors may give women injections of medroxyprogesterone acetate every 3 months or insert an intrauterine device (IUD) that releases a progestin called levonorgestrel.
For women who also desire contraception, estrogen-progestin contraceptives or a levonorgestrel IUD may be good options. However, these medications may have bothersome side effects, such as weight gain, depression, and irregular bleeding.
Tranexamic acid works by preventing blood clots (which are made by the body to help stop bleeding) from breaking down as quickly. As a result, bleeding decreases.
Nonsteroidal anti-inflammatory drugs (NSAIDs) may relieve pain and may slightly decrease bleeding.
Medications that may be used to reduce fibroid growth and treat abnormal uterine bleeding include
Gonadotropin-releasing hormone (GnRH) analogs
Selective estrogen receptor modulators (SERMs)
Danazol
Gonadotropin-releasing hormone (GnRH) analogs are used if other medications have not been effective, bleeding is persistent, and the woman has anemia (too few red blood cells in the blood). GnRH analogs are either agonists (such as leuprolide) or antagonists (such as elagolix and relugolix). Both types of analogs can shrink fibroids and reduce bleeding by creating a temporary state that is similar to menopause, which causes the body to produce less estrogen and progesterone. Because they shrink the fibroids and reduce bleeding, doctors may give GnRH analogs before surgery to make removal of fibroids easier, reduce blood loss, and thus reduce the risks of surgery.
The medications may be taken as a pill, injected, or implanted as a pellet under the skin. Nafarelin, another GnRH agonist, can be used as a nasal spray.
GnRH agonists are usually taken for less than 6 months. If taken for a long time, they may reduce bone density and increase the risk of osteoporosis. Low doses of estrogen, usually combined with a progestin (a medication that is similar to the hormone progesterone), may be given with GnRH agonists to help prevent loss of bone density.
Within 6 months after GnRH agonists are stopped, fibroids may become as large as they were before treatment.
Selective estrogen receptor modulators (SERMs), such as raloxifene and related medications, reverse some of estrogen’s effects. They may not be as effective as other medications.
Danazol (a synthetic hormone related to testosterone) can suppress fibroid growth but is rarely used because it has many side effects, such as weight gain, acne, increased body hair (hirsutism), swollen ankles, loss of scalp hair, vaginal dryness, and lowering of the voice.
Procedures to treat fibroids
Several minimally invasive procedures are available to treat fibroids. These are usually used if medications are not effective and a woman does not want surgery or has health reasons why she should not have surgery.
After having one of these procedures, women should not become pregnant. Whether pregnancy after these procedures is safe is unclear.
For uterine artery embolization, doctors use an anesthetic to numb a small area of the thigh and make a small puncture hole or incision there. Then, they insert a thin, flexible tube (catheter) through the incision into the main artery of the thigh (femoral artery). The catheter is threaded to the arteries that supply blood to the fibroid, and small synthetic particles are injected. The particles travel to the small arteries supplying the fibroid and block them. As a result, the fibroid dies, then shrinks. Most of the rest of the uterus appears to be unaffected. However, whether the fibroid will regrow (because blocked arteries reopen or new arteries form) is unknown.
After uterine artery embolization, most women have pain and cramping in the pelvis, nausea, vomiting, fever, fatigue, and muscle aches. These symptoms develop within 48 hours after the procedure and gradually lessen over 7 days. An infection may develop in the uterus or surrounding tissues. Women recover more quickly after this procedure than after a hysterectomy or myomectomy, but they tend to have more complications and more return visits to the doctor. If fibroids continue to be a problem or grow back after embolization, hysterectomy is recommended.
Magnetic resonance-guided focused ultrasound surgery uses sound waves to destroy fibroids.
Surgery for fibroids
Surgery is usually considered for women who have any of the following:
Fibroids that are rapidly enlarging
Bleeding that continues or recurs despite treatment with medications or minimally invasive procedures
Severe or persistent pain
Large fibroids that cause problems, such as the need to urinate frequently, constipation, pain during sexual intercourse, or blockage of the urinary tract
For women who want to conceive, fibroids that have caused infertility or repeated miscarriages
Several types of surgery can be done. The recommended surgery depends on the size, number, and location of fibroids. However, before making a decision about treatment, women should talk to their doctor about the problems that can result from each type of surgery and their desire for future pregnancy so that they can make an informed decision.
Surgery to remove fibroids traditionally involves one of the following:
Hysterectomy: The uterus is removed. Patients can discuss with their doctor whether to remove the cervix, ovaries, and fallopian tubes. Hysterectomy is the only permanent solution to fibroids. However, after hysterectomy, women cannot have children. Thus, hysterectomy is done only for women who do not wish to become pregnant.
Myomectomy: Only the fibroid or fibroids are removed. In contrast to a hysterectomy, most women who have a myomectomy can have children. However, after myomectomy, new fibroids may grow, and about 25% of women have a hysterectomy about 4 to 8 years later.
For hysterectomy, surgeons may use one of the following methods:
Laparoscopy: They make one or a few small incisions near or above the navel, then insert a viewing tube (laparoscope) and surgical instruments through the incisions.
Laparotomy: They make an incision that is several inches long in the abdomen.
Vaginal hysterectomy: The uterus is removed through the vagina, sometimes assisted by laparoscopy. An incision is made in the vagina. An abdominal incision is not needed.
Laparoscopic surgery can be done with robotic assistance. The robot is a device used to control and manipulate surgical instruments inserted with the laparoscope. The laparoscope sends a three-dimensional image of the body's interior to a console. Surgeons sit at a console to view this image, and a computer translates their hand movements into precise movements of the surgical instruments.
For myomectomy, surgeons may use
Hysteroscopy: Surgeons insert a telescope-like lighted device (hysteroscope) through the vagina into the uterus. Using instruments inserted through this tube, surgeons can cut tissue and remove fibroids on the inside of the uterus.
Laparoscopy
Laparotomy
Laparoscopy and hysteroscopy are outpatient procedures, and recovery is faster than recovery after laparotomy. However, sometimes removing fibroids using laparoscopy or hysteroscopy may be difficult or impossible—for example, when there are many fibroids, when they are very large, or when they are embedded deeply in the wall of the uterus. In such cases, doctors do a laparotomy.
Hysterectomy may be preferred to myomectomy or may be required for several reasons:
The woman does not desire future childbearing.
After myomectomy, fibroids may begin to grow again.
Women have disorders that make removal of fibroids harder. These disorders include endometriosis and abnormal bands of scar tissue in the uterus or pelvis (adhesions).
Hysterectomy may reduce the risks of developing new or worse disorders, especially if a woman has risk factors for a particular disorder. These disorders include endometriosis, cervical cancer, and endometrial cancer (cancer of the lining of the uterine cavity). For example, women who have Lynch syndrome are at increased risk of endometrial cancer.
Other treatments have been ineffective.
A procedure called morcellation may be done during myomectomy or hysterectomy. For this procedure, surgeons cut the fibroids or uterine tissue into small pieces so that the pieces can be removed through a smaller incision. Rarely, women with fibroids have cancer of the uterus that is unsuspected and undiagnosed. If morcellation is done in such women, the cancer cells may be spread into the abdomen and pelvis. In such cases, cancer can develop in other locations. Doctors can use surgical techniques to prevent tissue from being spread, such as using a bag to catch all of the pieces of the fibroid and remove them from the body. Before surgery for fibroids, women should evaluated for uterine cancer if they have any concerning symptoms and they should be informed of the very small risk of spreading cancerous cells if morcellation is done.
Radiofrequency fibroid ablation can be used during hysteroscopy or laparoscopy to destroy, rather than remove, fibroids. Doctors insert a needle that transmits an electrical current or heat into the fibroid to destroy its core. After these treatments, fibroids may grow back. In such cases, another treatment or a hysterectomy may be recommended.
Choice of treatment for fibroids
Choice of treatment for fibroids depends on the woman's situation, but women and their doctors may discuss the choice based on the following general guidelines:
If the fibroids do not cause any symptoms: No treatment but continue to follow up with a doctor.
If a woman is going through or has passed through menopause: Undergo evaluation for uterine cancer if there is abnormal uterine bleeding and, if results are normal, continue to follow up with a doctor to see if symptoms resolve, which usually happens as fibroids decrease in size after menopause.
If fibroids cause symptoms: Start with medications for most women, unless surgery is likely to be much more effective (such as for fibroids that are very large or for intracavitary submucosal fibroids). If medications are not effective, doctors treat with a minimally invasive procedure or surgery.
If fibroids cause infertility: Undergo myomectomy to remove fibroids.
If symptoms are severe and other treatments are ineffective, particularly if a woman does not want to become pregnant: Have a hysterectomy, possibly preceded by treatment with medications.
Drug Information for the Topic





