

Familial adenomatous polyposis is a hereditary disorder causing numerous colonic polyps and frequently results in colon carcinoma, often by age 40. Patients are usually asymptomatic but may have heme-positive stool. Diagnosis is by endoscopy and genetic testing. Treatment is colectomy.
Familial adenomatous polyposis is an autosomal dominant disease in which ≥ 100 adenomatous polyps carpet the colon and rectum.
The disorder occurs in approximately 1 in 10,000 people (1). Polyps are present in 50% of patients by age 15 years, and 95% by age 35 years. Cancer develops before age 40 in nearly all untreated patients.
Patients also can develop various extracolonic manifestations (previously termed Gardner syndrome), both benign and malignant. Benign manifestations include desmoid tumors, osteomas of the skull or mandible, sebaceous cysts, and adenomas in other parts of the gastrointestinal tract. Patients are at increased risk of cancer in the duodenum (5 to 11%), pancreas (2%), thyroid (2%), brain (medulloblastoma in < 1%), and liver (hepatoblastoma in 0.7% of children < 5 years) (2).
References
1. Yang J, Gurudu SR, Koptiuch C, et al. American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in familial adenomatous polyposis syndromes. Gastrointest Endosc. 2020 May;91(5):963-982.e2. doi: 10.1016/j.gie.2020.01.028
2. Boardman LA, Vilar E, You YN, Samadder J. AGA Clinical Practice Update on Young Adult-Onset Colorectal Cancer Diagnosis and Management: Expert Review. Clin Gastroenterol Hepatol. 2020 Oct;18(11):2415-2424. doi: 10.1016/j.cgh.2020.05.058
Symptoms and Signs of Familial Adenomatous Polyposis
Many patients are asymptomatic, but rectal bleeding, typically occult, occurs.
Diagnosis of Familial Adenomatous Polyposis
Colonoscopy
Genetic testing of patient and first-degree relatives
Offspring screened for hepatoblastoma
Diagnosis of familial adenomatous polyposis is made by finding > 100 polyps on colonoscopy (1). Patients with 10 to 99 synchronous adenomas have oligopolyposis or attenuated FAP (AFAP). AFAP is defined by <100 adenomas at presentation inherited in an autosomal-dominant pattern (2). Although the characteristic lesions of familial adenomatous polyposis can be recognized on sigmoidoscopy, colonoscopy is usually done to detect a more proximal cancer, which would require evaluation for metastases before treatment.
Diagnosed patients should have genetic testing to identify the specific mutation, which should then be sought in first-degree relatives (2, 3). If genetic testing is unavailable, relatives should be screened with annual sigmoidoscopy beginning at age 10-12, reducing frequency with each decade. If no polyps are evident by age 50, screening frequency is then the same as for average-risk patients (2). In AFAP, colonoscopy can be deferred until the late teens or early 20's with examinations every 1-2 years. Colonoscopy is highly recommended given the more proximal distribution of polyps in this form of FAP (2).
Diagnosis references
1. Yang J, Gurudu SR, Koptiuch C, et al. American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in familial adenomatous polyposis syndromes. Gastrointest Endosc. 2020 May;91(5):963-982.e2. doi: 10.1016/j.gie.2020.01.028
2. Syngal S, Brand RE, Church JM,et al; American College of Gastroenterology. ACG clinical guideline. Genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 2015 Feb;110(2):223-62; quiz 263. doi: 10.1038/ajg.2014.435
3. Heald B, Hampel H, Church J, et al; Collaborative Group of the Americas on Inherited Gastrointestinal Cancer. Collaborative Group of the Americas on Inherited Gastrointestinal Cancer Position statement on multigene panel testing for patients with colorectal cancer and/or polyposis. Fam Cancer. 2020 Jul;19(3):223-239. doi: 10.1007/s10689-020-00170-9
Treatment of Familial Adenomatous Polyposis
Colectomy
Endoscopic surveillance of remainder of gastrointestinal tract
Perhaps nonsteroidal anti-inflammatory drugs (NSAIDs)
Colectomy should be done soon after diagnosis. Total proctocolectomy eliminates the risk of colon and rectal cancer. The most commonly used reconstruction options are ileal pouch-anal anastomosis (IPAA) and permanent ileostomy. If subtotal colectomy (removal of most of the colon, leaving the rectum) with ileorectal anastomosis is done, the rectal remnant must be inspected frequently; new polyps must be excised or fulgurated. NSAIDs may inhibit new polyp formation. If new ones appear too rapidly or prolifically to remove, excision of the rectum is needed.

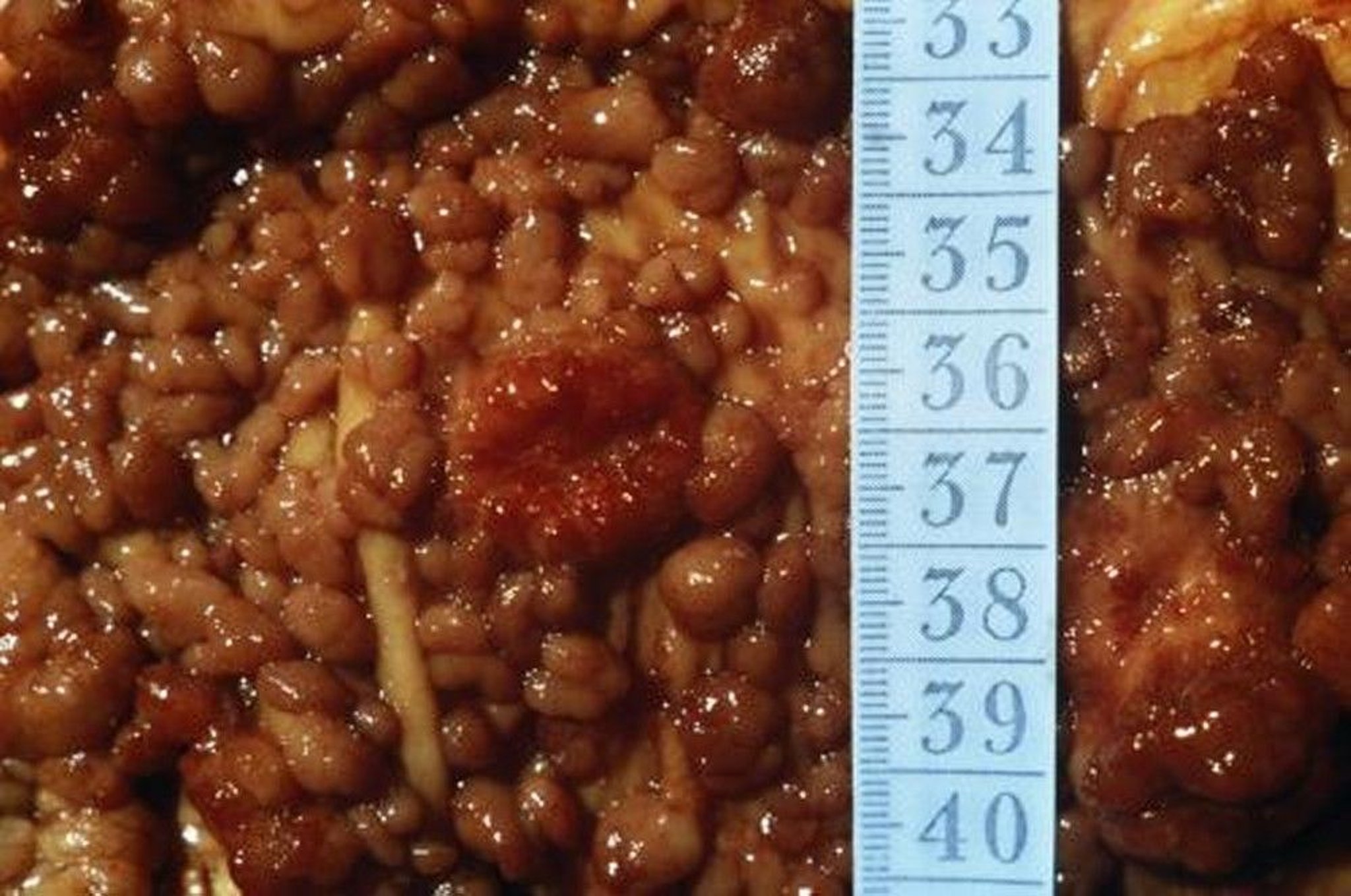
This photo shows a colectomy specimen with numerous polyps in the colon.
CNRI/SCIENCE PHOTO LIBRARY
After colectomy, patients should have upper endoscopic surveillance at periodic intervals. The American College of Gastroenterology recommends performing upper endoscopy including duodenoscopy starting at age 25 to 30 years and repeating surveillance every 6 months to 4 years depending on the stage of duodenal polyposis (1). The Spigelman classification is used to determine the degree of polyposis based on 4 variables (number of polyps, polyp size, histology, and dysplasia) and the calculated score provides a recommended surveillance interval (2). Annual screening of the thyroid with ultrasound also is recommended.
Treatment references
1. Syngal S, Brand RE, Church JM, et al. ACG clinical guideline: Genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 2015;110(2):223-263. doi:10.1038/ajg.2014.435
2. Saurin JC, Gutknecht C, Napoleon B, et al. Surveillance of duodenal adenomas in familial adenomatous polyposis reveals high cumulative risk of advanced disease. J Clin Oncol. 22(3):493–498, 2004. doi: 10.1200/JCO.2004.06.028
Key Points
Familial adenomatous polyposis is an autosomal dominant disease in which ≥ 100 adenomatous polyps carpet the colon and rectum.
Nearly all patients develop colon carcinoma by age 40, so total proctocolectomy is usually done soon after diagnosis.
Patients have an increased risk of other cancers, particularly of the duodenum, and also the pancreas, thyroid, brain, and liver.
After treatment, patients are screened regularly for other cancers and development of polyps in the upper gastrointestinal tract.
Children of parents with familial adenomatous polyposis may be screened for hepatoblastoma from birth to age 5 years.





