

Scrub typhus is a zoonotic disease caused by Orientia tsutsugamushi; mites are the reservoir and vector and transmit infection to various hosts, including rodents, other small animals, and humans. Symptoms are fever, a primary lesion, a macular rash, and lymphadenopathy. Diagnosis is by serology, polymerase chain reaction testing, and immunohistochemistry. Treatment is with doxycycline.; mites are the reservoir and vector and transmit infection to various hosts, including rodents, other small animals, and humans. Symptoms are fever, a primary lesion, a macular rash, and lymphadenopathy. Diagnosis is by serology, polymerase chain reaction testing, and immunohistochemistry. Treatment is with doxycycline.
Scrub typhus is a zoonosis related to rickettsial diseases.
O. tsutsugamushi is transmitted by the bites of trombiculid mite larvae (chiggers), which are the primary natural reservoir and vector. Chiggers feed on forest and rural rodents, including rats, voles, and field mice, but these animals are considered secondary (or maintaining) hosts (1). Similarly, human infection can occur after a chigger bite. Humans are accidental dead-end hosts. Human contact with infected animals cannot directly transmit infection.


PDC/SCIENCE PHOTO LIBRARY
Risk factors for scrub typhus include agricultural work, exposure to certain types of vegetation, outdoor activities in rural areas, and proximity to rodents or other farm animals (2).
Historically, scrub typhus was considered to be endemic across South Asia, East Asia, and Southeast Asia (the Tsutsugamushi triangle), with over 1 billion people at risk. Incidence is an estimated 1 million clinical cases annually (3). The identification of cases from the Arabian Peninsula, Chile, and Kenya suggests a wider global distribution in regions with warmer climates (4).
Scrub typhus is rare in the United States and is not a nationally notifiable disease (5).
General references
1. Weitzel T, Dittrich S, López J, et al. Endemic Scrub Typhus in South America. N Engl J Med. 2016;375(10):954-961. doi:10.1056/NEJMoa1603657
2. Wang Q, Ma T, Ding F, et al. Global and regional seroprevalence, incidence, mortality of, and risk factors for scrub typhus: A systematic review and meta-analysis. Int J Infect Dis. 2024;146:107151. doi:10.1016/j.ijid.2024.107151
3. Xu G, Walker DH, Jupiter D, Melby PC, Arcari CM. A review of the global epidemiology of scrub typhus. PLoS Negl Trop Dis. 2017;11(11):e0006062. Published 2017 Nov 3. doi:10.1371/journal.pntd.0006062
4. Bonell A, Lubell Y, Newton PN, Crump JA, Paris DH. Estimating the burden of scrub typhus: A systematic review. PLoS Negl Trop Dis. 2017;11(9):e0005838. Published 2017 Sep 25. doi:10.1371/journal.pntd.0005838
5. CDC. Information for Public Health Officials. December 11, 2025. Accessed January 9, 2026.
Symptoms and Signs of Scrub Typhus
After an incubation period of approximately ≥ 7 days (symptoms usually occur within 7 to 10 days and last 14 to 21 days) (1), symptoms of scrub typhus start suddenly and include fever, chills, headache, and generalized lymphadenopathy.


This photo shows a person's skin 24 hours after being bitten by a chigger (mite larvae). Note the vesicle at the bite site was caused by the bite of a larval harvest mite of the genus Trombicula.
CDC
At the onset of fever, an eschar often develops at the site of the chigger bite. The typical lesion begins as an erythematous, indurated lesion about 1 cm in diameter; it eventually vesiculates, ruptures, and becomes covered with a black scab. Whether different strains of O. tsutsugamushi can cause an eschar varies, and an eschar is easier to detect in people with light skin. A macular rash develops on the trunk during days 5 to 8 of fever in 25 to 50% of patients, often extending to the arms and legs (1). It may disappear rapidly or become maculopapular and intensely colored. Regional lymph nodes enlarge.


This photo shows a scrub typhus eschar on a person's leg.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Fever rises during the first week, often to 40 to 40.5° C. Headache is severe and common, as is conjunctival injection. Cough is present during the first week of fever, and pneumonitis may develop during the second week.
In severe cases, pulse rate increases; blood pressure drops; and delirium, stupor, and muscular twitching develop. Splenomegaly may be present, and interstitial myocarditis is more common than in other rickettsial diseases. In untreated patients, high fever may persist ≥ 2 weeks, then falls gradually over several days. With therapy, defervescence usually begins within 36 hours. Recovery is prompt and uneventful.

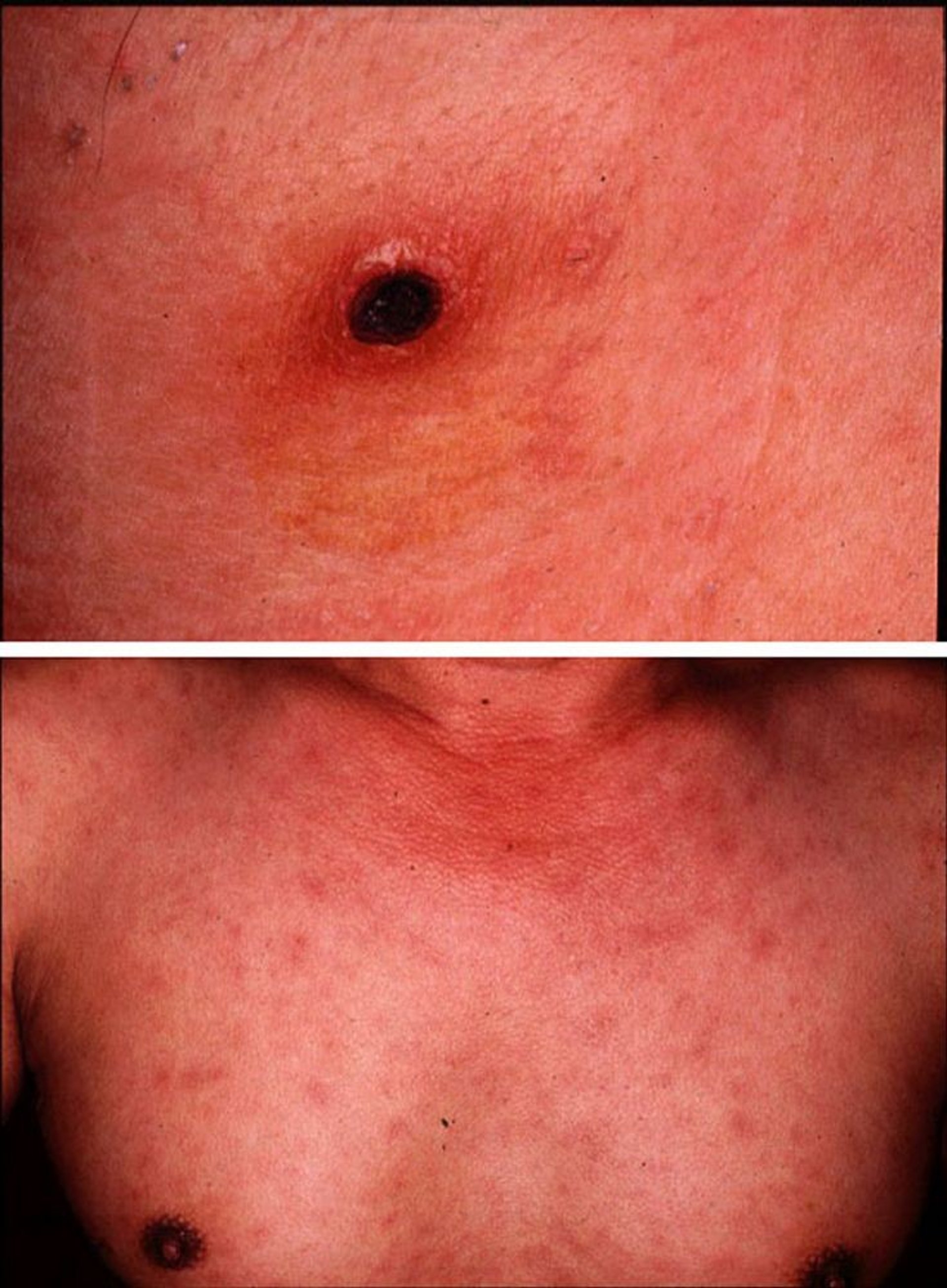
Scrub typhus (tsutsugamushi disease) manifests as an eschar at the site of a chigger bite (top). A diffuse macular rash follows the appearance of the eschar (bottom).
Images courtesy of Yoshiki Taniguchi, MD. From Taniguchi, Y: Eschar, fever, and rash in a 43-year-old man. Dermatology Online Journal 3(2), 1997.
Symptoms and signs reference
1. CDC. Clinical Overview of Scrub Typhus. May 15, 2024. Accessed January 9, 2026.
Diagnosis of Scrub Typhus
History and physical examination
Molecular diagnostic testing (polymerase chain reaction [PCR]) of infected tissue or blood specimens
Biopsy of tissue with immunohistochemistry to detect organisms
Acute and convalescent serologic testing (serologic testing not useful acutely)
The diagnosis of scrub typhus relies on timely identification of clinical signs such as fever, rash, and eschar with satellite lymphadenopathy in the appropriate epidemiologic context. Manifestations of scrub typhus are similar to those of Rocky Mountain spotted fever and epidemic typhus. However, scrub typhus usually occurs in different geographic areas.
Laboratory confirmation is primarily through indirect immunofluorescence assay serology showing increased titers between acute and convalescent samples (1). Weil-Felix OX-K agglutination assays are not recommended because of low sensitivity and specificity (1).
PCR testing on skin biopsies or an eschar swab may allow earlier diagnosis, and immunohistochemistry on formalin-fixed tissue biopsy is an adjunctive method.
Because scrub typhus is not common in the United States, serologic and molecular assays are not typically available at regional health departments but may be performed at the United States Centers for Disease Control and Prevention (CDC).
For further details, see Diagnosis of Rickettsial and Related Infections.
Diagnosis reference
1. CDC. Clinical Overview of Scrub Typhus. May 15, 2024. Accessed January 9, 2026.
Treatment of Scrub Typhus
DoxycyclineDoxycycline
Sometimes other tetracyclines or azithromycinSometimes other tetracyclines or azithromycin
Antibiotics are most effective if given soon after symptoms begin.
Doxycycline is the first-line treatment of scrub typhus. This medication is administered until the patient improves, has been afebrile for 48 hours, and has received treatment for at least 7 days. Doxycycline is the first-line treatment of scrub typhus. This medication is administered until the patient improves, has been afebrile for 48 hours, and has received treatment for at least 7 days.
For patients who are pregnant or who have severe doxycycline allergy, azithromycin has been shown to be a safe and effective alternative to allergy, azithromycin has been shown to be a safe and effective alternative todoxycycline (1).
In patients who are not pregnant, azithromycin and other tetracyclines may be alternatives to In patients who are not pregnant, azithromycin and other tetracyclines may be alternatives todoxycycline; however, the certainty of evidence is low (2).
Chloramphenicol is also an alternative treatment. Chloramphenicol is also an alternative treatment.Chloramphenicol can cause adverse hematologic effects, which require monitoring of blood indices, and, in neonates, gray baby syndrome.
Although some tetracyclines can cause tooth staining in children < 8 years of age, the United States Centers for Disease Control and Prevention (CDC) advises that a course of doxycycline is warranted (Although some tetracyclines can cause tooth staining in children doxycycline is warranted (3), given for 5 days for mild illness and for 10 days for high-risk children. Research indicates that short courses of doxycycline (5 to 10 days, as used for rickettsial disease) can be used in children without causing tooth staining or weakening of tooth enamel (4).
Treatment references
1. Lee SC, Cheng YJ, Lin CH, et al. Comparative effectiveness of azithromycin for treating scrub typhus: A PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore). 2017;96(36):e7992. doi:10.1097/MD.0000000000007992
2. El Sayed I, Liu Q, Wee I, Hine P. Antibiotics for treating scrub typhus. Cochrane Database Syst Rev. 2018;9(9):CD002150. Published 2018 Sep 24. doi:10.1002/14651858.CD002150.pub2
3. CDC. Clinical Overview of Scrub Typhus. May 15, 2024. Accessed January 9, 2026.
4. CDC. Research: Doxycycline and Tooth Staining. May 15, 2024. Accessed January 2, 2026.
Prevention of Scrub Typhus
Eliminating or decreasing mite populations by clearing brush and spraying infested areas with residual insecticides helps prevent scrub typhus.
Insect repellents (eg, diethyltoluamide [DEET], picaridin, IR3535, oil of Lemon eucalyptus (OLE), para-menthane-diol (PMD), or 2-undecanone) should be used on skin surfaces when exposure is likely.Insect repellents (eg, diethyltoluamide [DEET], picaridin, IR3535, oil of Lemon eucalyptus (OLE), para-menthane-diol (PMD), or 2-undecanone) should be used on skin surfaces when exposure is likely.
Key Points
Scrub typhus is transmitted by the bites of mite larvae (chiggers).
Fever (often accompanied by an eschar at the bite site), chills, severe headache, and generalized lymphadenopathy start suddenly; a rash develops and spreads.
Diagnosis is by serology, PCR testing, and immunohistochemistry.
Treatment is with doxycycline, which results in rapid improvement even in severe cases; azithromycin is an alternative in pregnant patients or in patients with Treatment is with doxycycline, which results in rapid improvement even in severe cases; azithromycin is an alternative in pregnant patients or in patients withdoxycycline allergy.
Drug Information for the Topic





