

Von Hippel-Lindau disease is a rare hereditary neurocutaneous disorder characterized by benign and malignant tumors in multiple organs. Diagnosis is made using clinical criteria and/or molecular genetic testing. Treatment is with surgery or sometimes radiation therapy or, for retinal angiomas, laser coagulation or cryotherapy.
Von Hippel-Lindau (VHL) is a neurocutaneous syndrome that occurs in 1 of 36,000 people and is inherited as an autosomal dominant trait with variable penetrance. The VHL gene is a tumor-suppressor gene located on the short arm of chromosome 3 (3p25.3). Over 1500 different mutations in this gene have been identified in patients with VHL. In 20% of affected people, the abnormal gene appears to be a new mutation.
VHL most commonly causes
Cerebellar hemangioblastomas
Retinal angiomas
Tumors, including pheochromocytomas and cysts (renal, hepatic, pancreatic, or genital tract), can occur in other organs. About 10% of people with VHL develop an endolymphatic tumor in the inner ear, threatening hearing. Risk of developing renal cell carcinoma increases with age and by age 60 may be as high as 70%.
Manifestations typically appear between ages 10 and 30 but can appear earlier.
Symptoms and Signs of VHL
Symptoms of VHL depend on the size and location of the tumors. Symptoms may include headaches, dizziness, weakness, ataxia, impaired vision, and high blood pressure.
Retinal angiomas, detected by direct ophthalmoscopy, appear as a dilated artery leading from the disk to a peripheral tumor with an engorged vein. These angiomas are usually asymptomatic, but if they are centrally located and enlarge, they can result in substantial loss of vision. These tumors increase risk of retinal detachment, macular edema, and glaucoma.
Untreated, VHL can result in blindness, brain damage, or death. Death usually results from complications of cerebellar hemangioblastomas or renal cell carcinoma.
Diagnosis of VHL
Direct ophthalmoscopy
Central nervous system imaging, typically MRI
Sometimes molecular genetic testing
Von Hippel-Lindau disease is diagnosed when one of the following criteria is met:
Family history of VHL and presence of ≥ 1 VHL tumor (retinal, brain, or spinal hemangioblastoma; pheochromocytoma; renal cell carcinoma; or pancreatic endocrine tumor)
Two or more characteristic VHL tumors in patients with no known family history of VHL

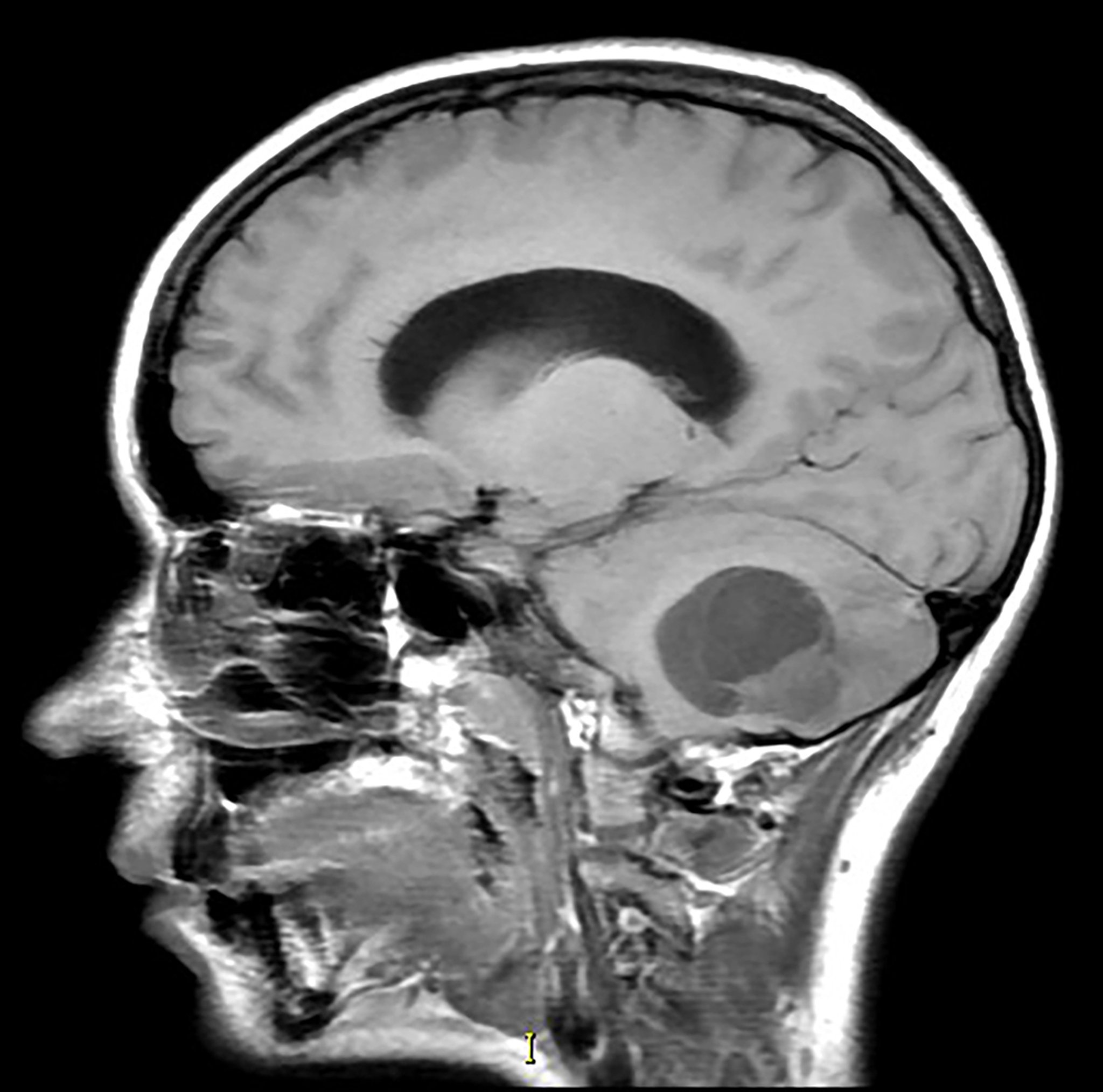
Living Art Enterprises/SCIENCE PHOTO LIBRARY
If clinical features are not conclusive, the diagnosis can also be established by using molecular genetic testing to identify a VHL gene mutation.
If a specific mutation for the VHL gene is identified in a patient, genetic testing should be done to determine whether at-risk family members also have that mutation.
Treatment of VHL
Surgery or sometimes radiation therapy
Belzutifan in selected patients with renal cell carcinomas, central nervous system hemangioblastomas, or pancreatic endocrine tumors
For retinal angiomas, laser coagulation or cryotherapy
Regular monitoring
Treatment of von Hippel-Lindau often involves surgical removal of the tumor before it becomes harmful. Pheochromocytomas are surgically removed; sometimes continued treatment of hypertension is needed. Renal cell carcinomas are surgically removed; advanced cancers may respond to pharmacologic treatment. Some tumors can be treated with focused high-dose radiation.
Belzutifan, an oral hypoxia-inducible factor-2 alpha inhibitor, is available for use in adult patients with VHL renal cell carcinomas, central nervous system hemangioblastomas, or pancreatic endocrine tumors that do not require immediate surgical removal. This medication can be used until the disease progresses or unacceptable toxicity occurs.Belzutifan, an oral hypoxia-inducible factor-2 alpha inhibitor, is available for use in adult patients with VHL renal cell carcinomas, central nervous system hemangioblastomas, or pancreatic endocrine tumors that do not require immediate surgical removal. This medication can be used until the disease progresses or unacceptable toxicity occurs.
Typically, retinal angiomas are treated with laser coagulation or cryotherapy to preserve vision.
Use of propranolol to reduce the size of the hemangiomas is being studied.Use of propranolol to reduce the size of the hemangiomas is being studied.
Screening to check for complications and early treatment can improve prognosis.
Screening for complications
If the diagnostic criteria for VHL are met, patients should be regularly screened to check for complications of VHL because early detection is key to preventing serious complications.
Routine surveillance should include the following (1):
Annual history and physical examination
Annual dilated eye examination beginning in infancy to screen for retinal hemangioblastomas
Annual blood pressure monitoring beginning at 2 years of age to screen for pheochromocytomas
Annual measurement of urine or plasma fractionated metanephrines beginning at 5 years of age to screen for pheochromocytomas
Brain and spinal MRI every 2 years beginning at 11 years of age to screen for central nervous system hemangioblastomas
Audiography every 2 years beginning at 11 years of age to screen for endolymphatic sac tumors
Abdominal MRI or ultrasonography every 2 years beginning at 15 years of age to screen for renal cell carcinomas, pheochromocytomas, and pancreatic tumors
People who do not meet diagnostic criteria for VHL but who have a germline mutation or who have not been tested but are first- and second-degree family members of a patient with VHL also should be screened using the following:
Annual evaluation for neurologic symptoms and for vision and hearing problems
Annual ocular examination to look for nystagmus, strabismus, and white pupils
Annual blood pressure monitoring
Screening reference
1. Maher ER: Von Hippel-Lindau disease. Curr Mol Med 4(8):833–842, 2004. doi: 10.2174/1566524043359827
Key Points
Von Hippel-Lindau (VHL) disease is a rare hereditary neurocutaneous disorder characterized by benign and malignant tumors in multiple organs.
Most commonly, VHL causes cerebellar hemangioblastomas and retinal angiomas.
Diagnosis is confirmed if the patient has a family history of VHL and presence of ≥ 1 VHL tumor or has ≥ 2 characteristic VHL tumors with no known family history of VHL.
Molecular genetic testing is also available for difficult to diagnose cases.
Treat with surgical removal of tumors and laser coagulation or cryotherapy for retinal angiomas.
Consider belzutifan in selected patients with renal cell carcinomas, central nervous system hemangioblastomas, or pancreatic endocrine tumors.Consider belzutifan in selected patients with renal cell carcinomas, central nervous system hemangioblastomas, or pancreatic endocrine tumors.
Regularly screen for complications, which can guide early treatment and improve prognosis.
Drugs Mentioned In This Article





