

Clavicle fractures are among the most common fractures, particularly among children. Diagnosis is by radiographs. Most types are treated with a sling.
(See also Overview of Fractures.)
Etiology of Clavicle Fractures
Clavicle fractures usually result from a fall on the lateral shoulder or, less often, a direct blow.
Classification
Traditionally, treatment has been based on the following classification.
Class A fractures involve the middle third of the bone and account for approximately 80% of clavicle fractures. The proximal fragment is often displaced upward because it is pulled by the sternocleidomastoid muscle. Subclavian vessels are rarely damaged.
Class B fractures involve the distal third of the bone and account for approximately 15% of clavicle fractures. They usually result from a direct blow. There are 3 subtypes:
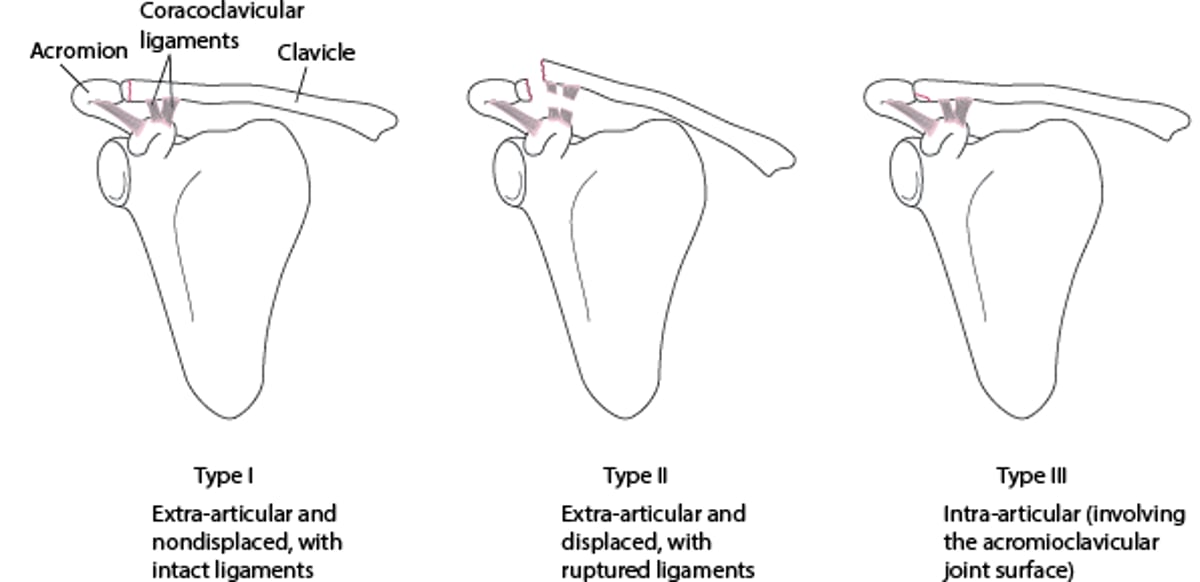
Type I: Extra-articular and nondisplaced, generally indicating a functionally intact coracoclavicular ligament (a strong and structurally important ligament)
Type II: Extra-articular and displaced, generally indicating rupture of the coracoclavicular ligament, with the proximal fragment typically displaced upward because it is pulled by the sternocleidomastoid muscle
Type III: Involving the intra-articular surface of the acromioclavicular joint, thus increasing the risk of osteoarthritis (see figure Class B Clavicular Fractures)
Class C fractures involve the proximal third of the bone and account for approximately 5% of clavicle fractures. These fractures usually result from great force and thus may be accompanied by intrathoracic injuries or sternoclavicular joint damage.
Class B Clavicular Fractures

Symptoms and Signs of Clavicle Fractures
The area over the fracture is painful, and patients may sense movement of the fracture fragments and instability. Some patients report pain in the shoulder. Arm abduction is painful.
Class A fractures and extra-articular class B fractures usually cause visible and palpable deformity. Widely displaced fractures may significantly tent the skin.
Diagnosis of Clavicle Fractures
Radiographs


This anteroposterior radiograph view shows a displaced fracture of the middle third of the clavicle (class A fracture).
Scott Camazine/SCIENCE PHOTO LIBRARY
Physical examination is often diagnostic, but anteroposterior radiograph is usually taken, and sometimes an apical lordotic view or a radiograph at a 45° angle upward is included. However, some class C and intra-articular class B fractures require other imaging studies (eg, CT).
Treatment of Clavicle Fractures
Sling
If the coracoclavicular ligament is ruptured, usually surgical repair
Many fractures are minimally displaced and can be treated with a sling for comfort for 4 to 6 weeks. Figure-of-eight braces are not recommended; clinical outcomes have not been shown to be better than when using a simple sling (1), and a simple sling is often more comfortable.
Usually, reduction is not necessary, even for greatly angulated fractures.
However, if the skin is significantly tented (usually in class A fractures), immediate consultation with an orthopedic specialist may be needed. Usually, such fractures are still successfully managed with a sling, but sometimes may require open reduction with internal fixation (ORIF) if closed reduction does not reduce skin tenting. With significant skin tenting, the bone may pierce the skin, causing an open fracture.
In class B type II fractures, the ruptured coracoclavicular ligament usually requires surgical repair by an orthopedic surgeon. For example, if patients have a distal clavicle fracture with superior displacement of the proximal fragment, they should be referred to an orthopedic surgeon for consideration of surgical repair of the coracoclavicular ligament.
For class B type III fractures, early mobilization may help decrease the risk of osteoarthritis.
Pearls & Pitfalls
|
Displaced class C fractures require reduction by an orthopedic surgeon.
Treatment reference
1. Culver A, Messick B, Burroughs K. Is a figure of eight bandage better than a simple sling for midshaft clavicle fractures in adults? Evidence-Based Practice 24(9): 41–42. doi: 10.1097/EBP.0000000000001213
Key Points
Most clavicle fractures are evident based on clinical findings.
Treat most clavicle fractures with a sling.
An orthopedic surgeon is needed to reduce displaced class C fractures and usually to surgically repair class B type II fractures.





