

Ninety percent of laryngeal cancer is squamous cell carcinoma. Smoking, excessive alcohol use, lower socioeconomic status, and being male and > 60 years increase risk. Early diagnosis is common with vocal cord tumors because hoarseness develops early. However, supraglottic tumors (above the vocal cords) and subglottic tumors (below the vocal cords) often manifest at an advanced stage because they can remain asymptomatic for a longer time frame. Diagnosis is based on laryngoscopy and biopsy. Treatment of early-stage tumors is with surgery or radiation. Advanced-stage tumors are often treated with chemotherapy and radiation therapy. Surgery is used for salvage treatment or lesions with extralaryngeal extension or cartilage destruction. Reestablishment of speaking ability is needed if a total laryngectomy is done.
(See also Overview of Head and Neck Tumors.)
Squamous cell carcinoma is the most common cancer of the larynx. In the United States, it is 4 times more common among males and is more common among people of lower socioeconomic status. Over 95% of patients smoke; 15 pack-years of smoking increase the risk 30-fold. The incidence of laryngeal cancer is estimated to be 12,650 new cases in 2024; the annual number of new cases is decreasing, particularly among males, most likely due to changes in smoking habits. Annual deaths are estimated to be 3880 in 2024 (1).
Forty-nine percent of patients present with localized disease alone; 28% present with local disease and regional nodal metastatic disease; and 16% present with metastases; and 7% are not staged (2). Lymph node metastasis are more common in supraglottic and subglottic tumors than with glottic cancers due to the minimal lymphatic drainage of the glottis and because glottic tumors cause symptoms earlier. Distant metastases occur most frequently in the lungs and liver.
Common sites of origin are the true vocal cords (glottis) and the supraglottic larynx. The least common site is the subglottic larynx, where only 1% of primary laryngeal cancers originate. Verrucous carcinoma, a rare variant of squamous cell carcinoma, usually arises in the glottic area and has a better survival rate than standard squamous cell carcinoma.
General references
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024 [published correction appears in CA Cancer J Clin. 2024 Mar-Apr;74(2):203. doi: 10.3322/caac.21830]. CA Cancer J Clin 2024;74(1):12-49. doi:10.3322/caac.21820
2. National Cancer Institute: Surveillance, Epidemiology, and End Results Program: Cancer Stat Facts: Laryngeal Cancer. Laryngeal Cancer — Cancer Stat Facts Accessed July 30, 2024.
Symptoms and Signs of Laryngeal Cancer
Symptoms and signs of laryngeal cancer differ based on the involved portion of the larynx.
Patients with supraglottic cancer often present with dysphagia; other common symptoms include airway obstruction, otalgia, development of a neck mass. Hoarseness is a common late symptom of supraglottic cancer. Patients with these symptoms should be referred for direct laryngoscopy without delay.
In glottic cancers, hoarseness is common early.
Patients with subglottic cancer often present with airway obstruction, and hoarseness is a common late symptom.
Diagnosis of Laryngeal Cancer
Laryngoscopy
Operative endoscopy and biopsy
Imaging tests for staging
All patients who have hoarseness for > 2 to 3 weeks should have their larynx examined by a head and neck specialist. Some clinicians use a mirror to evaluate the larynx, but most often a flexible fiberoptic examination is done. Any lesions discovered require further evaluation, usually with operative endoscopy and biopsy, with concomitant evaluation of the upper airway and gastrointestinal tract for coexisting cancers. The incidence of a synchronous second primary tumor may be as high as 10% (1).

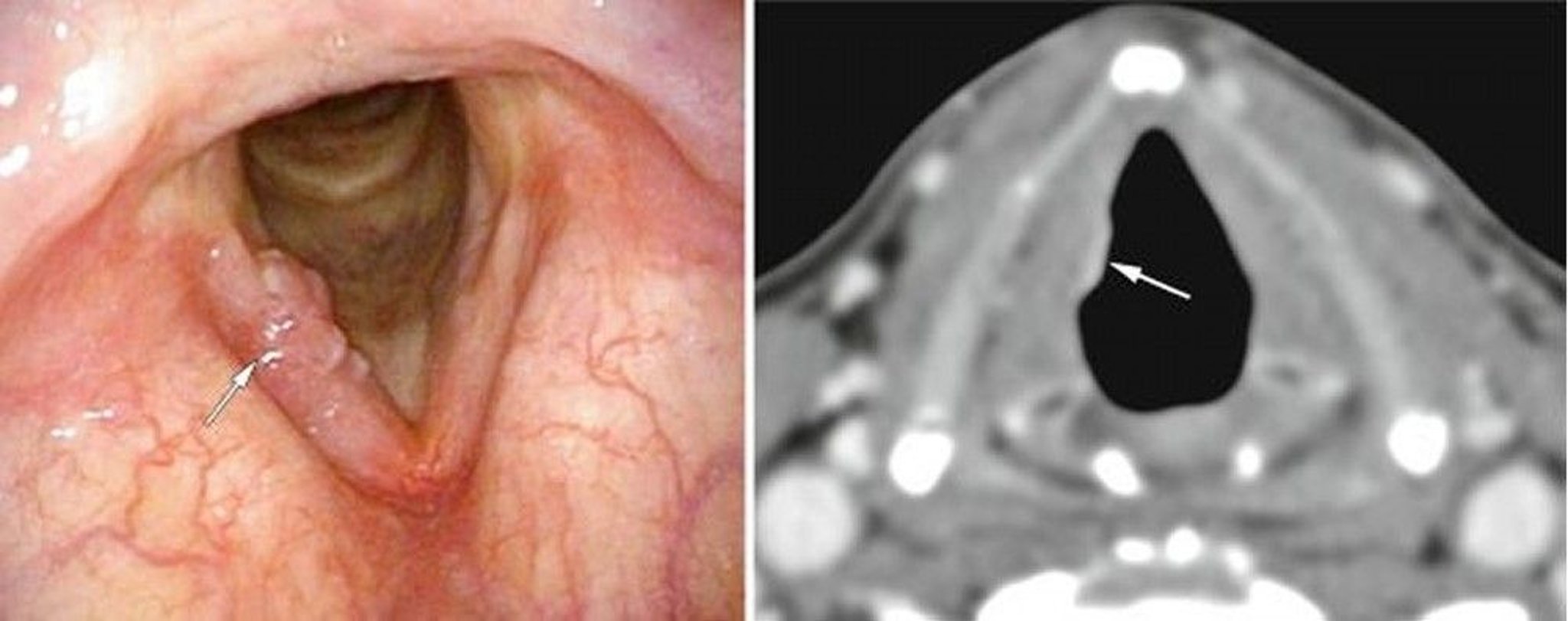
This patient had an early glottic laryngeal cancer, here visible on one vocal cord on endoscopy (left image, white arrow) as excrescences, and on CT (right image, white arrow) as an abnormal soft tissue density.
© Springer Science+Business Media
Patients with confirmed carcinoma typically have neck CT with contrast and a chest radiograph or chest CT. Most clinicians also do PET of the neck and chest at the time of diagnosis.
Diagnosis reference
1. de Vries N, Snow GB. Multiple primary tumours in laryngeal cancer. J Laryngol Otol 1986;100(8):915-918. doi:10.1017/s0022215100100313
Staging of Laryngeal Cancer
For purposes of clinical stage classification, the larynx is divided into 3 regions: supraglottis, glottis, and subglottis (1). Laryngeal cancer is staged according to size and site of the primary tumor (T), number and size of metastases to the cervical lymph nodes (N), and evidence of distant metastases (M). There are separate N categories for HPV-related and HPV-unrelated cancers. Staging usually requires imaging with CT, MRI, or both, and often PET.
Clinical staging (cTNM) is based on the results of the physical examination and tests done before surgery. Pathologic staging (pTNM) is based on the pathologic characteristics of the primary tumor and the number of positive nodes found during surgery.
Extranodal extension is incorporated into the "N" category for metastatic cancer to neck nodes. Clinical diagnosis of extranodal extension is based on finding evidence of gross extranodal extension during the physical examination together with imaging tests confirming the finding. Pathologic extranodal extension is defined as histologic evidence of tumor in a lymph node extending through the lymph node capsule into the surrounding connective tissue, with or without associated stromal reaction.
Staging reference
1. Amin MB, Edge S, Greene F, Byrd DR, et al: American Joint Committee on Cancer (AJCC) Cancer Staging Manual, 8th edition. New York, Springer, 2017; AJCC Cancer Staging Form Supplement, 2018.
Treatment of Laryngeal Cancer
Early-stage (T1 and T2): Surgery or radiation therapy
Moderately advanced (T3): Radiation therapy and sometimes chemotherapy
Advanced (T4): Surgery (often followed by radiation therapy and sometimes chemotherapy) or sometimes chemotherapy and radiation therapy
The approach to treatment varies by anatomic location (ie, supraglottis, glottis, subglottis) and stage (1).
Supraglottic cancer
Early supraglottic carcinoma can be effectively treated with radiation therapy or partial laryngectomy. Laser resection has shown considerable success on early-stage supraglottic squamous cell carcinomas and minimizes functional changes after surgery. If the carcinoma is more advanced but does not affect the true vocal cords, a supraglottic partial laryngectomy can be done to preserve the voice and glottic sphincter. If the true vocal cords also are affected, a supracricoid laryngectomy or a total laryngectomy is required if surgery is chosen.
Most advanced-stage supraglottic cancers initially are treated with chemotherapy and radiation therapy. The supraglottis has a rich lymphatic network, so in all patients with supraglottic cancer, the neck must be treated with surgery, radiation, or both.
Glottic cancer
Early-stage glottic carcinoma is treated with laser excision, radiation therapy, or occasionally open laryngeal surgery. Endoscopic laser resection and radiation therapy usually preserve a normal voice and post-treatment function and have similar cure rates. Whether surgery or radiation is used to treat early-stage glottic cancer usually depends on the location of the lesion in the glottis, the preferences of the patient and the treating institution.
For moderately advanced glottic carcinoma, defined by a lack of vocal cord mobility or extension into the tongue, most patients are treated with both chemotherapy and radiation therapy. If the patient presents with extension outside of the larynx or with cartilage invasion, a laryngectomy provides the best oncologic results; the laryngectomy is commonly total, but endoscopic laser resection or open partial laryngectomy can be used in selected cases. A total laryngectomy is also commonly used for salvage situations; however, endoscopic resection or open partial laryngectomy may sometimes be used in these situations.
Subglottic cancer
Early subglottic carcinoma is rarely treatable with endoscopic resection so radiation is the mainstay of treatment. For more advanced subglottic lesions or lesions with metastasis, chemoradiation is the standard of care unless there is extension outside of the larynx or extensive cartilage invasion in which case total laryngectomy provides the best outcome.
Rehabilitation
Rehabilitation may be required after either surgical or nonsurgical treatment. Significant swallowing problems are common after chemotherapy and radiation therapy and may require esophageal dilation, swallowing therapy, or, in severe cases, surgical replacement of the pharynx or gastrostomy tube feedings. Swallowing also is affected by surgery and may require swallowing therapy or dilation as well.
Speech, on the other hand, is more significantly affected by surgery. After total laryngectomy, the patient requires creation of a new voice by way of
Esophageal speech
A tracheoesophageal puncture
An electrolarynx
In all 3 techniques, sound is articulated into speech by the pharynx, palate, tongue, teeth, and lips.
Esophageal speech involves taking air into the esophagus during inspiration and gradually eructating the air through the pharyngoesophageal junction to produce a sound.
A tracheoesophageal puncture involves placement of a one-way valve between the trachea and esophagus to facilitate phonation. This valve forces air into the esophagus during expiration to produce a sound. Patients receive physical rehabilitation, speech therapy, and appropriate training in the maintenance and use of this valve and must be cautioned against the possible aspiration of food, fluids, and secretions.
An electrolarynx is a battery-powered sound source that is held against the neck to produce sound. Although it carries a great deal of social stigma for many patients, it has the advantage of being functional immediately with little or no training.
Treatment reference
1. National Cancer Institute: Laryngeal Cancer Treatment (PDQ®)–Health Professional Version. Updated February 2024
Prognosis for Laryngeal Cancer
The overall relative 5-year survival rate for patients with laryngeal cancer is 61% (1). Early-stage glottic carcinoma has an 85 to 95% 5-year survival rate (2). Patients who present with regional nodal disease have a 48% relative 5-year survival rate, and those who present with distant metastases have a 34% relative 5-year survival rate (2).
Prognosis references
1. National Cancer Institute: Surveillance, Epidemiology, and End Results Program: Cancer Stat Facts: Laryngeal Cancer. Laryngeal Cancer — Cancer Stat Facts Accessed July 30, 2024.
2. Chen JJ, Stessin A, Christos P, et al: Differences in survival outcome between stage I and stage II glottic cancer: A SEER-based analysis. Laryngoscope 125(9):2093-2098, 2015. doi:10.1002/lary.25338
Key Points
Hoarseness is common early in glottic cancers but is a late symptom for supraglottic and subglottic cancers.
All patients who have hoarseness for > 2 to 3 weeks should have their larynx examined by a head and neck specialist.
Patients with confirmed carcinoma typically have neck CT with contrast and often PET/CT for advanced stages.
Treat early-stage (T1 and T2) supraglottic, glottic, and subglottic cancer with surgery or radiation therapy.
Treat moderately advanced (T3) supraglottic, glottic, and subglottic cancer with radiation therapy and sometimes chemotherapy.
Treat most advanced (T4) supraglottic, glottic, and subglottic cancer that extends outside of the larynx with surgery and then postoperative chemotherapy and radiation therapy.
Some minimally invasive T4 cancers can be considered for primary treatment with chemotherapy and radiation.





