

A Lisfranc injury is a fracture and/or dislocation of the midfoot that disrupts one or more tarsometatarsal joints. Diagnosis is by radiographs and often CT. Treatment requires referral to an orthopedic surgeon and usually open reduction with internal fixation (ORIF) or sometimes fusion of the midfoot.
(See also Overview of Fractures.)
Lisfranc injuries are common. The usual mechanism is a direct blow or an indirect twisting force applied to a foot in plantar flexion (eg, fall on a foot in plantar flexion), as may occur in football players, motorcyclists, and horseback riders.
The Lisfranc joint complex consists of the 5 tarsometatarsal joints that connect the forefoot and midfoot. There are multiple ligaments in this complex. The Lisfranc ligament itself is the ligament that attaches the base of the 2nd metatarsal to the 1st cuneiform. Lisfranc complex injuries vary widely in severity from strains to dislocation of one or more tarsometatarsal joints with or without fracture. When fracture occurs, it often involves the 2nd metatarsal (see figure ). Lisfranc injuries often cause instability of the midfoot.
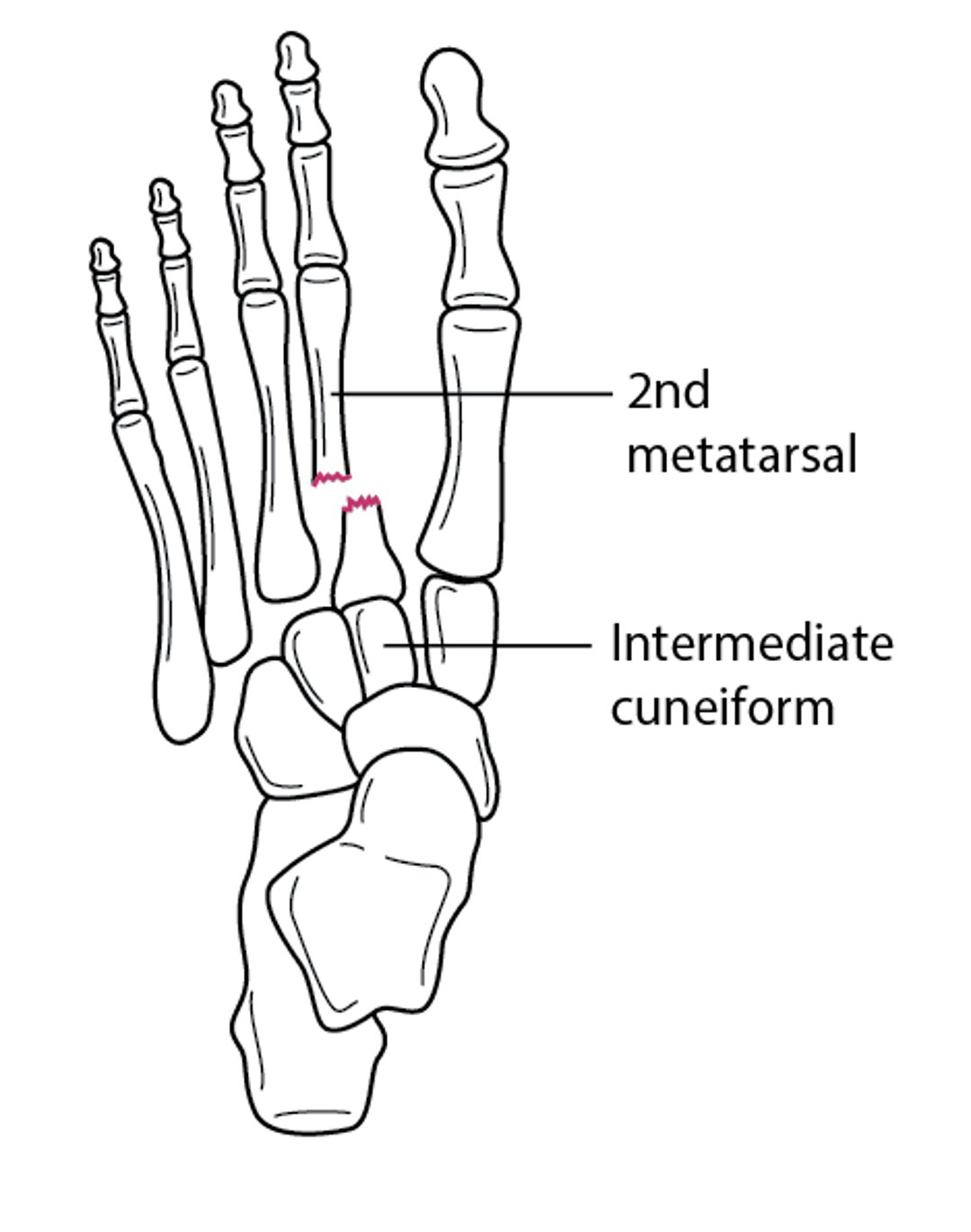
Fracture of the 2nd Metatarsal Base With Tarsometatarsal Joint Dislocation
Fracture of the 2nd metatarsal base may disrupt one or more of the tarsometatarsal joints. In this figure, the 2nd metatarsal fracture displaces the 3rd through 5th metatarsals laterally. |

Symptoms and Signs of Lisfranc Injury
Severity of Lisfranc injury varies widely. Some injuries cause only mild swelling and pain in the midfoot; others cause severe soft-tissue pain and swelling, deformity, a hematoma on the sole of the midfoot, and sometimes paresthesias. The foot may appear shortened.
Complications (eg, osteoarthritis, compartment syndrome) can be serious and chronic disability is common.
Diagnosis of Lisfranc Injury
Radiographs
Sometimes CT
Anteroposterior, lateral, and oblique radiographs of the foot are taken, but findings may be subtle, leading to misdiagnosis. Up to 20% of these fractures are missed at the initial presentation (1).
Radiographs can show a fracture at the base of the 2nd metatarsal or chip fractures of the cuneiform but may not show disruption of the tarsometatarsal joint, which should be suspected even if it is not visible on radiographs. Normally in this joint, the medial aspect of the 2nd cuneiform aligns directly with the medial aspect of the 2nd metatarsal. Comparison views or CT may be necessary to identify disruption of the joint.


This radiograph shows fractures at the base of the 2nd, 3rd, and 4th metatarsals. The tarsometatarsal joints are also disrupted.
Pearls & Pitfalls
|
If CT is not readily available, stress radiographs can be used. Radiographs are taken while the foot is under stress (eg, the patient is standing on the foot). The patient's body weight can cause the space between the 1st and 2nd metatarsals to widen, making the diagnosis much easier. However, CT is more sensitive than stress radiographs and so is preferred in equivocal cases.
Diagnosis reference
1. Singh A, Lokikere N, Saraogi A, Unnikrishnan PN, Davenport J. Missed Lisfranc injuries-surgical vs conservative treatment. Ir J Med Sci. 2021;190(2):653-656. doi:10.1007/s11845-020-02364-7
Treatment of Lisfranc Injury
Urgent orthopedic consultation
Usually, open reduction with internal fixation (ORIF) or sometimes fusion of the midfoot
Dislocations often spontaneously reduce. Nonetheless, because these injuries usually compromise foot function and cause residual pain and arthritis, patients should be immediately referred to an orthopedic specialist, usually for surgery. Typically, definitive treatment is ORIF or fusion of the midfoot.
After ORIF, CT is usually done to confirm correct alignment.
If surgery is not considered necessary, patients are immobilized, ultimately with a cast, with no weight-bearing for ≥ 6 weeks.
Key Points
Lisfranc injuries (fracture-dislocation) involve disruption of ≥ 1 ligaments that stabilize the midfoot, sometimes disrupting ≥ 1 tarsometatarsal joints.
Complications (eg, compartment syndrome, chronic pain, disability) may be serious.
Because radiograph findings may be subtle, stress radiographs or CT may be needed.
Refer patients to an orthopedic surgeon; usually, ORIF or fusion of the midfoot is required.





