

Acute tubular necrosis (ATN) is kidney injury characterized by acute tubular cell injury and dysfunction. Common causes are hypotension or sepsis that causes renal hypoperfusion and nephrotoxic medications. The condition is asymptomatic unless it causes renal failure. The diagnosis is suspected when azotemia develops after a hypotensive event, severe sepsis, or medication exposure and is distinguished from prerenal azotemia by laboratory testing and response to volume expansion. Treatment is supportive.
(See also Overview of Tubulointerstitial Diseases.)

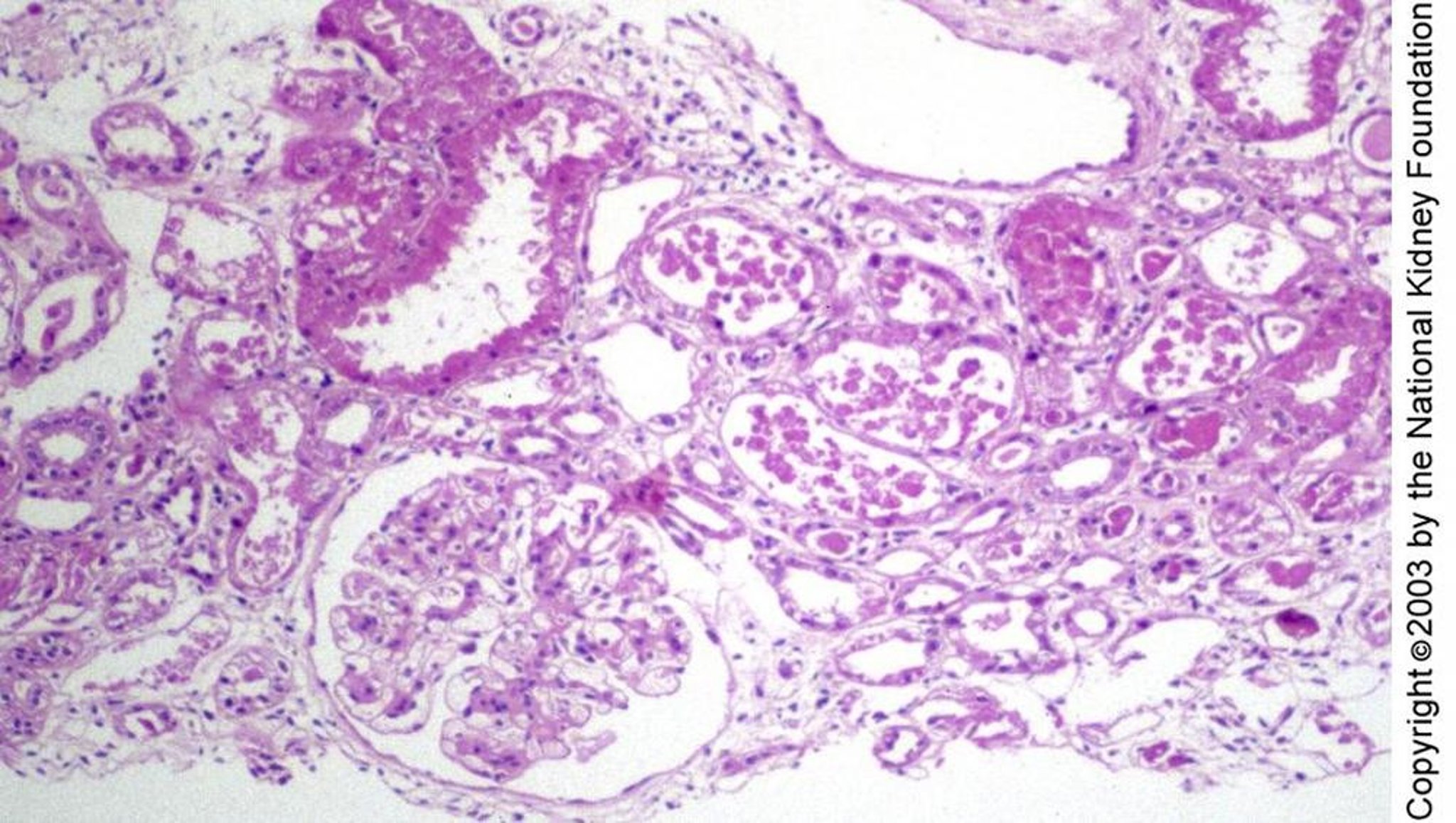
Tubular injury in acute tubular necrosis may be manifest histologically as regenerating flattened tubular epithelium without necrosis, as seen to the right of the glomerulus, blebbing and individual cell degeneration, as in the top left, or frank necrosis, as in the middle of the image (periodic acid-Schiff stain, ×100).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Etiology of Acute Tubular Necrosis
Common causes of acute tubular necrosis include the following:
Renal hypoperfusion, most often caused by hypotension or sepsis (ischemic ATN; most common, especially in patients in an intensive care unit)
Nephrotoxins
Major surgery (often due to multiple factors)
Other causes of ATN include
Third-degree burns covering > 15% of body surface area
The heme pigments myoglobin and hemoglobin (caused by either rhabdomyolysis or massive hemolysis)
Other endogenous toxins, resulting from disorders such as tumor lysis or multiple myeloma
Poisons, such as ethylene glycol
Herbal and folk remedies, such as ingestion of fish gallbladder in Southeast Asia
Common nephrotoxins include the following:
Aminoglycosides
Amphotericin BAmphotericin B
Cisplatin and other chemotherapy agentsCisplatin and other chemotherapy agents
Radiocontrast (particularly ionic high osmolar agents given IV in volumes > 100 mL—see Contrast Nephropathy)
Nonsteroidal anti-inflammatory drugs (NSAIDs; especially when concurrent with poor renal perfusion or other nephrotoxic agents)
Colistimethate (colistin)
Calcineurin inhibitors (eg, cyclosporine, tacrolimus, used systemically)Calcineurin inhibitors (eg, cyclosporine, tacrolimus, used systemically)
Vancomycin (particularly with supratherapeutic dosing [Vancomycin (particularly with supratherapeutic dosing [1])
Massive volume loss, particularly in patients with septic or hemorrhagic shock, pancreatitis, or major surgery, increases the risk of ischemic ATN; patients with serious comorbidities are at highest risk.
Major surgery and advanced hepatobiliary disease (2) increase the risk of aminoglycoside toxicity. Certain combinations of medications (eg, aminoglycosides with amphotericin B) may be especially nephrotoxic. NSAIDs may cause several types of intrinsic kidney disease, including ATN. ) increase the risk of aminoglycoside toxicity. Certain combinations of medications (eg, aminoglycosides with amphotericin B) may be especially nephrotoxic. NSAIDs may cause several types of intrinsic kidney disease, including ATN.
Toxic exposures cause patchy, segmental, tubular luminal occlusion with casts and cellular debris or segmental tubular necrosis.
Acute tubular necrosis is more likely to develop in patients with the following:
Preexisting chronic kidney disease
Preexisting hypovolemia or poor renal perfusion
Older age
Etiology references
1. Stokes MB: Vancomycin in the kidney—A novel cast nephropathy. : Vancomycin in the kidney—A novel cast nephropathy.J Am Soc Nephrol 28(6):1669-1670, 2017. doi: 10.1681/ASN.2017010091
2. Aniort J, Poyet A, Kemeny J-L, et al: Bile cast nephropathy caused by obstructive cholestasis. Am J Kidney Dis 69(1):143-146, 2017. doi: 10.1053/j.ajkd.2016.08.023
Symptoms and Signs of Acute Tubular Necrosis
Acute tubular necrosis is usually asymptomatic but may cause symptoms or signs of acute kidney injury, typically oliguria initially, if ATN is severe. However, urine output may not be reduced if ATN is less severe (eg, typical in aminoglycoside-induced ATN).
Diagnosis of Acute Tubular Necrosis
Differentiation from prerenal azotemia, based mainly on laboratory findings and, in the case of blood or fluid loss, response to volume expansion
Acute tubular necrosis is suspected when serum creatinine rises ≥ 0.3 mg/dL/day (26.5 micromol/liter [μmol/L]) above baseline or a 1.5- to 2.0-fold increase in serum creatinine from baseline after an apparent trigger (eg, hypotensive event, exposure to a nephrotoxin); the rise in creatinine may occur 1 to 2 days after certain exposures (eg, IV radiocontrast) but be more delayed after exposure to other nephrotoxins (eg, aminoglycosides).
ATN must be differentiated from prerenal azotemia because treatment differs. In prerenal azotemia, renal perfusion is decreased enough to elevate serum blood urea nitrogen (BUN) out of proportion to creatinine, but not enough to cause ischemic damage to tubular cells. Prerenal azotemia can be caused by direct intravascular fluid loss (eg, due to hemorrhage, gastrointestinal tract losses, urinary losses) or by a relative decrease in effective circulating volume ATN must be differentiated from prerenal azotemia because treatment differs. In prerenal azotemia, renal perfusion is decreased enough to elevate serum blood urea nitrogen (BUN) out of proportion to creatinine, but not enough to cause ischemic damage to tubular cells. Prerenal azotemia can be caused by direct intravascular fluid loss (eg, due to hemorrhage, gastrointestinal tract losses, urinary losses) or by a relative decrease in effective circulating volumewithout loss of total body fluid (eg, in heart failure, portal hypertension with ascites). If fluid loss is the cause, volume expansion using IV normal saline solution increases urine output and normalizes serum creatinine level. If ATN is the cause, IV saline typically causes no increase in urine output and no rapid change in serum creatinine. Untreated prerenal azotemia may progress to ischemic ATN.
Laboratory findings also help distinguish acute tubular necrosis from prerenal azotemia (see table ).
Laboratory Findings Distinguishing Acute Tubular Necrosis From Prerenal Azotemia
Test* | Acute Tubular Necrosis | Prerenal Azotemia |
|---|---|---|
Rate of creatinine rise | 0.3–0.5 mg/dL/day (26.5–44.2 micromol/L) | Variable and fluctuates |
BUN/creatinine ratio | 10–15:1 | > 20:1 |
Urine osmolality (in mOsm/kg or mmol/kg) | < 450 (usually < 350) | > 500 |
Urine specific gravity | ≤ 1.010 | >1.020 |
Urine sodium (in mEq/L or mmol/L) | > 40 | < 20 |
Urine/plasma creatinine ratio | < 20 | > 40 |
Fractional excretion of sodium (%) | > 2 | < 1 |
Urinary sediment | Muddy brown granular casts, epithelial cell casts, free epithelial cells, or a combination | Normal or with hyaline casts |
* Criteria may not apply in patients with chronic kidney disease or recent diuretic use. BUN = blood urea nitrogen. blood urea nitrogen. | ||

Treatment of Acute Tubular Necrosis
Supportive care
Treatment is supportive and includes stopping nephrotoxins whenever possible, maintaining euvolemia, providing nutritional support, and treating infections (preferably with medications that are not nephrotoxic). Diuretics may be used to maintain urine output in oliguric acute tubular necrosis but are of unproven benefit and do not alter the course of kidney injury; there is no evidence to support use of mannitol or dopamine. General Treatment is supportive and includes stopping nephrotoxins whenever possible, maintaining euvolemia, providing nutritional support, and treating infections (preferably with medications that are not nephrotoxic). Diuretics may be used to maintain urine output in oliguric acute tubular necrosis but are of unproven benefit and do not alter the course of kidney injury; there is no evidence to support use of mannitol or dopamine. Generalmanagement of acute kidney injury is discussed elsewhere.
Pearls & Pitfalls
|
Prognosis for Acute Tubular Necrosis
In otherwise healthy patients, short-term prognosis is good when the underlying insult is corrected; serum creatinine typically returns to normal or near-normal within 1 to 3 weeks. In hospitalized patients, even when acute kidney injury is mild, morbidity and mortality are increased (1). Prognosis is better in patients who do not require treatment in an intensive care unit than in those who do. Predictors of mortality include mainly (1)
Decreased urine volume (eg, anuria, oliguria)
Severity of the underlying disorder
Severity of coexisting disorders
Patients who survive acute tubular necrosis have an increased risk of chronic kidney disease.
Cause of death is usually infection or the underlying disorder.
Prognosis reference
1. Chertow GM, Burdick E, Honour M, et al: Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol 16(11):3365-3370, 2005. doi: 10.1681/ASN.2004090740
Prevention of Acute Tubular Necrosis
Prevention includes the following:
Maintaining euvolemia and renal perfusion in critically ill patients
Avoiding nephrotoxic medications when possible
Closely monitoring renal function when nephrotoxic medications must be used
Taking measures to prevent contrast nephropathy
Among patients with diabetes, controlling blood glucose levels
There is no evidence that loop diuretics, mannitol, or dopamine helps prevent or alter the course of established acute tubular necrosis. There is no evidence that loop diuretics, mannitol, or dopamine helps prevent or alter the course of established acute tubular necrosis.
Key Points
Acute tubular necrosis (ATN) can develop after various disorders or triggers decrease renal perfusion or expose the kidneys to toxins.
Other than oliguria in severe cases, symptoms do not develop unless and until renal failure develops.
Differentiate ATN from prerenal azotemia by the response to volume expansion and by urine and blood chemistry tests and calculations derived from them.
Correct the cause of ATN as soon as possible to achieve a good short-term prognosis.
Stop nephrotoxins, maintain euvolemia, and treat infection and undernutrition.
Drug Information for the Topic





