




Malocclusion is abnormal contact between the maxillary and mandibular teeth.
(See also Evaluation of the Dental Patient.)


DR ARMEN TARANYAN/SCIENCE PHOTO LIBRARY
Normally, each dental arch consists of teeth in side-by-side contact, forming a smooth curve, with the maxillary anterior teeth overlying the upper third of the mandibular anterior teeth (see figure Identifying the Teeth). The buccal (outer) cusps of the maxillary posterior teeth are external to the corresponding cusps of the mandibular posterior teeth. In most cases, the anterior buccal cusp of the maxillary first permanent molar fits into the anterior buccal groove of the mandibular first molar.
Because the outer parts of all maxillary teeth are normally external to the mandibular teeth, the lips and cheeks are displaced from between the teeth so that they are not bitten. The lingual (inner) surfaces of the lower teeth form a smaller arch than those of the upper teeth, confining the tongue and minimizing the likelihood of its being bitten. All the maxillary teeth should contact the corresponding mandibular teeth, so that the masticatory forces (which may be > 150 pounds [> 1000 kilopascals] in the molar region and 250 pounds [> 1700 kilopascals] when clenching during sleep) are widely distributed. If these forces are applied to only a few teeth, those teeth may eventually become mobile or show abnormal wear.
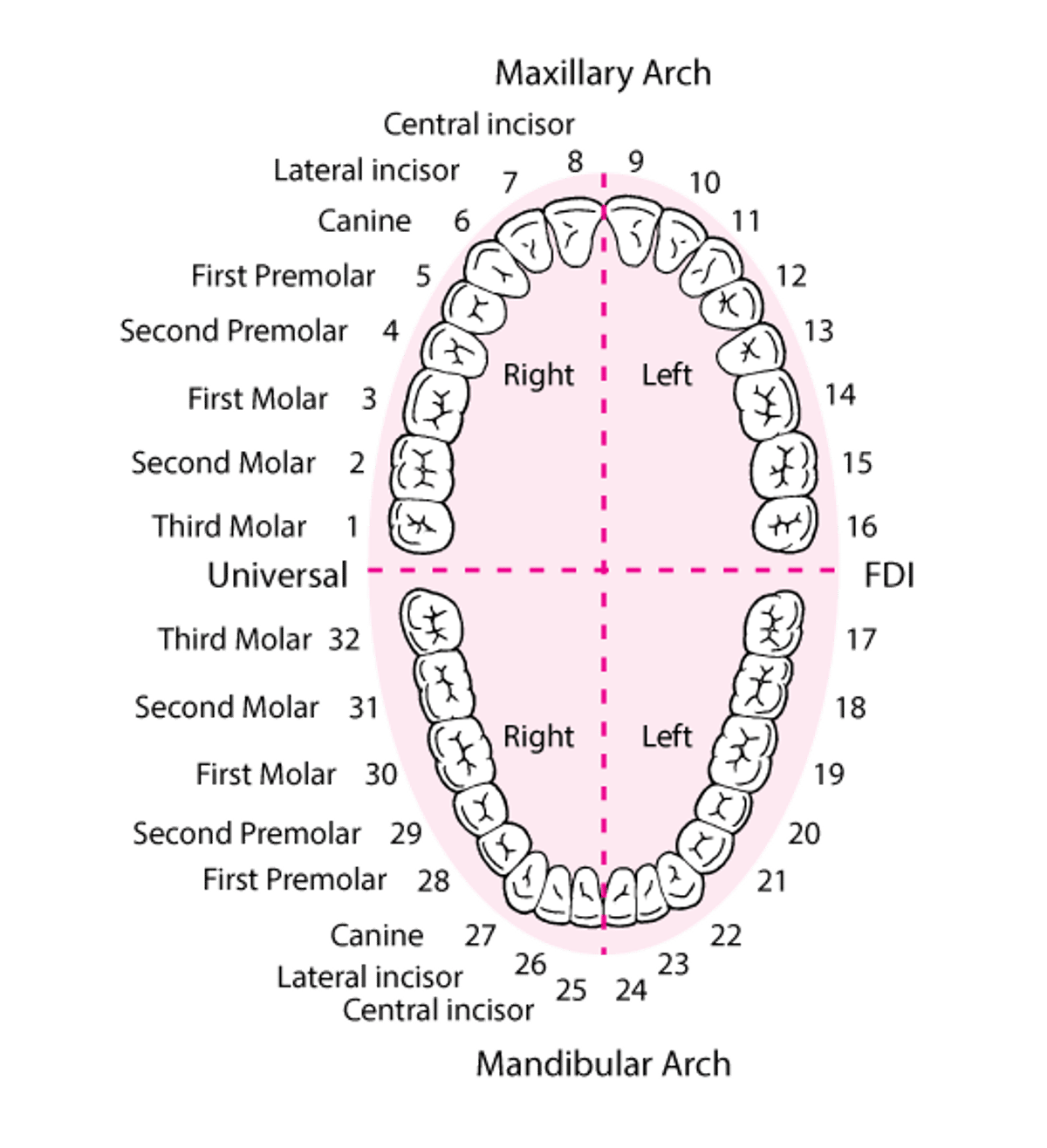
Identifying the Teeth
The numbering system shown is the one most commonly used in the United States. |

Etiology of Malocclusion
Causes of malocclusion include
Size mismatch between jaw and teeth
Certain oral habits (eg, thumb-sucking, tongue thrusting)
Missing teeth
Facial trauma
Certain congenital defects
Malocclusion most often results from jaw and tooth size discrepancies (ie, the jaw is too small or the teeth are too large for the jaw to accommodate them in proper alignment). People who habitually suck their thumb or push their tongue up against their front teeth may cause gradual protrusion of the upper incisors.
When permanent teeth are lost, adjacent teeth may shift and opposing teeth may extrude, causing malocclusion unless a bridge, implant, or partial denture (see Dental Appliances) is worn to prevent these movements. When children lose deciduous teeth prematurely, the teeth more posterior in the arch or the permanent first molars often drift forward, leaving insufficient space for other permanent teeth to erupt.
Malocclusion after facial trauma may indicate tooth displacement and/or alveolar bone or jaw fractures. In ectodermal dysplasia, cleft palate, or Down syndrome, malocclusions may result from having too few teeth.
Evaluation of Malocclusion
Physical examination
Occlusion is checked on both sides of the mouth by retracting each cheek with a tongue depressor while telling the patient to close on the back teeth; telling patients to bite may mistakenly cause them to close on their incisors (as in biting a piece of fruit), which gives the false appearance of malocclusion of the back teeth. Malocclusion sometimes is identified as early as the first dental visit (age 1 year). Early identification may make later treatment easier and more effective.
Treatment of Malocclusion
Dental modification
Orthodontic appliances (braces or aligners)
Sometimes surgery
Malocclusions are corrected primarily for aesthetic and psychological reasons. However, in some cases, treatment may increase resistance to caries (by improving ability to clean realigned teeth), to anterior tooth fracture, and, possibly, to periodontal disease or stripping of the gingiva on the palate. Treatment may improve speech and mastication as well. Occlusion can be improved by aligning teeth properly, by selectively grinding teeth and restorations that contact prematurely, and by inserting crowns or onlays to build up tooth surfaces that are below the plane of occlusion.
Braces (metal orthodontic appliances) apply a continuous mild force to teeth to gradually remodel the surrounding alveolar bone. Extraction of one or more permanent teeth (usually a first premolar) may be needed to allow other teeth to be repositioned or to erupt into a stable alignment. After the teeth are properly aligned, the patient wears either a fixed retainer (wire bonded to the back of the teeth) or a removable retainer. Removable retainers are made from plastic-and-wire or vacuum-formed plastic and are worn 24 hours a day initially, then only at night for 2 to 3 years.
Tooth aligners are a set of clear plastic appliances (similar to retainers) that are used in a specific order to gradually move teeth (up to 0.3 mm per aligner). Each aligner is worn for about 2 weeks and then changed for a new one until the misalignment is corrected. As with traditional braces, a retainer is used to keep the teeth from shifting back.
When orthodontic treatment alone is insufficient, surgical correction of jaw abnormalities contributing to malocclusion (orthognathic surgery) may be indicated.






