Secretory otitis media occurs when fluid accumulates behind the eardrum and remains there after an acute middle ear infection or blockage of the eustachian tube.
A previous ear infection is the usual cause, but some children may develop it as a result of a blocked eustachian tube.
Children typically have no pain, but fluid can impair hearing.
Diagnosis involves physical examination of the eardrum and sometimes tympanometry.
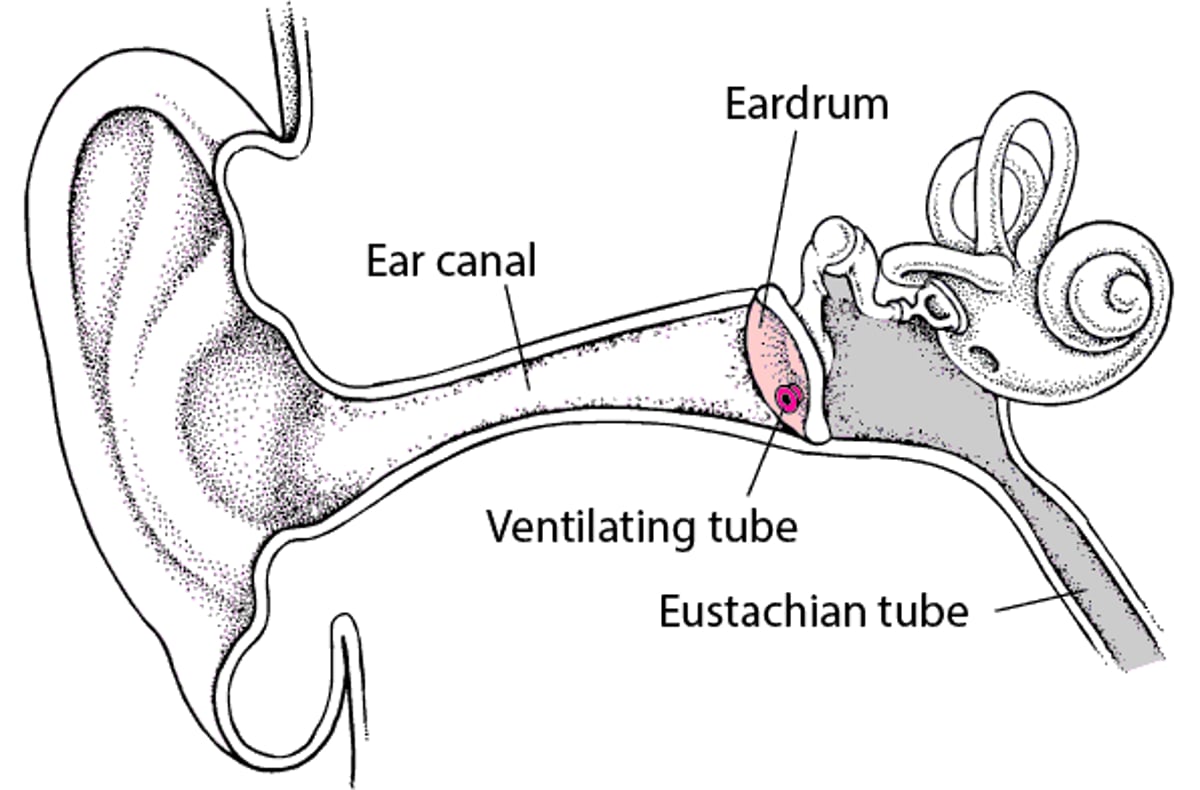
Secretory otitis media usually resolves without treatment, but some children need surgery to install a ventilating tube in their eardrum.
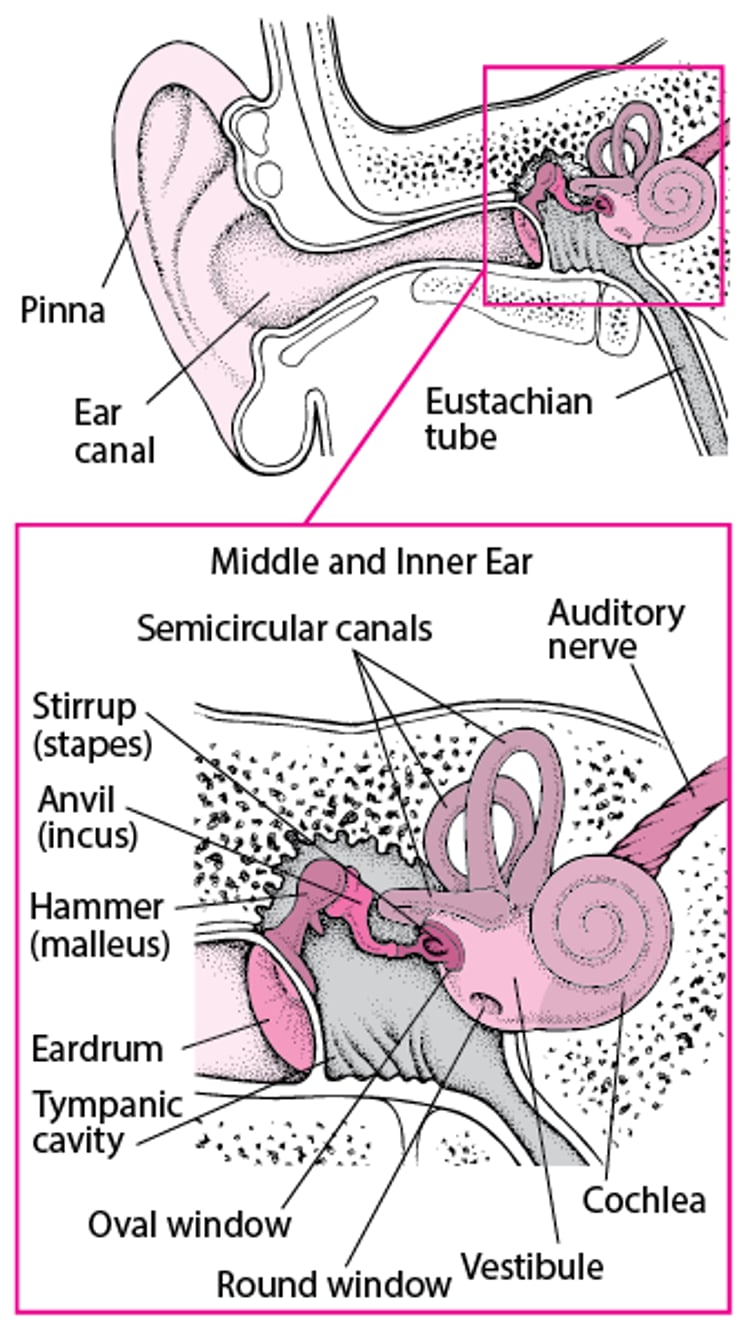
A Look Inside the Ear

Secretory otitis media often occurs after an acute middle ear infection. The fluid that has accumulated behind the eardrum during the acute infection remains after the infection resolves. Secretory otitis media may also occur without a preceding ear infection. It may be due to a blockage of the eustachian tube (the tube that connects the middle ear with the nasal passages) by an infection, enlarged adenoids (collections of lymphoid tissue located where the throat and nasal passages meet), tumors (rarely), or possibly gastroesophageal reflux disease. Allergies (such as seasonal allergies or year-round allergies) may also make secretory otitis media more likely to develop. Secretory otitis media is extremely common among children aged 3 months to 3 years.
(See also Overview of Middle Ear Infections in Young Children and see Otitis Media (Secretory) in adults.)

Symptoms
Although this disorder is usually painless, the fluid often impairs hearing. Hearing may be impaired sufficiently to affect the understanding of speech, language development, learning, and behavior. Children may have a feeling of fullness, pressure, or popping in the ear with swallowing.
Diagnosis
A doctor's examination of the eardrum
Sometimes tympanometry
Doctors diagnose secretory otitis media by looking for changes in the color and appearance of the eardrum and by gently blowing air into the ear using a rubber bulb to see whether the eardrum moves. If the eardrum does not move but there is no redness or bulging and the child has few symptoms, secretory otitis media is likely.
If examination findings are unclear, doctors often do tympanometry. In tympanometry, a device containing a microphone and a sound source is placed snugly in the ear canal, and sound waves are bounced off the eardrum as the device varies the pressure in the ear canal.
Doctors examine the nasal passages and throat in adolescents to check for tumors.
Treatment
Often no treatment
Sometimes myringotomy with or without tubes
Sometimes adenoidectomy
Secretory otitis media often resolves by itself, usually in 2 or 3 weeks. Antibiotics or other drugs, such as decongestants, are not helpful. Children who have allergies may be given antihistamines by mouth, a corticosteroid nasal spray, or both.
If the disorder persists and children do not improve after 1 to 3 months, surgery may help. Sometimes, myringotomy is done. For this procedure, doctors make a tiny slit in the eardrum, remove the fluid, and insert a small ventilating tube called a tympanostomy tube in the slit to provide drainage from the middle ear to the outer ear. The adenoids may be removed at the same time (called adenoidectomy). Sometimes a myringotomy is done only to remove fluid and not insert ventilating tubes. If fluid is removed but no tubes are inserted, the procedure is called tympanic membrane perforation or tympanocentesis.
Occasionally, the middle ear can be opened temporarily using a Valsalva maneuver or politzerization. Both techniques require that the child is capable of following instructions and does not have an infection causing a runny nose. To do the Valsalva maneuver, the child keeps the mouth closed and tries to forcibly blow air out through the pinched nostrils (popping the ear). To do politzerization, the doctor uses a special syringe to blow air into one of the child’s nostrils and blocks the other nostril while the child swallows.
Air travel and scuba diving should be avoided or delayed if possible because they can cause painful changes in pressure in the ear. If air travel cannot be avoided, young children may be helped by chewing food or drinking (for example, from a bottle). A Valsalva maneuver or politzerization may help older children.
Antibiotics are given to treat nasal and sinus infections caused by bacteria.
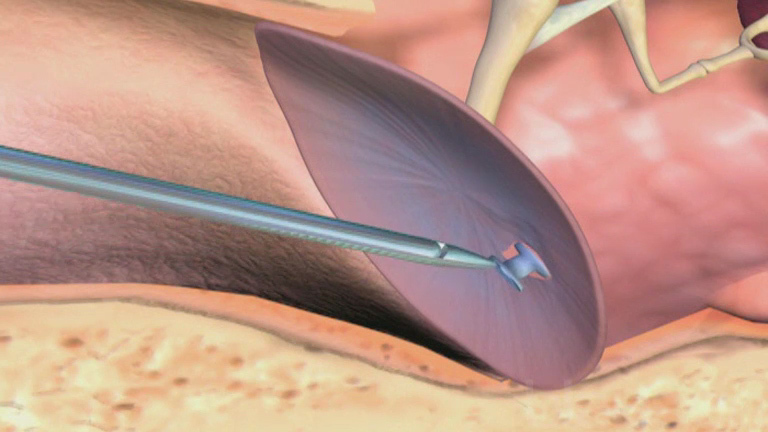
Myringotomy: Treating Recurring Ear Infections
During a myringotomy, doctors make a small opening in the eardrum to allow fluid to drain from the middle ear. Then they place a tiny, hollow plastic or metal tube (tympanostomy tube, or ventilating tube) in the eardrum through the opening. These tubes balance the pressure in the environment with that in the middle ear. Doctors recommend ventilating tubes for some children who have had recurring ear infections (acute otitis media) or recurring or persistent collections of fluid in their middle ears (chronic serous otitis media). Placement of ventilating tubes is a common surgical procedure that is done in a hospital or doctor’s office. General anesthesia or sedation is usually required. After the procedure, children usually go home within a few hours. Antibiotic ear drops are sometimes given after the procedure for about a week. The tubes usually come out on their own after about 6 to 12 months, but some types stay in longer. Tubes that do not come out on their own are removed by the doctor, sometimes under general anesthesia or sedation. If the opening does not close on its own, it may need to be closed surgically. Children with ventilating tubes may wash their hair and go swimming, but some doctors recommend children do not submerge their head in deep water without using earplugs. Drainage of fluid from the ears indicates an infection, and the doctor should be notified. |