

Because distinct flavors depend on aromas to stimulate the olfactory chemoreceptors, smell and taste are physiologically interdependent. Dysfunction of one often disturbs the other. Disorders of smell and taste are rarely incapacitating or life threatening, so they often do not receive close medical attention, although their effect on quality of life can be severe.
Conditions, such as infections, smoking, pregnancy, aging, depression, and seizures, and nutritional deficiencies (eg, of zinc, copper, or nickel), cause distortions of taste and smell. Some cause one or the other.Conditions, such as infections, smoking, pregnancy, aging, depression, and seizures, and nutritional deficiencies (eg, of zinc, copper, or nickel), cause distortions of taste and smell. Some cause one or the other.
Taste
Abnormal taste sensations may be caused by a variety of conditions, including psychiatric disorders. However, local causes should always be sought first.
Some causes include drying of the oral mucosa caused by heavy smoking, Sjögren syndrome, radiation therapy of the head and neck, or desquamation of the tongue can impair taste, and various medications (eg, those with anticholinergic properties, vincristine) alter taste. In all instances, the gustatory receptors are diffusely involved. , radiation therapy of the head and neck, or desquamation of the tongue can impair taste, and various medications (eg, those with anticholinergic properties, vincristine) alter taste. In all instances, the gustatory receptors are diffusely involved.
When limited to one side of the tongue (eg, in Bell palsy), ageusia (loss of the sense of taste) is rarely noticed. Sudden loss of taste may be an early symptom of COVID-19, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Distortions of taste (dysgeusia) may be caused by gingivitis, xerostomia, or many of the same conditions that also result in loss of smell. Dysgeusia may also be caused by some medications, such as the following:
Antibiotics
Antiseizure medications
Antidepressants
Certain chemotherapy medications
Diuretics
Medications used to treat arthritis
Thyroid medications
Glossopharyngeal and facial nerve integrity can be determined by testing taste on both sides of the dorsum of the tongue with sugar, salt, vinegar (sour), and quinine (bitter).
Smell
The inability to detect certain odors, such as gas or smoke, may be dangerous, and several systemic and intracranial disorders should be excluded before dismissing symptoms as harmless. Disorders of smell typically tend to involve the olfactory bulb and related pathways. Although implicated in disorders of taste, whether brain stem disease (involvement of the nucleus solitarius) can cause disorders of smell is uncertain because other neurologic manifestations usually take precedence.
Anosmia (complete loss of the sense of smell) is probably the most common abnormality. Hyperosmia (increased sensitivity to odors) usually reflects a neurotic or histrionic personality but can occur intermittently with seizure disorders. Dysosmia (disagreeable or distorted sense of smell) may occur in patients with infection of the nasal sinuses, partial damage to the olfactory bulbs, or mental depression. Some cases, accompanied by a disagreeable taste, result from poor dental hygiene. Seizure activity that originates in the uncus of the temporal lobe can cause brief, vivid, unpleasant olfactory hallucination; rarely herpes encephalitis causes olfactory hallucinations. Hyposmia (partial loss of smell) and hypogeusia (diminished sense of taste) can follow acute influenza, usually temporarily. Sudden loss of smell may be an early symptom of COVID-19.
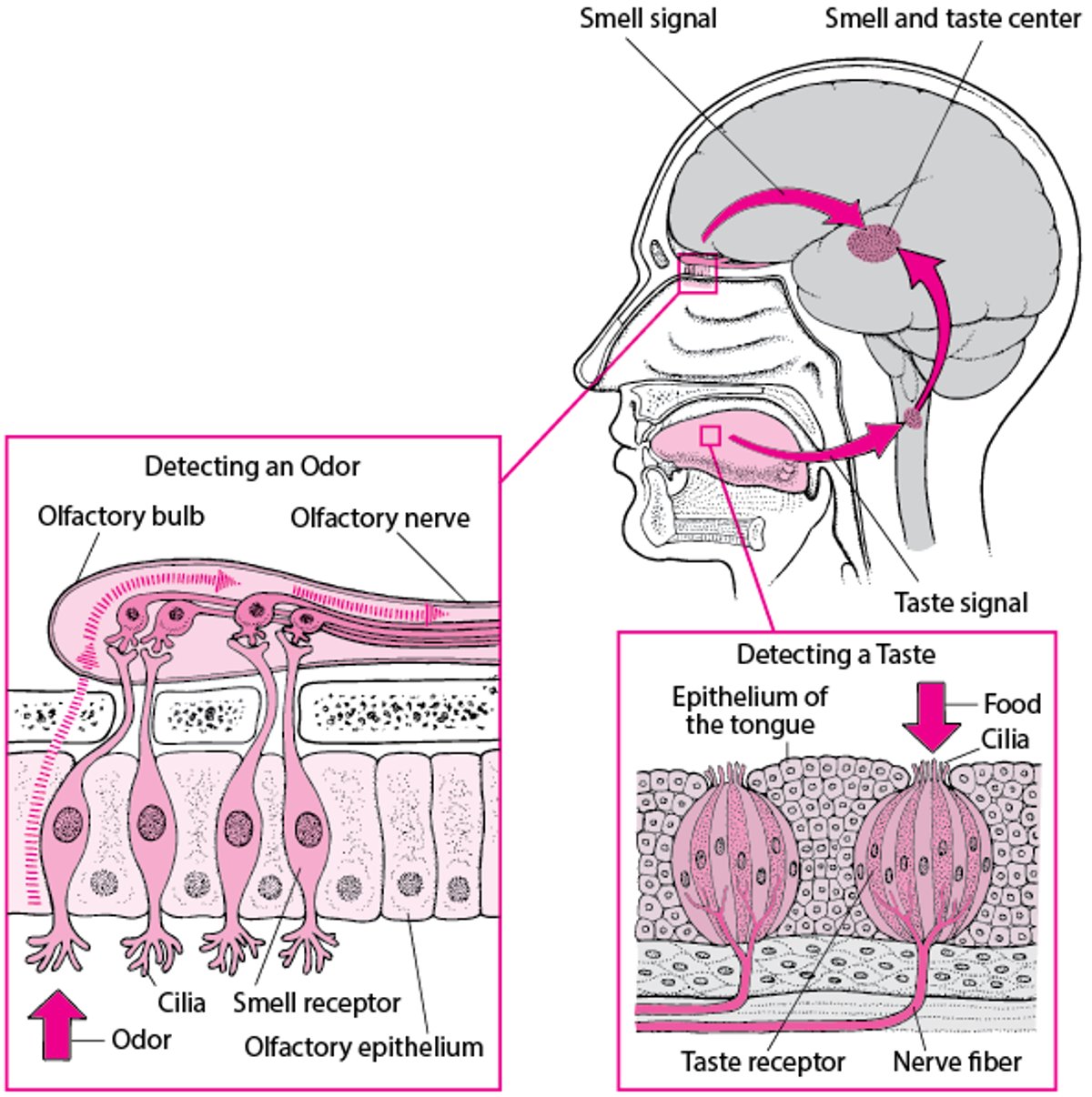
How People Sense Flavors
To distinguish most flavors, the brain needs information about both smell and taste. These sensations are communicated to various areas of the brain from receptors in the nose and mouth. The olfactory epithelium is an area of the nasal mucosa in the upper part of the nasal cavity. The smell receptors in this epithelium are specialized nerve cells with cilia that detect odors. Airborne molecules entering the nasal passage stimulate the cilia, triggering a nerve impulse that is transmitted upward through the cribriform plate and across a synapse within the olfactory bulbs (the distal ends of the 1st cranial (olfactory) nerves. The olfactory nerves transmit the impulse to the brain, which interprets the impulse as a distinct odor. Information is also sent to the middle part of the temporal lobe (the smell and taste center), in which memories of odors are stored. Thousands of tiny taste buds cover most of the tongue’s surface. A taste bud contains several types of ciliated taste receptors. Each type detects one of the five basic tastes: sweet, salty, sour, bitter, or savory (also called umami, the taste of monosodium glutamate). The sensitivity of specific areas of the tongue may vary for each taste (eg, the tip of the tongue for sweetness, the front sides for saltiness, along the sides for sourness, and the back one-third for bitterness); however, these tastes can be detected all over the tongue, and the contribution of regional differences to taste sensation is probably minor. Nerve impulses from the taste buds are transmitted to the brain through the facial and glossopharyngeal nerves (cranial nerves VII and IX). The brain interprets the combination of impulses from the olfactory and taste receptors along with other sensory information (eg, the food’s texture and temperature) to produce a distinct flavor when food enters the mouth and is chewed. |

Geriatrics Essentials: Smell and Taste
After age 50, the ability to smell and to taste gradually begins to decrease. The olfactory epithelium becomes thinner and drier, and the olfactory nerves deteriorate. Older people can still detect strong odors, but detecting subtle odors is more difficult.
With aging, the number of taste buds also decrease, and those that are left become less sensitive. These changes tend to reduce the ability to taste sweet and salt more than the ability to taste sour and bitter. Thus, many foods start to taste bitter.
Because smell and taste are diminished with aging, many foods taste bland. The mouth tends to be dry more often, further reducing the ability to taste and smell. Also, many older adults have a disorder or take medications that contribute to dry mouth. Due to these changes, older adults may decrease their food intake, which can lead to inadequate nutrition. This lack of essential nutrients may exacerbate existing health conditions and contribute to a decline in overall well-being.
Drugs Mentioned In This Article





