

Rotator cuff injury includes tendinopathy and partial or complete tears; subacromial bursitis may result from tendinitis. Symptoms are shoulder area pain and, with severe tears, weakness. Diagnosis is by examination and, sometimes, diagnostic testing. Treatment includes nonsteroidal anti-inflammatory drugs (NSAIDs), maintenance of range of motion, and rotator cuff–strengthening exercises.
The rotator cuff, consisting of the supraspinatus, infraspinatus, teres minor, and subscapularis (SITS) muscles, together with the triceps and biceps, helps stabilize the humeral head in the glenoid fossa of the scapula during overhead arm motions (eg, pitching, swimming, weightlifting, serving in racket sports).

Etiology of Rotator Cuff Injury
Rotator cuff injury can be an acute or chronic sports injury, but it can also occur for reasons unrelated to sports activities (eg, repetitive overhead activities occurring while performing manual labor) and in people with no history of overuse or clear precipitating factor (1).
A strain of the rotator cuff is a single acute, traumatic injury to the muscles. Tendinopathy typically results from chronic impingement of the supraspinatus tendon between the humeral head and coracoacromial arch (the acromion, acromioclavicular joint, coracoid process, and coracoacromial ligament). Activities that require the arm to be moved over the head repeatedly, such as pitching in baseball, lifting heavy weights over the shoulder, serving the ball in racket sports, and swimming freestyle, butterfly, or backstroke, increase the risk.
The supraspinatus tendon is thought to be particularly susceptible because it has an undervascularized region near its insertion on the greater tuberosity. The resultant inflammatory reaction and edema further narrow the subacromial space, accelerating tendon irritation or damage. If the process is not interrupted, the resulting inflammation can lead to partial or complete tear of the rotator cuff. Degenerative rotator cuff tendinitis is common among older (> 40 years) adults who are not athletes for the same reason. Subacromial bursitis (inflammation, swelling, and fibrosis of the bursal area above the rotator cuff) commonly results from tendinitis of the cuff.
Etiology reference
1. Jain NB, Khazzam MS. Degenerative Rotator-Cuff Disorders. N Engl J Med. 2024;391(21):2027-2034. doi:10.1056/NEJMcp1909797
Symptoms and Signs of Rotator Cuff Injury
Subacromial bursitis, rotator cuff tendinopathy, and partial rotator cuff tears cause shoulder pain, especially when the arm is moved overhead. The pain usually is worse between 60° and 120° (painful arc of motion) of shoulder abduction or flexion and is usually minimal or absent at < 60° or > 120°. The pain may be described as a dull ache that is poorly localized. Complete rotator cuff tears result in acute pain and weakness of the shoulder. In larger tears of the rotator cuff, weakness of external rotation is particularly apparent.
Diagnosis of Rotator Cuff Injury
Primarily history and physical examination
Sometimes MRI or arthroscopy
Diagnosis is by history and physical examination, including provocative maneuvers (see also Physical Examination of the Shoulder). The rotator cuff cannot be palpated directly, but it can be assessed indirectly by provocative maneuvers that test its individual muscular components; significant pain or weakness is considered a positive result.
The supraspinatus is assessed by having the patient resist downward pressure on the arms held in forward flexion with the thumbs pointing downward (empty can, or Jobe test).
The infraspinatus and teres minor are assessed by having the patient resist external rotation pressure with the arms held at the sides with elbows flexed to 90°; this position isolates rotator cuff muscle function from that of other muscles such as the deltoid. Weakness during this test suggests significant rotator cuff dysfunction (eg, a complete tear).
The subscapularis is assessed by having the patient place the hand behind the back with the back of the hand resting on the lower back. The examiner lifts the hand off the lower back. The patient should be able to keep the hand off the skin of the back (Gerber lift-off test).
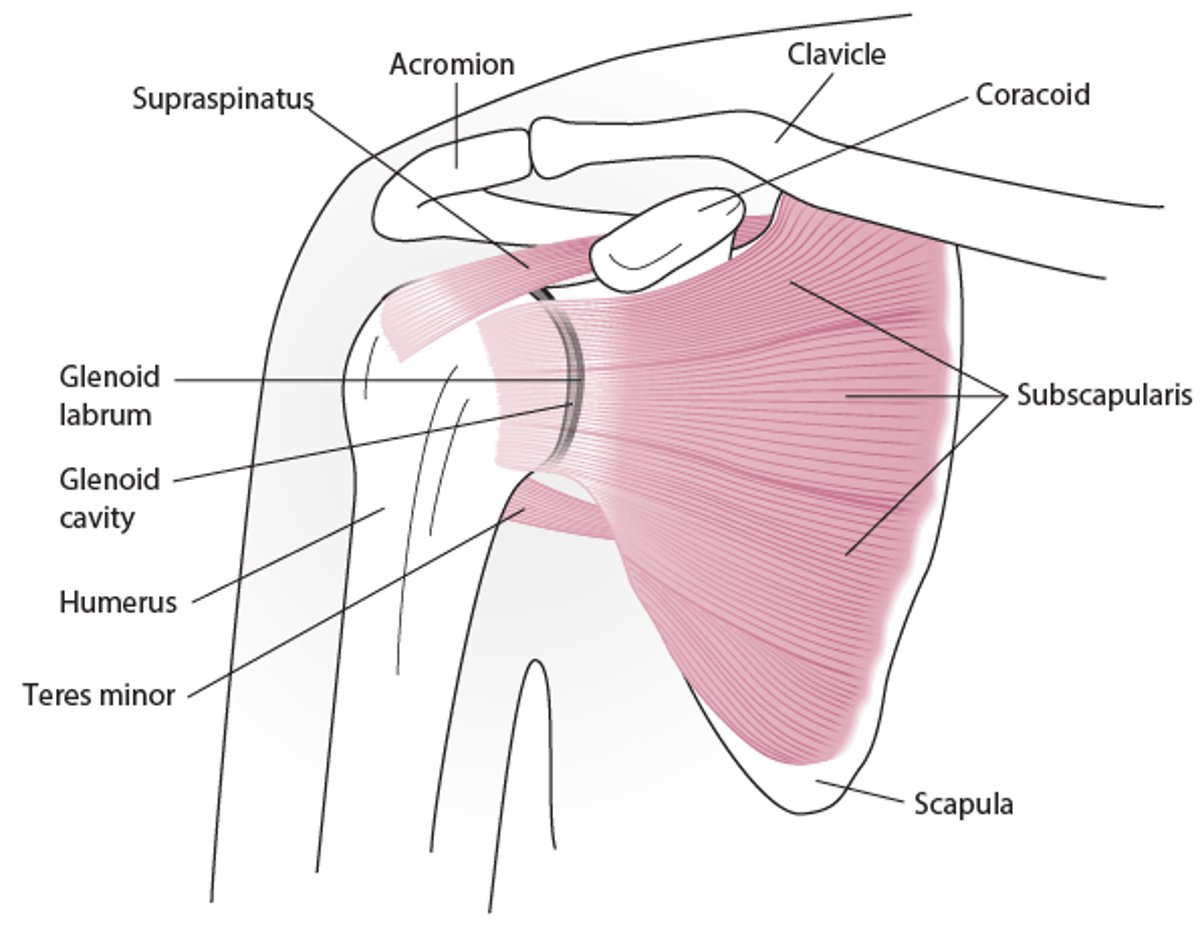
Shoulder Anatomy (Anterior View)

The Neer test checks for impingement of the rotator cuff tendons under the coracoacromial arch. It is performed by placing the arm in forced forward flexion (arm lifted overhead) with the arm fully pronated.
The Hawkins test also checks for impingement. It is performed by elevating the arm to 90°, flexing the elbow 90°, and then forcibly rotating the shoulder internally.
The Apley scratch test assesses combined shoulder range of motion by having the patient attempt to touch the opposite scapula: Reaching overhead, behind the neck, and to the opposite scapula with the tips of the fingers tests abduction and external rotation; reaching under, behind the back, and across to the opposite scapula with the back of the hand tests adduction and internal rotation.
Other areas that may be the source of shoulder pain include the acromioclavicular and sternoclavicular joints, cervical spine, biceps tendon, and scapula. These areas should be assessed for any tenderness or deformity indicating a problem in those areas.
The neck is examined as part of any shoulder evaluation because pain can be referred to the shoulder from the cervical spine (particularly with C5 radiculopathy).
Suspected rotator cuff injury can be further evaluated with MRI should a brief course of conservative treatment not result in resolution of symptoms.
Treatment of Rotator Cuff Injury
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Exercises
Sometimes surgery
In most cases of tendinitis, bursitis, and partial rotator cuff tears, nonoperative management with rest, NSAIDs, and rotator cuff–strengthening exercises are sufficient (1, 2, 3). A glucocorticoid injection into the subacromial space may occasionally be administered for short-term pain relief (eg, when symptoms are acute and severe or when prior treatment has been ineffective or NSAIDs are contraindicated) (3). However, repeat glucocorticoid injections are associated with an increased risk of tendon degeneration and their use should be limited (4).
Surgery to remove excess bone and decrease impingement may be necessary in chronic bursitis that is resistant to conservative management. Surgical repair may also be recommended if a rotator cuff injury is severe (eg, a complete tear).

1. Lie on stomach with involved arm hanging off edge of bed with thumb pointed out away from body.
2. Keep elbow straig
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on uninvolved side with pillow between arm and body of the involved side.
2. Bend involved elbow to 90°.
3. Prep
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Hold weight in hand on involved side.
2. Slightly bend hips and knees and support upper body with other hand placed
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Place band to secure object at waist level.
2. Place pillow or towel roll between elbow and body on involved side.
3
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Place band to secure object at waist level.
2. Place pillow or towel roll between elbow and body on involved side.
3
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Begin with arm at side, keep elbow straight and thumb up.
2. Move arm forward in position approximately 30° to be i
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on stomach with involved arm out to the side, off edge of bed and elbow bent to 90°.
2. Forearm should be off ed
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on stomach with involved arm down off edge of table and thumb pointed out away from body.
2. Retract and depress
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.


1. Lie on stomach with involved arm hanging off edge of bed with thumb pointed out away from body.
2. Keep elbow straight and extend arm to trunk level while squeezing the scapula down and back.
3. Return to starting position.
4. Perform 3 sets of 10 repetitions.
5. Add light weight as tolerated.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on uninvolved side with pillow between arm and body of the involved side.
2. Bend involved elbow to 90°.
3. Prepare the scapula by retracting and depressing (squeezing toward spine and downward).
4. Move forearm up by rotating at the shoulder, so the back of the hand is up toward the ceiling.
5. Slowly return to start position and repeat.
6. Perform 3 sets of 10 repetitions, 1 time a day.
7. Add light weight as tolerated.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Hold weight in hand on involved side.
2. Slightly bend hips and knees and support upper body with other hand placed on table or bed.
3. Bend elbow to 90° and extend shoulder to raise elbow to shoulder height by retracting (squeezing) the scapula.
4. Return to start position.
5. Perform 3 sets of 10 repetitions, 1 time a day.
6. Special Instructions
a. Start with 1 to 2 pound (0.5 to 1 kg) weight (ie, a soup can).
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Place band to secure object at waist level.
2. Place pillow or towel roll between elbow and body on involved side.
3. Grasp band with involved hand, with elbow bent to 90° and thumb up.
4. Internally rotate arm (pull hand inward across body), then slowly return to start position.
5. Perform 3 sets of 10 repetitions, 1 time a day.
6. Special Instructions
a. Start with least resistance band.
b. Keep arm at side and elbow flexed at 90°.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Place band to secure object at waist level.
2. Place pillow or towel roll between elbow and body on involved side.
3. Grasp band in involved hand, with elbow bent to 90° and thumb up.
4. Externally rotate arm, then slowly return to start position.
5. Perform 3 sets of 10 repetitions, 1 time a day.
6. Special Instructions
a. Start with least resistance band.
b. Keep arm at side and elbow flexed at 90°.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Begin with arm at side, keep elbow straight and thumb up.
2. Move arm forward in position approximately 30° to be in the place of the scapula or scaption.
3. In this position raise arm up staying in a pain-free range.
4. Return to starting position.
5. Perform 3 sets of 10 repetition, 1 time a day.
6. Add light weight as tolerated.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on stomach with involved arm out to the side, off edge of bed and elbow bent to 90°.
2. Forearm should be off edge of bed with thumb toward the body.
3. Retract and depress the scapula (squeeze toward spine and downward).
4. Rotate forearm upward.
5. Return to start position and repeat.
6. Perform 3 sets of 10 repetitions, 1 time a day.
7. Special Instructions
a. Do not let shoulder blade move when lifting forearm.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on stomach with involved arm down off edge of table and thumb pointed out away from body.
2. Retract and depress the scapula (squeeze toward spine and downward).
3. Lift arm upward to shoulder level.
4. Lower arm toward the floor and repeat.
5. Perform 3 sets of 10 repetitions, 1 time a day.
6. Special Instructions
a. Do not let shoulder blade move when lifting arm.
b. Keep thumb facing up toward the ceiling.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.
Treatment references
1. Dickinson RN, Kuhn JE. Nonoperative Treatment of Rotator Cuff Tears. Phys Med Rehabil Clin N Am. 2023;34(2):335-355. doi:10.1016/j.pmr.2022.12.002
2. Weber S, Chahal J. Management of Rotator Cuff Injuries. J Am Acad Orthop Surg. 2020;28(5):e193-e201. doi:10.5435/JAAOS-D-19-00463
3. Desmeules F, Roy JS, Lafrance S, et al. Rotator Cuff Tendinopathy Diagnosis, Nonsurgical Medical Care, and Rehabilitation: A Clinical Practice Guideline. J Orthop Sports Phys Ther. 2025;55(4):235-274. doi:10.2519/jospt.2025.13182
4. Puzzitiello RN, Patel BH, Nwachukwu BU, et al. Adverse Impact of Corticosteroid Injection on Rotator Cuff Tendon Health and Repair: A Systematic Review. Arthroscopy. 2020;36(5):1468-1475. doi:10.1016/j.arthro.2019.12.006
Key Points
The rotator cuff consists of the supraspinatus, infraspinatus, teres minor, and subscapularis muscles; these muscles help stabilize the humeral head during overhead arm motions (eg, pitching, swimming, weightlifting, serving in racket sports) and assist in elevation and rotation of the shoulder.
Rotator cuff muscles may be torn acutely; shoulder instability, rotator cuff weakness, or mechanical impingement in the subacromial space may cause tendinitis (particularly of the supraspinatus tendon) and result in subacromial bursitis.
Diagnosis is usually made by examination, but some patients require MRI and/or arthroscopy.
Treat with NSAIDs, rest, and rotator cuff exercises; glucocorticoid injection into the subacromial space is also an option for persistent pain.
Surgical repair may be recommended if injury is severe (eg, a complete tear).





