




Vitamin A is required for the formation of rhodopsin, a photoreceptor pigment in the retina (see table Sources, Functions, and Effects of Vitamins). Vitamin A helps maintain epithelial tissues and is important for lysosome stability and glycoprotein synthesis.
vitamin A. Carotenoids are absorbed better from vegetables when they are cooked or homogenized and served with some fat (eg, oils). Normally, the liver stores 80 to 90% of the body’s vitamin A. To use vitamin A, the body releases it into the circulation bound to prealbumin (transthyretin) and retinol-binding protein.
Retinol activity equivalents (RAE) were developed because provitamin A carotenoids have less vitamin A activity than preformed vitamin A; 1 mcg retinol = 3.33 units.
Synthetic vitamin analogs (retinoids) are being used increasingly in dermatology. The possible protective role of beta-carotene and retinoids against some epithelial cancers is under study. However, risk of certain cancers may be increased after beta-carotene supplementation.
(See also Overview of Vitamins.)
Primary vitamin A deficiency is usually caused by
Prolonged dietary deprivation
It is endemic in areas such as southern and eastern Asia, where rice, devoid of beta-carotene, is the staple food. Xerophthalmia due to primary deficiency is a common cause of blindness among young children in countries with high rates of food insecurity.
Secondary vitamin A deficiency may be due to
Decreased bioavailability of provitamin A carotenoids
Interference with absorption or storage is likely in celiac disease, cystic fibrosis, pancreatic insufficiency, duodenal bypass, chronic diarrhea, bile duct obstruction, giardiasis, and cirrhosis. Vitamin A deficiency is common in prolonged protein-energy undernutrition not only because the diet is deficient but also because vitamin A storage and transport is defective.

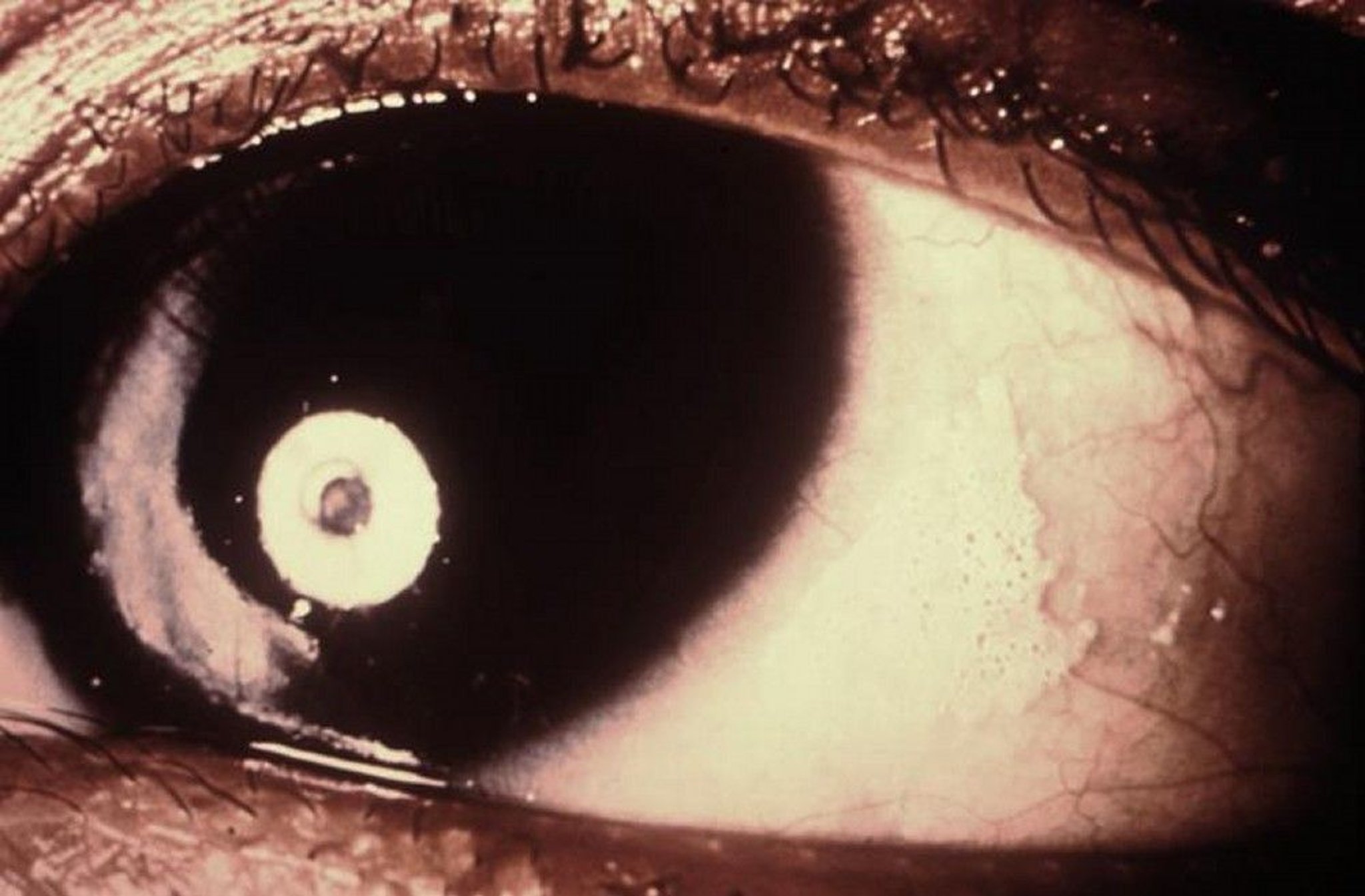
Image courtesy of the Nutrition Program via the Public Health Image Library of the Centers for Disease Control and Prevention.
Impaired dark adaptation of the eyes, which can lead to night blindness, is an early symptom of vitamin A deficiency. Xerophthalmia (which is nearly pathognomonic) results from keratinization of the eyes. It involves drying (xerosis) and thickening of the conjunctivae and corneas. Superficial foamy patches composed of epithelial debris and secretions on the exposed bulbar conjunctiva (Bitot spots) develop. In advanced deficiency, the cornea becomes hazy and can develop erosions, which can lead to its destruction (keratomalacia).
Keratinization of the skin and of the mucous membranes in the respiratory, gastrointestinal, and urinary tracts can occur. Drying, scaling, and follicular thickening of the skin and respiratory infections can result.
Immunity is generally impaired.
The younger the patient, the more severe are the effects of vitamin A
Ocular findings suggest vitamin A deficiency. Dark adaptation can be impaired in other disorders (eg, zinc deficiency, retinitis pigmentosa, severe refractive errors, cataracts, diabetic retinopathy). If dark adaptation is impaired, rod scotometry and electroretinography are done to determine whether vitamin A deficiency is the cause.
Serum levels of retinol are measured. Normal range is 28 to 86 mcg/dL (1 to 3 mcmol/L). However, levels decrease only after the deficiency is advanced because the liver contains large stores of vitamin A. Also, decreased levels may result from acute infection, which causes retinol-binding protein and transthyretin (also called prealbumin) levels to decrease transiently.
< 6 months can be given a one-time dose of 50,000 units (15,000 RAE), and those aged 6 to 12 months can be given a one-time dose of 100,000 units (30,000 RAE).
Dietary deficiency of vitamin A< 6 months, 100,000 units for infants 6 to 12 months, or 200,000 units for children > 12 months and adults should be given for 2 days, with a third dose at least 2 weeks later. The same doses are recommended for infants and children with complicated measles.
measlesWHO: Measles Fact Sheet).
Infants born of HIV-positive mothers should receive 50,000 units (15,000 RAE) within 48 hours of birth. Prolonged daily administration of large doses, especially to infants, must be avoided because toxicity may result.
For pregnant or breastfeeding women, prophylactic or therapeutic doses should not exceed 10,000 units (3000 RAE)/day to avoid possible damage to the fetus or infant.
Key Points
Vitamin A deficiency usually results from dietary deficiency, as occurs in areas where rice, devoid of beta-carotene, is the staple food, but it may result from disorders that interfere with the absorption, storage, or transport of vitamin A.
Ocular findings include impaired night vision (early), conjunctival deposits, and keratomalacia.
In children with severe deficiency, growth is slowed and risk of infection is increased.
Diagnose based on ocular findings and serum retinol levels.






