


An ischemic stroke is death of an area of brain tissue (cerebral infarction) resulting from an inadequate supply of blood and oxygen to the brain due to blockage of an artery.
Ischemic stroke usually results when an artery to the brain is blocked, often by a blood clot and/or a fatty deposit due to atherosclerosis.
Symptoms occur suddenly and may include muscle weakness, paralysis, lost or abnormal sensation on one side of the body, difficulty speaking, confusion, problems with vision, dizziness, and loss of balance and coordination.
Diagnosis is usually based on symptoms and results of a physical examination and brain imaging.
Other imaging tests (computed tomography and magnetic resonance imaging) and blood tests are done to identify the cause of the stroke.
Treatment may include medications to break up blood clots or to make blood less likely to clot and procedures to physically remove blood clots, followed by rehabilitation.
About one third of people recover all or most of normal function after an ischemic stroke.
Preventive measures include control of risk factors, medications to make blood less likely to clot, and sometimes surgery or angioplasty to open blocked arteries.
(See also Overview of Stroke.)
Causes of Ischemic Stroke
An ischemic stroke typically results from blockage of an artery that supplies blood to the brain, most commonly a branch of one of the internal carotid arteries. As a result, brain cells are deprived of blood. Most brain cells die if they are deprived of blood for 4.5 hours.
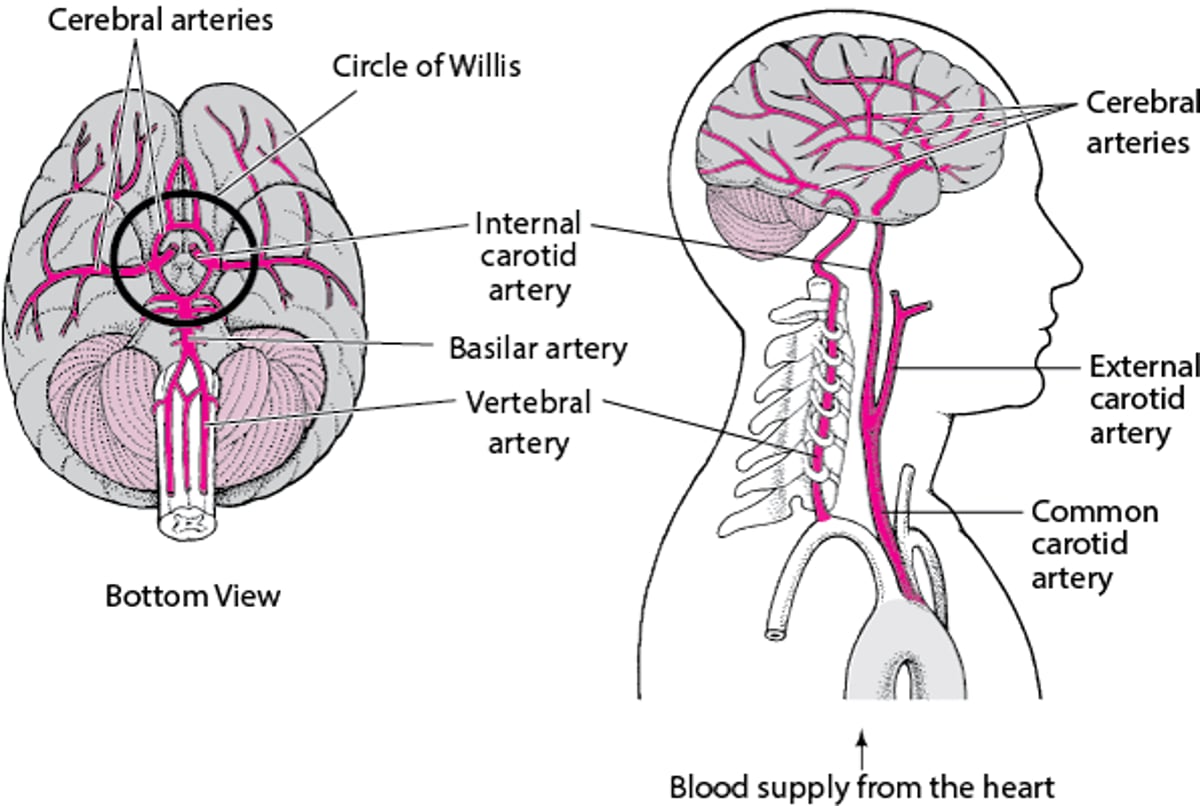
Supplying the Brain With Blood
Blood is supplied to the brain through two pairs of large arteries:
In the skull, the vertebral arteries unite to form the basilar artery (at the back of the head). The internal carotid arteries and the basilar artery divide into several branches, including the cerebral arteries. Some branches join to form a circle of arteries (circle of Willis) that connect the vertebral and internal carotid arteries. Other arteries branch off from the circle of Willis like roads from a traffic circle. The branches carry blood to all parts of the brain. When the large arteries that supply the brain are blocked, some people have no symptoms or have only a small stroke. But others with the same sort of blockage have a massive ischemic stroke. Why? Part of the explanation is collateral arteries. Collateral arteries run between other arteries, providing extra connections. These arteries include the circle of Willis and connections between the arteries that branch off from the circle. Some people are born with large collateral arteries, which can protect them from strokes. Then when one artery is blocked, blood flow continues through a collateral artery, sometimes preventing a stroke. Other people are born with small collateral arteries. Small collateral arteries may be unable to pass enough blood to the affected area, so a stroke results. The body can also protect itself against strokes by growing new arteries. When blockages develop slowly and gradually (as occurs in atherosclerosis), new arteries may grow in time to keep the affected area of the brain supplied with blood and thus prevent a stroke. If a stroke has already occurred, growing new arteries can help prevent a second stroke (but cannot reverse damage that has been done). |

Common causes
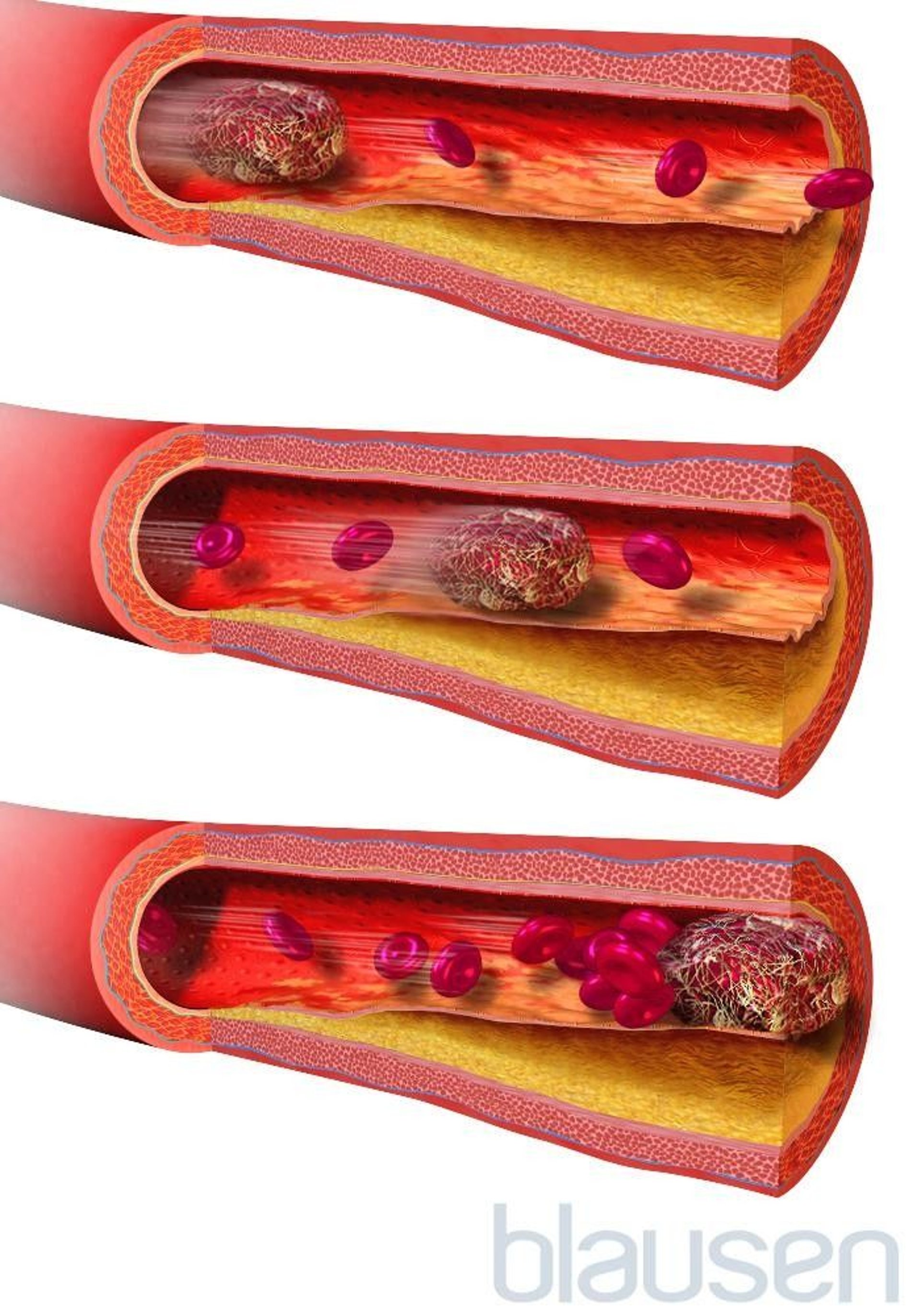
Commonly, blockages are blood clots (thrombi) or pieces of fatty deposits (atheromas, or plaques) due to atherosclerosis. Such blockages often occur in the following ways:
By forming in and blocking an artery: An atheroma in the wall of an artery may continue to accumulate fatty material and become large enough to block the artery. Even if the artery is not completely blocked, the atheroma narrows the artery and slows blood flow through it, like a clogged pipe slows the flow of water. Slow-moving blood is more likely to clot. A large clot can block enough blood flowing through the narrowed artery that brain cells supplied by that artery die. Or if an atheroma splits open (ruptures), the material in it can trigger formation of a blood clot that can block the artery (see figure How Atherosclerosis Develops).
By traveling from another artery to an artery in the brain: A piece of an atheroma or a blood clot in the wall of an artery can break off and travel through the bloodstream (becoming an embolus). The embolus may then lodge in an artery that supplies the brain and block blood flow there. (Embolism refers to blockage of arteries by materials that travel through the bloodstream to another part of the body.) Such blockages are more likely to occur where arteries are already narrowed by fatty deposits.
By traveling from the heart to the brain: Blood clots may form in the heart or on a heart valve, particularly artificial valves and valves that have been damaged by infection of the heart's lining (endocarditis). These clots may break off and travel as emboli and block an artery to the brain. Strokes due to such blood clots are most common among people who have recently had heart surgery, who have had a heart attack, or who have a heart valve disorder or an abnormal heart rhythm (arrhythmia), especially a fast, irregular heart rhythm called atrial fibrillation.
Clogs and Clots: Causes of Ischemic Stroke
When an artery that carries blood to the brain becomes clogged or blocked, an ischemic stroke can occur. Arteries may be blocked by fatty deposits (atheromas, or plaques) due to atherosclerosis. Arteries in the neck, particularly the internal carotid arteries, are a common site for atheromas. Arteries may also be blocked by a blood clot (thrombus). Blood clots may form on an atheroma in an artery. Clots may also form in the heart of people with a heart disorder. Part of a clot may break off and travel through the bloodstream (becoming an embolus). It may then block an artery that supplies blood to the brain, such as one of the cerebral arteries. |

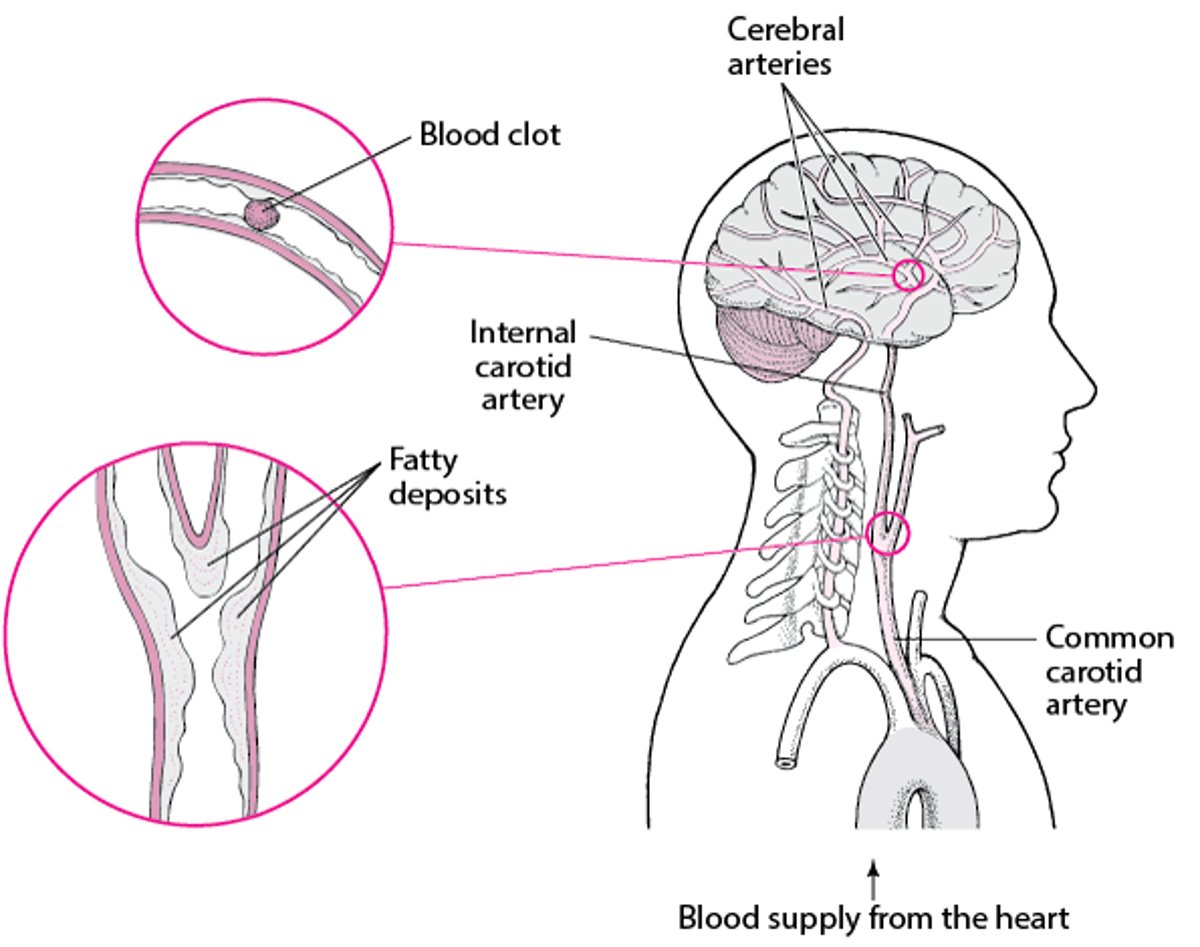

Blood clots in a brain artery do not always cause a stroke. If the clot breaks up spontaneously within less than 15 to 30 minutes, brain cells do not die and people's symptoms resolve. Such events are called transient ischemic attacks (TIAs).
If an artery narrows very gradually, other arteries (called collateral arteries—see figure Supplying the Brain With Blood) sometimes enlarge to supply blood to the parts of the brain normally supplied by the clogged artery. Thus, if a clot occurs in an artery that has developed collateral arteries, people may not have symptoms.
The most common causes of ischemic stroke can be classified as
Cryptogenic stroke
Embolic stroke
Lacunar infarction
Large-vessel atherosclerosis (the 4th most common cause)
Cryptogenic stroke
Stroke is classified as cryptogenic when no clear cause is identified despite a complete evaluation.
Embolic stroke
Blood clots can form in the heart, especially in people who have or have had the following:
Rheumatic heart disease (usually mitral stenosis)
Mechanical circulatory assist devices (such as a left ventricular assist device)
Tiny pieces of these blood clots can break off and travel to small arteries in the brain (as emboli).
Lacunar infarction
Lacunar infarction refers to tiny ischemic strokes, typically no larger than about a third of an inch (1 centimeter). In lacunar infarction, one of the small arteries deep in the brain becomes blocked when part of its wall deteriorates and is replaced by a mixture of fat and connective tissue—a disorder called lipohyalinosis. Lipohyalinosis is different from atherosclerosis, but both disorders can cause arteries to be blocked.
Lacunar infarction can also occur when tiny pieces of fatty material that has been deposited in arteries (atheromas or atherosclerotic plaques) break off and travel to small arteries in the brain.
Lacunar infarction tends to occur in older people with diabetes or poorly controlled high blood pressure. Only a small part of the brain is damaged in lacunar infarction, and the prognosis is usually good. However, over time, many small lacunar infarcts may develop and cause problems, including problems with thinking and other mental functions (cognitive impairment).
Large-vessel atherosclerosis
In large-vessel atherosclerosis, atherosclerotic plaques develop in the walls of large arteries, such as those that supply the brain (cerebral arteries).
The plaques can gradually enlarge and cause the artery to narrow. As a result, tissues supplied by the artery may not receive enough blood and oxygen. Plaques tend to split open (rupture). Then material inside the plaque is exposed to the bloodstream. The material triggers the formation of blood clots (called thromboses). These blood clots can suddenly block all blood flow through an artery. Sometimes the blood clots break off, travel through the bloodstream and block an artery that supplies blood to the brain (called emboli). Both thromboses and emboli can cause a stroke by blocking the blood supply to an area of the brain.
Other causes
Several conditions besides rupture of an atheroma can trigger or promote the formation of blood clots, increasing the risk of blockage by a blood clot. They include the following:
Blood disorders: Some disorders, such as an excess of red blood cells (polycythemia), antiphospholipid syndrome, and a high homocysteine level in the blood (hyperhomocysteinemia), make blood more likely to clot. In children, sickle cell disease can cause ischemic stroke.
Oral contraceptives: Taking oral contraceptives, particularly those with a high estrogen dose, increases the risk of blood clots.
An ischemic stroke can also result from any disorder that reduces the amount of blood supplied to the brain. For example,
An ischemic stroke can occur if inflammation of blood vessels (vasculitis) or infection (such as herpes simplex, meningitis, or syphilis) narrows blood vessels that supply the brain.
In atrial fibrillation, the heart does not contract normally, and blood can stagnate and clot. A clot may break loose, then travel to an artery in the brain, and block it.
Sometimes the layers of the walls of an artery that carries blood to the brain (such as arteries in the neck) separate from each other (called dissection) and interfere with blood flow to the brain.
Rarely, a stroke results from a general decrease in blood flow, as occurs when people lose a lot of blood, become severely dehydrated, or have very low blood pressure. This type of stroke often occurs when arteries supplying the brain are narrowed but had not previously caused any symptoms and had not been detected.
Occasionally, an ischemic stroke occurs when blood flow to the brain is normal but the blood does not contain enough oxygen. Disorders that reduce the oxygen content of blood include a severe deficiency of red blood cells (anemia), suffocation, and carbon monoxide poisoning. Usually, brain damage in such cases is widespread (diffuse), and coma results.
Sometimes a blood clot in a leg vein (deep venous thrombosis) or, rarely, small pieces of fat from the marrow of a broken leg bone move into the bloodstream. Usually, these blood clots and pieces of fat travel to the heart and block an artery in the lungs (called pulmonary embolism). However, some people have an abnormal opening between the right and left upper chambers of the heart (called a patent foramen ovale). In such people, the blood clots and pieces of fat may go through the opening and thus bypass the lungs and enter the aorta (the largest artery in the body). If they travel to arteries in the brain, a stroke can result.
Risk factors
Some risk factors for ischemic stroke can be controlled or modified to some extent—for example, by treating the disorder that increases risk.
The major modifiable risk factors for ischemic stroke are
Narrowing (stenosis) of a carotid artery in the neck
Insulin resistance (an inadequate response to insulin), which occurs in type 2 diabetes
Cigarette smoking
Obesity, particularly if the excess weight is around the abdomen
Consumption of too much alcohol
Lack of physical activity
An unhealthy diet (such as one that is high in saturated fats, trans fats, and calories)
Depression or other mental stresses
Heart disorders that increase the risk of blood clots forming in the heart, breaking off, and traveling through the blood vessels as emboli (such a heart attack or an abnormal heart rhythm called atrial fibrillation)
Infective endocarditis (infection of the heart's lining and usually of the heart valves)
Use of or amphetamines
Inflammation of blood vessels (vasculitis)
Clotting disorders that result in excessive clotting
Use of estrogen therapy, including oral contraceptives
Risk factors that cannot be modified include
Having had a stroke previously
Being male
Being older
Having relatives who have had a stroke
Symptoms of Ischemic Stroke
Usually, symptoms of an ischemic stroke occur suddenly and are often most severe a few minutes after they start because most ischemic strokes begin suddenly, develop rapidly, and cause death of brain tissue within minutes to hours. Then, most strokes become stable, causing little or no further damage. Strokes that remain stable for 2 to 3 days are called completed strokes. Sudden blockage by an embolus is most likely to cause this kind of stroke.
In about 10 to 15% of strokes, damage continues to occur and symptoms continue to worsen for up to 2 days, as a steadily enlarging area of brain tissue dies. Such strokes are called evolving strokes. In some people, symptoms affect one arm, then spread to other areas on the same side of the body. The progression of symptoms and damage usually occurs in steps, interrupted by somewhat stable periods. During these periods, the area temporarily stops enlarging or some improvement occurs. Such strokes are usually due to the formation of clots in a narrowed artery.
Strokes caused by an embolus often occur during the day, and a headache may be the first symptom. Strokes caused by a blood clot in a narrowed artery often occur at night and are first noticed when the person wakes up.
Many different symptoms can occur, depending on which artery is blocked and thus which part of the brain is deprived of blood and oxygen (see Brain Dysfunction by Location).
When the arteries that branch from the internal carotid artery (which carry blood along the front of the neck to the brain) are affected, the following are most common:
Blindness in one eye
Loss of vision on either the left side or the right side of both eyes
Abnormal sensations, weakness, or paralysis in one arm or leg or on one side of the body
When the arteries that branch from the vertebral arteries (which carry blood along the back of the neck to the brain) are affected, the following are most common:
Double vision or loss of vision in both eyes
Generalized weakness on one or both sides of the body
Many other symptoms, such as difficulty speaking (for example, slurred speech), impaired consciousness (such as confusion), loss of coordination, and urinary incontinence, can occur.
Severe strokes may lead to stupor or coma. In addition, strokes, even milder ones, can cause depression or an inability to control emotions. For example, people may cry or laugh inappropriately.
Some people have a seizure when the stroke begins. Seizures may also occur months to years later. Late seizures result from scarring or materials that are deposited from blood in the damaged brain tissue.
Occasionally, fever develops. It may be caused by the stroke or another disorder.
If symptoms, particularly impaired consciousness, worsen during the first 2 to 3 days, the cause is often swelling due to excess fluid (edema) in the brain. In large strokes, the swelling in the brain is typically at its worst about 3 days after the stroke begins. Symptoms usually lessen within a few days, as the fluid is absorbed. Nonetheless, the swelling is particularly dangerous because the skull does not expand. The resulting increase in pressure can cause the brain to shift, further impairing brain function, even if the area directly damaged by the stroke does not enlarge. If the pressure becomes very high, the brain may be forced sideways and downward in the skull, through the rigid structures that separate the brain into compartments. The resulting disorder is called herniation, which can be fatal.
Complications of stroke
Strokes can lead to other problems (complications):
If swallowing is difficult, people may not eat enough and become malnourished and dehydrated.
Food, saliva, or vomit may be inhaled (aspirated) into the lungs, resulting in aspiration pneumonia.
Being in one position too long can result in pressure sores and lead to muscle loss, deconditioning, urinary tract infections, and permanent shortening of muscles (contractures).
Not being able to move the legs can result in the formation of blood clots in deep veins of the legs and groin (deep vein thrombosis).
Clots in the deep veins of the legs can break off, travel through the bloodstream, and block an artery to a lung (a disorder called pulmonary embolism).
People may have difficulty sleeping.
The losses and problems resulting from the stroke may make people depressed.
Diagnosis of Ischemic Stroke
A doctor's evaluation
Computed tomography and sometimes magnetic resonance imaging
Laboratory tests, including those to measure blood sugar
Doctors can usually diagnose an ischemic stroke based on the history of events and results of a physical examination. Doctors can usually identify which artery in the brain is blocked based on symptoms. For example, weakness or paralysis of the left leg suggests blockage of the artery supplying the area on the right side of the brain that controls the left leg’s muscle movements.
Doctors often use a standardized set of questions and commands to determine how severe the stroke is, how well people are functioning, and how symptoms are changing over time. These test helps doctors evaluate the person's level of consciousness, ability to answer questions, ability to obey simple commands, vision, arm and leg function, and speech.
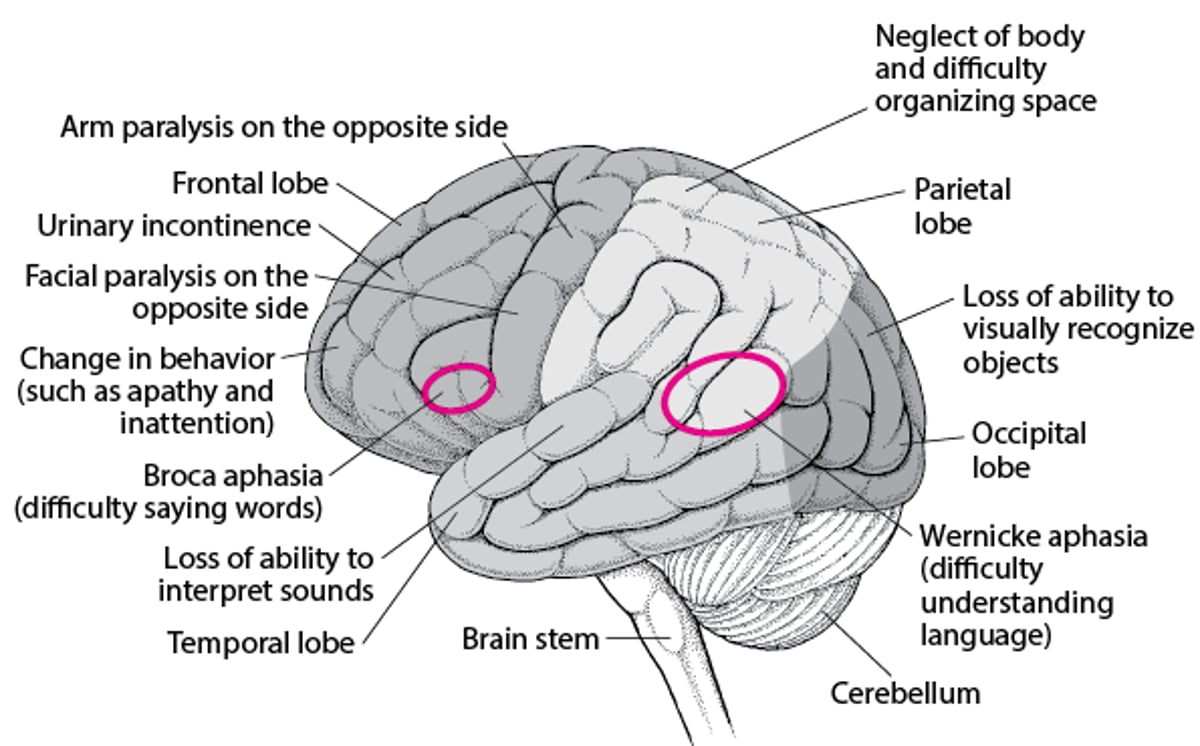
When Specific Areas of the Brain Are Damaged
Different areas of the brain control specific functions. Consequently, where the brain is damaged determines which function is lost. |

Doctors measure the blood sugar level. A low blood sugar level (hypoglycemia) can cause similar symptoms.
Computed tomography (CT) is usually done next. CT helps distinguish an ischemic stroke from a hemorrhagic stroke, a brain tumor, an abscess, and other structural abnormalities. However, during the first hours after some strokes, the CT scan may be normal or show only subtle changes. As a result, diagnosis may be delayed. So if available, diffusion-weighted magnetic resonance imaging (MRI), which can detect ischemic strokes within minutes of their start, may be done next.
As soon as possible, doctors may also do other imaging tests (CT angiography or magnetic resonance angiography) to check for blockages in large arteries. Prompt treatment of these blockages can sometimes limit the amount of brain damage caused by the stroke.
Tests to identify the cause
Identifying the precise cause of an ischemic stroke is important. If the blockage is a blood clot, another stroke may occur unless the underlying disorder is corrected. For example, if blood clots result from an abnormal heart rhythm, treating that disorder can prevent new clots from forming and causing another stroke.
Tests for causes may include the following:
Electrocardiography (ECG) to look for abnormal heart rhythms
Continuous ECG monitoring (done at home or in the hospital) to record the heart rate and rhythm continuously for 24 hours (or more), which may detect abnormal heart rhythms that occur unpredictably or briefly
Echocardiography to check the heart for blood clots, pumping or structural abnormalities, and valve disorders
Imaging tests—color Doppler ultrasonography, magnetic resonance angiography, CT angiography (CT done after a contrast agent is injected into a vein), or cerebral angiography (done using a catheter inserted into an artery to inject the contrast agent)—to determine whether arteries, especially the internal carotid arteries, are blocked or narrowed
Blood tests to check for anemia, polycythemia, blood clotting disorders, vasculitis, and some infections (such as heart valve infections and syphilis) and for risk factors such as high cholesterol levels or diabetes
Urine drug screen for cocaine and amphetamines
Imaging tests enable doctors to determine how narrowed the carotid arteries are and thus to estimate the risk of a subsequent stroke or transient ischemic attack (TIA). Such information helps determine which treatments are needed.
For cerebral angiography, a thin, flexible tube (catheter) is inserted into an artery, usually in the groin, and threaded through the aorta to an artery in the neck. Then, a substance that can be seen on x-rays (radiopaque contrast agent) is injected to outline the artery. Thus, this test is more invasive than other tests that provide images of the brain’s blood supply. However, it provides more information. Cerebral angiography is done before any endovascular procedure that uses a catheter to treat a blocked or narrowed arteries. Cerebral angiography is also done when vasculitis is suspected.
Because CT angiography is less invasive, it has largely replaced cerebral angiography done with a catheter. The exceptions are when endovascular procedures are planned. These procedures involve using instruments threaded through a catheter to physically remove a clot (mechanical thrombectomy), to widen a narrowed artery (angioplasty), and/or to place a tube made of wire mesh (a stent) to keep the artery open.
Treatment of Ischemic Stroke
Measures to support vital functions, such as breathing
Medications to break up blood clots or make blood less likely to clot
Sometimes surgery to remove a blockage or angioplasty with a stent
Measures to manage problems that stroke can cause, such as difficulty swallowing
Measures to prevent blood clots in the legs
Rehabilitation
When a stroke occurs, minutes matter. The longer blood flow to the brain is reduced or stopped, the more brain damage there will be. People who have any symptom suggesting an ischemic stroke should immediately call 911 and go to an emergency department.
Treatment to remove or break up clots is most effective when done as soon as possible. For some medications (thrombolytic therapy) to be effective, they must be started within 4.5 hours of when the stroke began. Procedures to remove clots through a catheter (mechanical thrombectomy) can be effective up to 6 hours after a stroke began and sometimes even later. Starting treatment as soon as possible is crucial because the earlier blood flow is restored to the brain, the less brain damage there is and the better are the chances for recovery. Thus, doctors try to rapidly determine when the stroke began and confirm that the stroke is an ischemic stroke, not a hemorrhagic stroke, which is treated differently.
Generally, doctors do not immediately treat high blood pressure unless it is very high (over 220/120 mm Hg) because when arteries are narrowed, blood pressure must be higher than normal to push enough blood through them to the brain. However, very high blood pressure can injure the heart, kidneys, and eyes and must be lowered.
Specific treatment of stroke may include medications to break up blood clots (thrombolytic therapy) and medications to make blood less likely to clot (antiplatelet medications and anticoagulants), followed by rehabilitation. At some specialized centers, blood clots are physically removed from arteries in the brain (mechanical thrombectomy). Or angioplasty is done to widen the artery. For angioplasty, a catheter with a balloon at its tip is threaded into the narrowed artery (see figure Understanding Percutaneous Coronary Intervention (PCI)). The balloon is then inflated for several seconds to widen the artery. To keep the artery open, doctors insert a tube made of wire mesh (a stent) into the artery.
Thrombolytic (fibrinolytic) medications
Because tPA can cause bleeding in the brain and elsewhere, it usually should not be given to people with certain conditions, such as the following:
Bleeding within the brain or a very large area of dead brain tissue detected by CT or MRI
A suspected hemorrhagic stroke, even if CT does not detect evidence of one
A tendency to bleed (indicated by a low platelet count or abnormal results of other blood tests)
Internal bleeding (hemorrhage)
A recent head injury (within the past 3 months)
A brain disorder that may increase the risk of bleeding, such as some cancers, an arteriovenous malformation (an abnormal connection between arteries and veins), or a cerebral aneurysm (a bulge in the wall of an artery)
Blood pressure that remains high after treatment with an antihypertensive medication
Brain or spinal surgery within the past 3 months
A tendency to bleed or bruise easily
Before tPA is given, CT is done to rule out bleeding in the brain. To be effective and safe, tPA, given intravenously, must be started within 3 hours of the beginning of an ischemic stroke. Some experts recommend using tPA up to 4.5 hours after an ischemic stroke begins.
But when tPA is given between 3 and 4.5 hours, additional conditions may prohibit its use. These conditions include
Being over age 80
Taking an anticoagulant by mouth (regardless of its effect on clotting)
Having a severe stroke that resulted in substantial loss of function
Having a history of both stroke and diabetes mellitus
After 4.5 hours, giving tPA intravenously increases the risk of bleeding.
Pinpointing when the stroke began may be difficult. So doctors assume that the stroke began the last time a person was known to be well. For example, if a person awakens with symptoms of a stroke, doctors assume the stroke began when the person was last seen awake and well. Thus, tPA can be used in only some people who have had a stroke. If advanced imaging identifies undamaged brain tissue, people may be given tPA even if doctors cannot determine when the stroke began—for example, if people wake up and have had a stroke sometime during the night.
Mechanical thrombectomy
For mechanical thrombectomy, doctors use a device to physically remove the blood clot in large cerebral arteries. This procedure is often done when people have had a severe stroke. New evidence suggests that mechanical thrombectomy can effectively treat people who have a stroke, regardless of its severity.
Mechanical thrombectomy is traditionally done within 6 hours of when symptoms began. However, the procedure can be done up to 24 hours after symptoms began if imaging tests show undamaged brain tissue. Thus, at some stroke centers, doctors are starting to use a special type of CT or MRI (perfusion imaging) and other imaging tests to determine how much a stroke has progressed, rather than going strictly by time. These tests can show how much blood flow has been reduced and indicate how much brain tissue may be saved. This approach (based on brain tissue status, not time) is especially useful when doctors are unsure of when the stroke began—for example, when people wake up in the morning and have symptoms of a stroke. If imaging tests show that blood flow is only somewhat reduced, treatment with mechanical thrombectomy up to 24 hours after symptoms start may still be able to save brain tissue. But if blood flow has been greatly reduced or has stopped, treatment after only 1 hour may be unable to save any brain tissue.
Different types of devices can be used. For example, the stent retriever may be used. It resembles a tiny wire cage. It can be attached to a catheter, which is inserted through an incision, often in the groin, and threaded to the clot. The cage is opened up, then closed around the clot, which is drawn out through a larger catheter. If done within 6 hours of the stroke's start, mechanical thrombectomy with a stent retriever can dramatically improve outcomes in people with a large blockage. Devices can restore blood flow in 90 to 100% of people.
Mechanical thrombectomy is done only in stroke centers.
Antiplatelet medications and anticoagulants
aspirin alone for reducing the risk of another stroke, but only if given within 24 hours after stroke symptoms began. It is given only for first 3 weeks after the stroke and reduces the risk of recurrence only for the first 3 months after a stroke. After that, the combination has no advantage over aspirin alone. Also, taking clopidogrel plus aspirin for more than 3 weeks increases the risk of bleeding by a small amount. However, the combination is sometimes given for 3 months in certain circumstances—for example, when people have a partial blockage of a large artery.
If people have been given a thrombolytic medication, doctors usually wait at least 24 hours before antiplatelet medications or anticoagulants are started because these medications add to the already increased risk of bleeding in the brain. Anticoagulants are not given to people who have uncontrolled high blood pressure or who have had a hemorrhagic stroke.
Carotid artery surgery
Once an ischemic stroke is completed, surgical removal of fatty deposits (atheromas, or plaques) due to atherosclerosis or clots in an internal carotid artery may be done (see figure Supplying the Brain With Blood). This procedure, called carotid endarterectomy, can help if all of the following are present:
The stroke resulted from narrowing of a carotid artery by more than 70% (more than 60% in people who have been having transient ischemic attacks).
Some brain tissue supplied by the affected artery still functions after the stroke.
The person’s life expectancy is at least 5 years.
In such people, carotid endarterectomy may reduce the risk of subsequent strokes. This procedure also reestablishes the blood supply to the affected area, but it cannot restore lost function because some brain tissue is dead.
For carotid endarterectomy, a general anesthetic is used. The surgeon makes an incision in the neck over the area of the artery that contains the blockage, then an incision in the artery. The blockage is removed, and the incisions are closed. For a few days afterwards, the neck may hurt, and swallowing may be difficult. Most people stay in the hospital 1 or 2 days. Heavy lifting should be avoided for about 3 weeks. After several weeks, people can resume their usual activities.
Carotid endarterectomy can trigger a stroke because the operation may dislodge clots or other material that can then travel through the bloodstream and block an artery. However, after the operation, the risk of stroke is lower than it is when medications are used, and this risk is lower for several years. The procedure can result in a heart attack because people who have this procedure often have risk factors for coronary artery disease.
People should find a surgeon who is experienced doing this operation and who has a low rate of serious complications (such as heart attack, stroke, and death) after the operation. If people cannot find such a surgeon, the risks of endarterectomy may outweigh its expected benefits.
Carotid artery angioplasty and stenting
If endarterectomy is too risky or cannot be done because of the artery's anatomy, a less invasive procedure (carotid artery angioplasty) can be done to widen the artery.
For this procedure, a local anesthetic is given. Then a catheter with an umbrella filter at its tip is inserted through a small incision into a large artery near the groin or in the arm, and the catheter is threaded to the internal carotid artery in the neck. A substance that can be seen on x-rays (radiopaque contrast agent) is injected, and x-rays are taken so that the narrowed area can be located. Doctors use the catheter to widen the carotid artery, then insert a tube made of wire mesh (a stent) into the artery. Once in place, the stent is expanded to help keep the artery open. The filter catches any debris that may break off during the procedure.
After the stent is placed, the catheter and the filter at its tip are removed. People remain awake for the procedure, which usually takes 1 to 2 hours.
Placement of a stent appears to be as safe and as effective in preventing strokes and death as endarterectomy. For younger people and people who do not have risk factors for heart or blood vessel disorders (such as high blood pressure, high cholesterol levels, diabetes, and smoking), carotid endarterectomy is usually done.
A similar procedure can be done for other types of large blocked arteries (see figure Understanding Percutaneous Coronary Intervention (PCI)).
Long-term treatment of strokes
Long-term treatment of stroke includes measures to do the following:
Control problems that can make the effects of stroke worse
Prevent or treat problems caused by strokes
Prevent future strokes
Treat any disorders that are also present
During the recovery period, high blood sugar (hyperglycemia) and fever can make brain damage worse after a stroke. Lowering them limits the damage and results in better functioning.
Before people who have had a stroke start to eat, drink, or take medications by mouth, they are checked for problems with swallowing. Problems with swallowing can lead to aspiration pneumonia. Measures to prevent this problem are started early. If problems are detected, a therapist can teach people how to swallow safely. Sometimes people need to be fed through a tube (tube feeding).
If people cannot move on their own or have difficulty moving, they are at risk of developing blood clots in their legs (deep vein thrombosis) and pressure sores
Measures to prevent pressure sores are started early. For example, staff members periodically change the person's position in bed to help prevent pressure sores from forming. They also regularly inspect the skin for any sign of pressure sores.
Controlling or treating risk factors for stroke (such as high blood pressure, diabetes, smoking, consumption of too much alcohol, high cholesterol levels, and obesity) can help prevent future strokes.
Statinsatherosclerosis). Such therapy can help prevent strokes from recurring.
Antiplatelet medications, taken by mouth, may be used to reduce the risk of blood clots and thus help prevent strokes due to atherosclerosis. One of the following can be used:
aspirin.
aspirin alone, but only for the first 3 months after a stroke. After that, the combination has no advantage over aspirin alone. Also, taking clopidogrel plus aspirin
Anticoagulants
warfarinwarfarin.
People who have atrial fibrillation or a heart valve disorder
If other disorders such as heart failure, abnormal heart rhythms, and lung infections are present, they must be treated.
Because a stroke often causes mood changes, especially depression, family members or friends should inform the doctor if the person seems depressed. Depression can be treated with antidepressants and psychotherapy.
Prognosis for Ischemic Stroke
The sooner a stroke is treated with a medication that breaks up blood clots (thrombolytic medication), the less severe brain damage is likely to be and the better the chances for recovery.
During the first few days after an ischemic stroke, doctors usually cannot predict whether a person will improve or worsen. Younger people and people who start improving quickly are likely to recover more fully.
About 50% of people with one-sided paralysis and most of those with less severe symptoms recover some function by the time they leave the hospital, and they can eventually take care of their basic needs. They can think clearly and walk adequately, although use of the affected arm or leg may be limited. Use of an arm is more often limited than use of a leg.
About 10% of people who have an ischemic stroke recover all normal function.
Some people are physically and mentally devastated and unable to move, speak, or eat normally.
About 20% of people who have an ischemic stroke die within 28 days. The proportion is higher among older people. About 25% of people who recover from a first stroke have another stroke within 5 years. Subsequent strokes impair function further.
Most impairments still present after 12 months are permanent.






