




Many people with diabetes require medication to lower blood glucose levels, relieve symptoms, and prevent complications of diabetes.
There are two types of diabetes mellitus
Type 1, in which the body's immune system attacks the insulin-producing cells of the pancreas, and more than 90% of them are permanently destroyed
Type 2, in which the body develops resistance to the effects of insulin
General treatment of type 1 diabetes requires lifestyle changes, including a healthy diet and exercise. People with type 1 diabetes require insulin injections and frequent monitoring of glucose levels.
General treatment of type 2 diabetes also requires lifestyle changes, including weight loss, a healthy diet, and exercise. A few people with type 2 diabetes can control blood glucose levels with only diet and exercise, but most people require medication to lower blood glucose levels, sometimes including insulin. People who take medication for type 2 diabetes also often need to monitor blood glucose daily to several times a day.
Doctors must be careful when treating diabetes with medication because insulin and some of the medications given by mouth can make blood glucose levels too low (hypoglycemia).
Insulin Replacement Therapy
People with type 1 diabetes almost always require insulin therapy and will become very sick without it. Many people with type 2 diabetes require insulin as well. Usually, insulin is injected under the skin. For certain people, inhaled insulin is also available, although it is not used commonly. Insulin cannot be taken by mouth because insulin is destroyed in the stomach. Newer forms of insulin, such as forms that can be taken by mouth, are being tested.
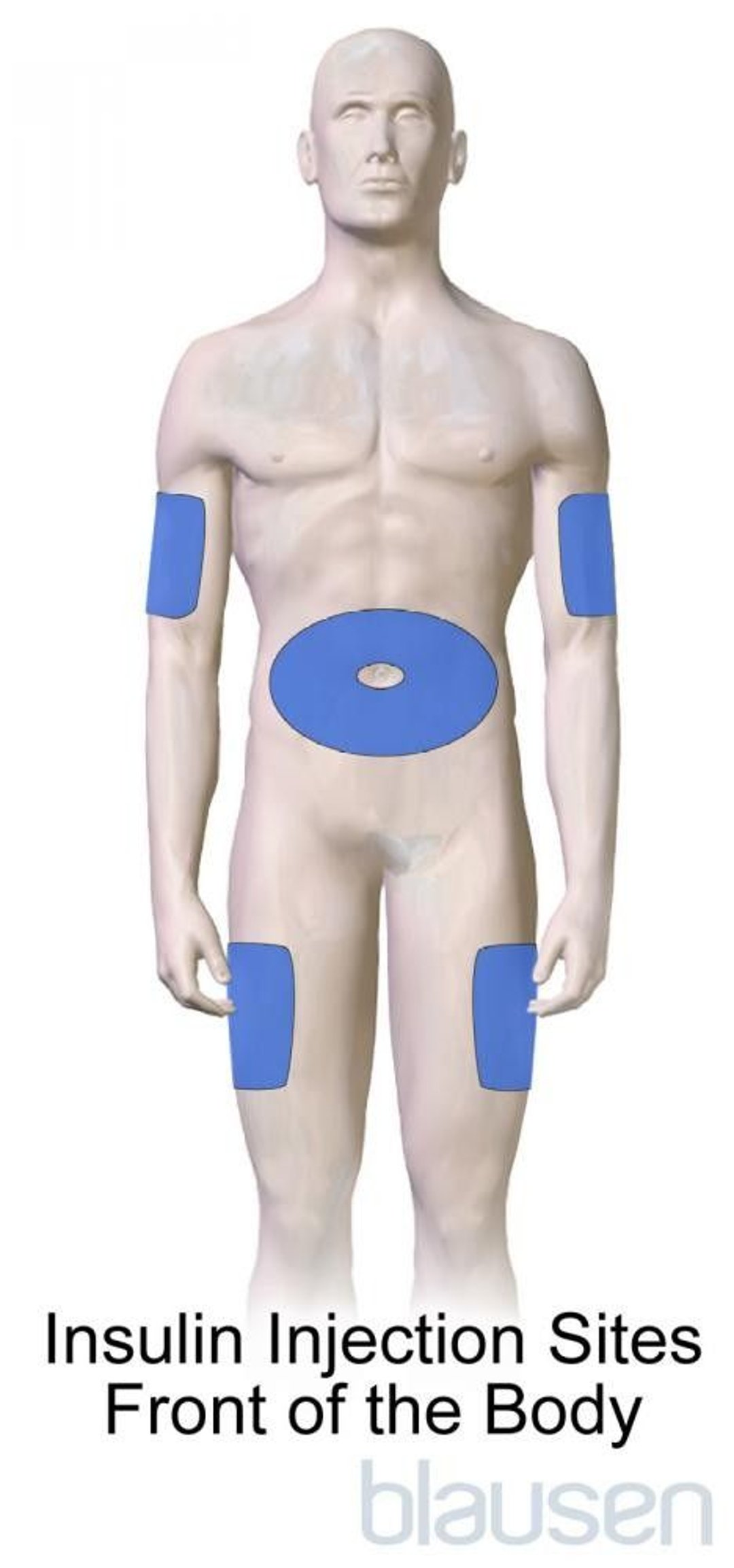
Insulin is injected under the skin into the fat layer, usually in the arm, thigh, or abdomen. Small syringes with very thin needles make the injections nearly painless.


An insulin pen, which contains a cartridge that holds the insulin, is a convenient way for many people to carry and use insulin, especially for people who take several injections a day outside the home.
Another device is an insulin pump, which pumps insulin continuously from a reservoir through a small cannula (hollow plastic tube) left in the skin. The rate of insulin administration can be adjusted depending on the time of day, whether the person is exercising, or other parameters. People can release additional doses of insulin as needed for meals or to correct high blood glucose levels. The pump mimics the way the body normally produces insulin. Pump therapy is considered in some people who require more than three injections per day. For some people, the pump offers an added degree of control, whereas others find wearing the pump inconvenient or develop sores at the cannula insertion site.
Hybrid closed-loop insulin-delivery systems are also available. With these systems (sometimes called an artificial pancreas), an algorithm is used to calculate and automatically deliver baseline insulin doses through an insulin pump based on input from a continuous glucose monitor. However, this device does not eliminate the need for people to monitor their blood glucose levels and give themselves insulin before meals.
Insulin forms
Insulin is available in four basic forms, divided by speed of onset and duration of action:
includes lispro, aspart, and glulisine insulins. They are the fastest of all, reaching maximum activity in about 1 hour and working for 3 to 5 hours. Rapid-acting insulins are injected at the beginning of a meal or up to 15 minutes beforehand.
such as regular insulin, begins acting slightly more slowly and lasts longer than rapid-acting insulin. Regular insulin reaches its maximum activity in 2 to 4 hours and works for 6 to 8 hours. It is injected 30 minutes before eating a meal.
such as insulin isophane (sometimes known as neutral protamine Hagedorn or NPH) or U-500 insulin, starts to work within 0.5 to 2 hours, reaches its maximum activity in 4 to 12 hours, and works for 13 to 26 hours depending on which intermediate-acting insulin is used. This type of insulin may be used in the morning to provide coverage for the first part of the day or in the evening to provide coverage during the night.
such as insulin glargine, insulin detemir, U-300 insulin glargine or insulin degludec, has very little effect during the first few hours but provides coverage for 20 to 40 hours depending on which of these types is used.
Both rapid-acting insulin and short-acting insulin are often used by people who take several daily injections and need extra insulin for meals.
Some combinations of insulin are available already mixed. In addition, concentrated insulins are available for people who require high doses of insulin.
Inhaled insulin is available for use in some situations for people who are unable or unwilling to take insulin injections. Inhaled insulin is available as an inhaler (similar to an asthma inhaler), and people inhale the insulin into the lungs for absorption. Inhaled insulin works similar to rapid-acting insulin and needs to be taken several times per day. People also need to take injections of long-acting insulin. While people are using inhaled insulin, doctors check their lung function every 6 to 12 months.
Insulin preparations are stable at room temperature for up to 1 month, allowing them to be carried, brought to work, or taken on a trip. Insulin should not, however, be exposed to extreme temperatures and should be refrigerated if being stored for longer than 1 month.
Choice of insulin type and dose
The choice of insulin is complex. Doctors consider the following factors when deciding which insulin is best and how much insulin to use:
How well the body responds to the insulin it makes
How much the blood glucose level rises after meals
Whether other antihyperglycemic medications can be used instead of insulin
How willing and able people are to monitor their blood glucose levels and adjust their insulin dosage
How often people are willing to inject insulin
How varied daily activity is
How likely a person is to have symptoms of hypoglycemia (low blood glucose levels)
Doctors sometimes have people combine two insulins—a rapid-acting and an intermediate-acting insulin—in one morning dose. A second injection of one insulin or both may be taken at dinner or at bedtime.
Some people take the same amount of insulin every day. Other people, especially people with type 1 diabetes, need to adjust the insulin dose, especially doses taken around mealtime, depending on their diet, exercise, and blood glucose patterns. In addition, insulin needs may change if people gain or lose weight or experience emotional stress or illness, especially infection.
One adjustable regimen involves injecting a long-acting insulin in the morning or evening along with several additional injections of rapid-acting insulin during the day with meals. Adjustments are made as insulin needs change. Measuring blood glucose levels at various times during the day helps determine the adjustment. This regimen requires people to have a lot of knowledge about diabetes to pay close attention to the details of their treatment.
Hypoglycemia
The most common complication of insulin treatment is low blood glucose levels (hypoglycemia). Hypoglycemia occurs more often in people who try to strictly control blood glucose levels.
Symptoms of mild or moderate hypoglycemia include headache, sweating, palpitations, light-headedness, blurred vision, agitation, and confusion. Symptoms of more severe hypoglycemia include seizures and loss of consciousness. In older adults, hypoglycemia may cause stroke-like symptoms.
People who have frequent hypoglycemia may be unaware of hypoglycemic episodes because they no longer experience symptoms (hypoglycemia unawareness).
Doctors teach people how to recognize symptoms of hypoglycemia and how to treat these symptoms. Usually, a person can eat something sweet such as candy or juice to raise their blood glucose level quickly. People may also carry glucose tablets to take in the event of hypoglycemia. Because people with hypoglycemia may be too confused to recognize they are hypoglycemic, it is important for other members of their household and trusted others to be familiar with signs of hypoglycemia.
Insulin antibodies
In very rare cases, the body produces antibodies to injected insulin because injected insulin is not exactly like the insulin the body manufactures. These antibodies may interfere with insulin’s activity, requiring very large doses.
Allergic reaction to insulin
Insulin injections can affect the skin and underlying tissues. An allergic reaction, which occurs rarely, causes pain and burning, followed by redness, itchiness, and swelling around the injection site for several hours. Very rarely, a person may have an anaphylactic reaction after injection of insulin.
Skin reactions to insulin
Insulin injections may cause fat deposits, making the skin look lumpy, or destroy fat, causing indentation of the skin. Although this skin reaction is not an allergic reaction, it can decrease the absorption of injected insulin. It is, therefore, important to rotate the injection sites, for example, using the thigh one day, the stomach another, and an arm the next, to avoid these problems.


Oral Antihyperglycemic Medications
Oral antihyperglycemic medication can often lower blood glucose levels adequately in people with type 2 diabetes. However, they are not effective in type 1 diabetes. There are several types, but oral antihyperglycemic medications work in four major ways:
Insulin secretagogues stimulate the pancreas to produce more insulin
Insulin sensitizers do not affect the release of insulin but rather increase the body’s response to it
Some medications delay absorption of glucose by the intestine
Some medications increase glucose excretion in the urine
Insulin secretagogues
Insulin sensitizers
Medications that delay absorption of glucose by the intestine
Medications that increase glucose secretion in the urine
Dipeptidyl peptidase-4 (DPP 4) inhibitorsinsulin and delay the absorption of glucose by the intestine. These medications work by increasing glucagon-like peptide 1 (GLP-1).
insulin, an injectable glucagon-like peptide 1 (GLP-1) medication, or a combination medication containing GLP-1 and glucose-dependent insulinotropic polypeptide (GIP), may be used if one medication is not adequate. The treatment of diabetes often requires medication adjustments and addition of medications over time.
Injectable Antihyperglycemic Medications
is the most commonly used injectable antihyperglycemic medication. Its use is discussed above.
There are 3 other types of injectable antihyperglycemic medications:
Glucagon-like peptide 1 (GLP-1) medications
Combination medication containing GLP-1 and glucose-dependent insulinotropic polypeptide (GIP)
Amylin-like medications
Injectable antihyperglycemic medications are given together with other antihyperglycemic medications.
Glucagon-like peptide medications (GLP-1 medications) work mainly by increasing insulin secretion by the pancreas. These medications also slow the passage of food out of the stomach (which slows the rise of blood glucose), and reduce appetite and promote weight loss. GLP-1 medications are given by injection. The most common side effects are nausea and vomiting. These medications may increase the risk of pancreatitis (a painful inflammation of the pancreas), although the evidence is unclear. They should not be used in people with a personal or family history of medullary thyroid cancer, because studies in animals showed an increased risk of some types of thyroid tumors. So far, data from large clinical trials has not shown an increase in these types of cancers in humans.
insulin secretion and weight loss. This medication can also be used in people who have type 2 diabetes and obesity.
Amylin-like medicationsamylin-like medication. It suppresses secretion of the hormone glucagon. Because glucagoninsulin in people with type 1 or type 2 diabetes.
Disease-Modifying Medication
A monoclonal antibody
Other Medications Given to People With Diabetes
Because people with diabetes mellitus are at risk of complications, such as heart attacks and strokes, it is important that people take medications to prevent or treat these complications. Unless there is a reason people cannot take one of these medications (for example, an allergy to the medication), they may be given the following:
Angiotensin converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs): For people with diabetes and high blood pressure or chronic kidney disease
Aspirin: For people with diabetes and risk factors for cardiovascular disease
Statins: For people 40 to 75 years-old with diabetes to decrease the risk of cardiovascular disease
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of the resources.
American Diabetes Association: Comprehensive information on diabetes, including resources for living with diabetes
JDRF (previously called Juvenile Diabetes Research Foundation): General information on type 1 diabetes mellitus
National Institute of Diabetes and Digestive and Kidney Diseases: General information on diabetes, including on the latest research and community outreach program






