


Bleeding may occur anywhere along the digestive (gastrointestinal or GI) tract, from the mouth to the anus. Blood may be easily seen by the naked eye (overt), or blood may be present in amounts too small to be visible (occult). Occult bleeding is detected only by testing a stool specimen with special chemicals.
Hematemesis is blood that is visible in vomit. Hematemesis indicates the bleeding is coming from the upper GI tract, usually from the esophagus, stomach, or the first part of the small intestine. When blood is vomited, it may be bright red if bleeding is brisk and ongoing. Alternatively, vomited blood may have the appearance of coffee grounds. It results from bleeding that has slowed or stopped, and the blood looks like coffee grounds because it has been partially digested by acid in the stomach.
Blood may also be passed from the rectum:
As black, tarry stools (melena)
As bright red blood (hematochezia)
In apparently normal stool if bleeding is less than a few teaspoons per day
Melena is more likely when bleeding comes from the esophagus, stomach, or small intestine. The black color of melena is caused by blood that has been exposed for several hours to stomach acid and enzymes and to bacteria that normally reside in the large intestine. Melena may continue for several days after bleeding has stopped.
Hematochezia is more likely when bleeding comes from the large intestine, although it can be caused by very rapid bleeding from the upper portions of the digestive tract as well.
People who have lost only a small amount of blood may feel well otherwise. However, serious and sudden blood loss may be accompanied by a rapid pulse, low blood pressure, and reduced urine flow. A person may also have cold, clammy hands and feet. Severe bleeding may reduce the flow of blood to the brain, causing confusion, disorientation, sleepiness, and even extremely low blood pressure (shock). Slow, chronic blood loss may cause symptoms and signs of low blood count (anemia), such as weakness, easy fatigue, paleness (pallor), chest pain, and dizziness. People with underlying ischemic heart disease may develop chest pain (angina) or a have a heart attack (myocardial infarction) because of decreased blood flow through the heart.
(See also Overview of Digestive Symptoms.)
Causes of Gastrointestinal Bleeding
The causes of GI bleeding are divided into three areas:
Upper GI tract
Lower GI tract
Small intestine
(See table Some Causes and Features of Gastrointestinal Bleeding.)
The most common causes are difficult to specify because causes vary by the area that is bleeding and the person's age.
However, in general, the most common causes of upper GI bleeding are
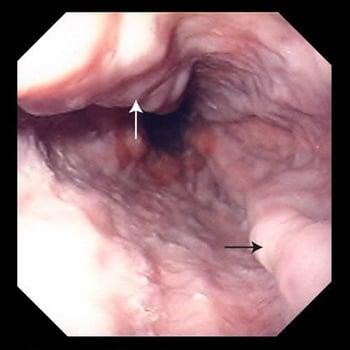
Enlarged veins in the esophagus (esophageal varices)
A tear in the lining of the esophagus after vomiting (Mallory-Weiss syndrome)

The most common causes of lower GI bleeding are
Abnormal blood vessels (angiodysplasia, arteriovenous malformations [AVMs])
Other causes of lower GI bleeding include a split in the skin of the anus (anal fissure), ischemic colitis, and large-bowel inflammation resulting from radiation or poor blood supply.
Bleeding from the small intestine is rare but can result from blood vessel abnormalities, tumors, or a Meckel diverticulum.

Bleeding from any cause is more likely, and potentially more severe, in people who have chronic alcohol-related liver disease or chronic hepatitis, who have hereditary disorders of blood clotting, or who are taking certain medications. Liver disease makes bleeding more likely because a poorly functioning liver produces fewer of the proteins that help blood clot (blood clotting factors).
Medications that can cause or worsen bleeding include
Anticoagulants (such as heparin, warfarin, dabigatran, apixaban, rivaroxaban, and edoxaban)
Those that affect platelet function (such as aspirin and certain other nonsteroidal anti-inflammatory drugs [NSAIDs] and clopidogrel)
Those that affect mood or mental health (such as selective serotonin reuptake inhibitors [SSRIs])
Those that affect the stomach's protective barrier against acid (such as NSAIDs)
Evaluation of Gastrointestinal Bleeding
GI bleeding typically requires evaluation by a doctor. The following information can help people decide when a doctor’s evaluation is needed and help them know what to expect during the evaluation.
Warning signs
In people with GI bleeding, certain symptoms and characteristics are cause for concern. They include
Fainting (syncope)
Sweating (diaphoresis)
Rapid heart rate (over 100 beats per minute)
Passing in stool or vomiting more than 1 cup (250 milliliters) of blood
When to see a doctor
People who have GI bleeding should see a doctor right away unless the only sign of bleeding is blood on the toilet paper after a bowel movement. If people with such findings have no warning signs and feel otherwise well, a delay of a day or two is not harmful.
What the doctor does
Doctors first ask questions about the person's symptoms and medical history. Doctors then do a physical examination. What they find during the history and physical examination often suggests a cause of the GI bleeding and the tests that may need to be done (see table Some Causes and Features of Gastrointestinal Bleeding).
The history is focused on finding out exactly where the bleeding is coming from, how rapid it is, and what is causing it. Doctors need to know how much blood (for instance, a few teaspoons or several clots) is being passed and how often blood is being passed. People with hematemesis are asked whether blood was passed the first time they vomited or only after they vomited a few times with no blood.
Doctors ask people with rectal bleeding whether pure blood was passed; whether it was mixed with stool, pus, or mucus; or whether blood simply coated the stool. People with bloody diarrhea are asked about recent travel or other possible forms of exposure to other agents that can cause digestive tract illness (for instance, bacterial infections).
Doctors then ask about symptoms of abdominal discomfort, weight loss, and easy bleeding or bruising and symptoms of anemia (such as weakness, easy exhaustion [fatigability], and dizziness).
Doctors need to know about any current or past digestive tract bleeding and the results of any previous colonoscopy (an examination of the entire large intestine, the rectum, and the anus using a flexible viewing tube). People should tell doctors whether they have inflammatory bowel disease, bleeding tendencies, or liver disease and whether they use any medications that increase the likelihood of bleeding (such as aspirin, NSAIDs, or anticoagulants) or drugs that can cause chronic liver disease (such as alcohol).
The physical examination is focused on the person’s vital signs (such as pulse, breathing rate, blood pressure, and temperature) and other indicators of shock or a decrease in the volume of circulating blood (hypovolemia—rapid heart rate, rapid breathing, pallor, sweating, little urine production, and confusion) and anemia.
Doctors also look for small purplish red (petechiae) and bruise-like (ecchymoses) spots on the skin, which are signs of bleeding disorders. Doctors also look for signs of chronic liver disease (such as spider angiomas, fluid in the abdominal cavity [ascites], and red palms) and portal hypertension (such as an enlarged spleen and dilated abdominal wall veins).
Doctors do a rectal examination to look at stool color and check it for blood and to search for tumors and fissures. Doctors also examine the anus to look for hemorrhoids.
Testing
The need for tests depends on what doctors find during the history and physical examination, particularly whether warning signs are present.
There are four main testing approaches to GI bleeding:
Blood tests and other laboratory studies
Upper endoscopy for suspected upper GI tract bleeding
Colonoscopy for lower GI tract bleeding (unless clearly caused by hemorrhoids)
Angiography or CT angiography if bleeding is rapid or severe
The person’s blood count helps indicate how much blood has been lost. A low platelet count is a risk factor for bleeding. Other blood tests include prothrombin time (PT), partial thromboplastin time (PTT), and liver tests, all of which help detect problems with blood clotting. Doctors often do not do blood tests on people who have minor bleeding caused by hemorrhoids.
If the person has vomited blood or dark material (which may represent partially digested blood), the doctor sometimes passes a small, hollow plastic tube through the person’s nose down into the stomach (nasogastric tube—see Intubation of the Digestive Tract) and suctions out the stomach contents. Bloody or pink contents indicate active upper GI bleeding, and dark or coffee-ground material indicates that bleeding is slow or has stopped. Sometimes, there is no sign of blood even though the person was bleeding very recently. A nasogastric tube may be inserted in anyone who has not vomited but has passed a large amount of blood from the rectum (if not from an obvious hemorrhoid) because this blood may have originated in the upper digestive tract.
If the nasogastric tube reveals signs of active bleeding, or the person’s symptoms strongly suggest the bleeding is originating in the upper digestive tract, the doctor usually does upper endoscopy. Upper endoscopy is a visual examination of the esophagus, stomach, and the first segment of the small intestine (duodenum) using a flexible tube called an endoscope. An upper endoscopy allows the doctor to see the bleeding source and often treat it and is often done without a nasogastric tube being passed.
People with symptoms typical of hemorrhoids may need only sigmoidoscopy (examination of the lower part of the large intestine, the rectum, and anus using an endoscope) or anoscopy (examination of only the rectum, using a short scope and light source). All other people with hematochezia should have colonoscopy (examination of the entire large intestine, the rectum, and the anus using an endoscope).
Occasionally, upper endoscopy and colonoscopy do not show the cause of bleeding. There are still other options for finding the source of the bleeding. Doctors may do endoscopy of the small bowel (enteroscopy). If bleeding is rapid or severe, doctors sometimes do angiography. During angiography, doctors use a catheter to inject an artery with a contrast agent that can be seen on x-rays. Angiography helps doctors diagnose upper digestive tract bleeding and allows them to do certain treatments (such as embolization and vasoconstrictor infusion—see Stopping the bleeding). Doctors may also inject the person with red blood cells labeled with a radioactive marker (radionuclide scanning). With the use of a special scanning camera, the radioactive marker can sometimes show the approximate location of the bleeding. Before doing angiography or surgery, doctors may also do a test called CT angiography. During this procedure, a type of imaging called computed tomography (CT) and a radiopaque contrast agent are used to produce images of blood vessels and sometimes can show the location of the bleeding.
Doctors may do a small-bowel follow-through, which is a series of detailed x-rays of the small intestine. This test has largely been replaced by CT enterography, which is used to evaluate the inside of the small intestine for tumors.
Another option is video capsule endoscopy, in which people swallow a tiny camera that takes pictures as it passes through the intestines. Video capsule endoscopy is especially useful in the small intestine, but it is not very useful in either the colon or stomach because these organs are easier to see using endoscopy.
Treatment of Gastrointestinal Bleeding
There are two goals to treating people with GI bleeding:
Replace lost blood with fluid given by vein (intravenously) and sometimes with a blood transfusion.
Stop any ongoing bleeding.
Hematemesis, hematochezia, or melena should be considered an emergency. People with severe GI bleeding should be admitted to an intensive care unit (ICU) or other closely monitored setting and should be seen by a gastroenterologist and a surgeon.
Replacing fluids and blood
People with sudden, severe blood loss require intravenous fluids and sometimes an emergency blood transfusion to stabilize their condition. People with blood clotting abnormalities may require transfusion of platelets or fresh frozen plasma or preparations of blood clotting proteins (prothrombin complex concentrates).
Stopping the bleeding
Most GI bleeding stops without treatment. Sometimes, however, it does not. The type and location of bleeding tell the doctors what treatment to use. For example, doctors can often stop peptic ulcer bleeding during endoscopy by using a device that uses an electrical current to produce heat (electrocautery), heater probes, or injections of certain agents. If endoscopy does not stop the bleeding, surgery may be needed.
For esophageal varices (enlarged veins in the esophagus), doctors try to stop bleeding with endoscopic banding, injection sclerotherapy, placement of a tube with balloons to compress the varices, or a transjugular intrahepatic portosystemic shunting
Polyps can be removed by a wire snare or electrocautery.
Doctors may give people with upper GI bleeding a proton pump inhibitor (PPI) by vein (intravenously) to help control the bleeding.
Internal hemorrhoid bleeding stops spontaneously in most cases. For people whose bleeding does not stop without treatment, doctors do anoscopy and may place rubber bands around the hemorrhoids or inject them with substances that stop bleeding or do electrocautery or surgery (see treatment of hemorrhoids).
Essentials for Older People: Gastrointestinal Bleeding
In older people, hemorrhoids and colorectal cancer are the most common causes of minor bleeding. Peptic ulcers, diverticular disease (such as diverticulitis), and abnormal blood vessels (angiodysplasia) are the most common causes of major bleeding. Bleeding from enlarged veins in the esophagus (esophageal varices) is less common than in younger people.
Older people poorly tolerate massive GI bleeding. Doctors must diagnosis older people quickly, and treatment must be started sooner than in younger people, who can better tolerate repeated episodes of bleeding.
Key Points
Rectal bleeding may result from upper or lower GI bleeding.
Most people stop bleeding spontaneously.
Endoscopy is usually the first treatment choice for people whose bleeding does not stop without treatment.






