

Physical therapy aims to improve joint and muscle function (eg, range of motion, strength) and thus improve the patient’s ability to stand, balance, walk, and climb stairs. For example, physical therapy is commonly used to train patients with lower-extremity amputations. On the other hand, occupational therapy focuses on self-care activities and improvement of fine motor coordination of muscles and joints, particularly in the upper extremities.
(See also Overview of Rehabilitation.)
Range of motion
Limited range of motion impairs function, tends to cause pain, and can predispose patients to pressure ulcers. Range of motion should be evaluated with a goniometer before therapy and regularly thereafter.
Range-of-motion exercises stretch stiff joints. Stretching is usually most effective and least painful when heat is applied adjunctively (see Heat) (1). There are several types of range-of-motion exercises.
Active: This type is used when patients can exercise without assistance; patients must move their limbs themselves.
Active assistive: This type is used when muscles are weak or when joint movement causes discomfort; patients must move their limbs, but a therapist helps them do so.
Passive: This type is used when patients cannot actively participate in exercise; no effort is required from them.
Strength and conditioning
Many exercises aim to improve muscle strength. The Medical Research Council grading system is one of the most widely used clinical tools for grading muscle strength (see table ). Muscle strength may be increased with progressive resistive exercise. When a muscle is very weak, gravity alone is sufficient resistance. When muscle strength becomes fair, additional manual or mechanical resistance (eg, weights, spring tension, resistance bands) is added.
General conditioning exercises combine various exercises to treat the effects of debilitation, prolonged bed rest, or immobilization. The goals are to reestablish hemodynamic balance, increase cardiorespiratory capacity and endurance, and maintain range of motion and muscle strength.
For older adults, the purpose of these exercises is both to strengthen muscles enough to function normally and possibly to regain normal strength for their age.
Grades of Muscle Strength [a]
Grade | Description |
|---|---|
5 | Full strength against resistance |
4 | Active movement against moderate resistance |
3 | Active movement against gravity but not resistance |
2 | Active movement with gravity eliminated |
1 | Evidence of contraction (visible or palpable) with no or trace joint movement |
0 | No palpable or visible contraction and no joint movement |
[a] Data are adapted from the MRC Muscle Scale found in Aids to the Examination of the Peripheral Nervous System (Memorandum No. 45) and used with the permission of the Medical Research Council under Open Government Licence 3.0. | |
Proprioceptive neuromuscular facilitation
Proprioceptive neuromuscular facilitation helps promote neuromuscular activity in patients who have upper motor neuron damage with spasticity; it enables them to perceive muscle contraction and helps maintain the affected joint’s range of motion.
Proprioceptive neuromuscular facilitation (PNF) has been proposed as an effective treatment to improve basic activities of daily living (ADLs) and quality of life in patients with upper motor neuron damage and spasticity, such as that due to stroke or cerebral palsy (2). PNF involves cycles of passive stretching, isometric contractions, and additional passive stretching. PNF is performed on specific muscles to maintain range of motion and/or flexibility (eg, on the right biceps in a patient with spasticity or contractures as a result of a left middle cerebral artery infarct) (2).
Coordination exercises
Coordination exercises are task-oriented movements that train multiple joints and muscles to work together smoothly and efficiently. Examples include reaching and grasping objects at various distances, finger-to-nose tasks, touching different body parts on command, heel-to-shin sliding, or ball-handling activities such as tossing and catching.
Ambulation exercises
Before proceeding to ambulation exercises, patients must be able to balance in a standing position (3). Balancing exercise is usually done using parallel bars with a therapist standing in front of or directly behind a patient. While holding the bars, patients shift weight from side to side and from forward to backward. Once patients can balance safely, they can proceed to ambulation exercises.
Supporting a Patient During Ambulation
Aides should place one arm under that of the patient, gently grasp the patient’s forearm, and lock their arm firmly under the patient’s axilla. Thus, if the patient starts to fall, aides can provide support at the patient’s shoulder. If a patient is wearing a waist belt, aides use their free hand to grasp the belt. |

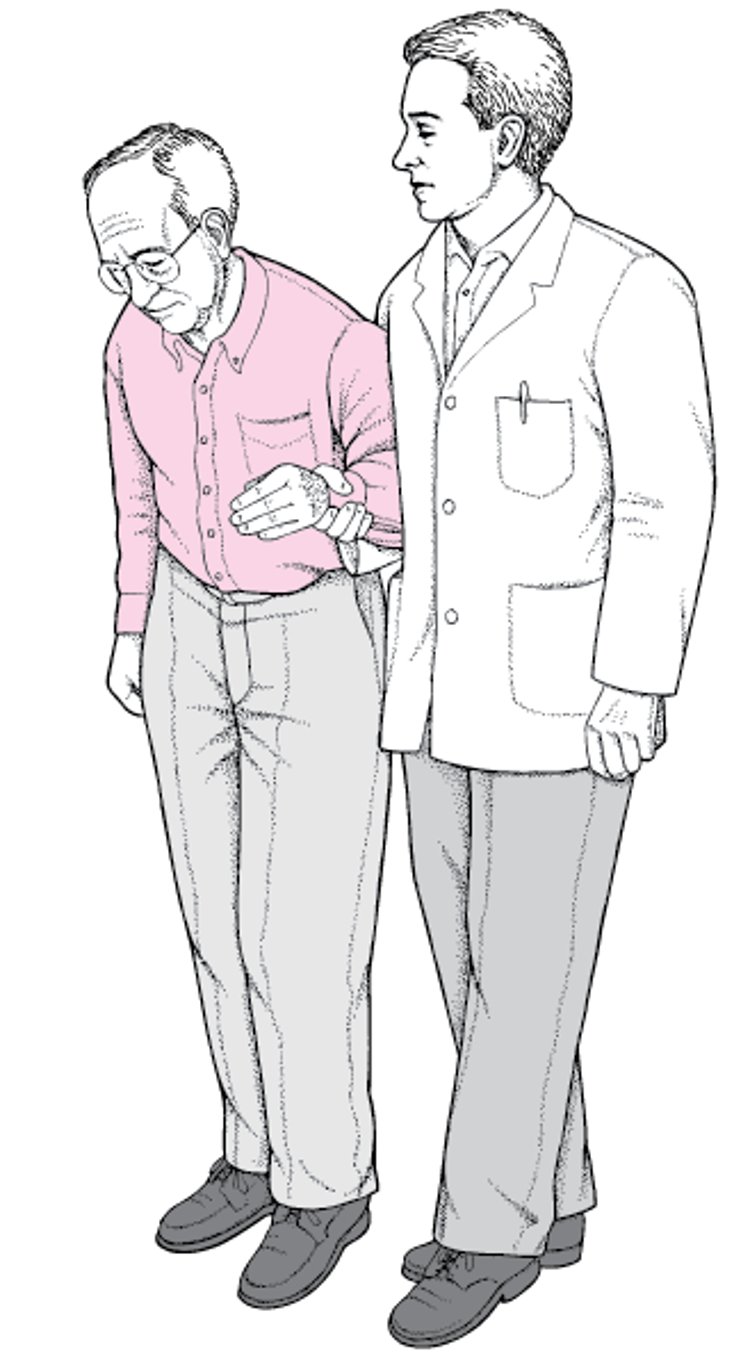
Ambulation is often a major goal of rehabilitation. If individual muscles are weak or spastic, an orthosis (eg, a brace) may be used. Ambulation exercises are commonly started after using parallel bars; as patients progress, they use a walker, crutches, or cane and then walk without devices. Some patients wear an assistive belt used by the therapist to help prevent falls. Anyone assisting patients with ambulation should know how to correctly support them (see figure ).
As soon as patients can walk safely on level surfaces, they can start training to climb stairs or to step over curbs if either skill is needed. Patients who use walkers must learn special techniques for climbing stairs and stepping over curbs. When climbing stairs, ascent starts with the better leg, and descent starts with the affected leg (ie, good leads up; bad leads down). Before patients are discharged, the social worker or physical therapist should arrange to have secure handrails installed along all stairs in the patients’ home.
Transfer training
Patients who cannot transfer independently from bed to chair, chair to commode, or chair to a standing position usually require attendants 24 hours/day. Adjusting the heights of commodes and chairs may help. Sometimes assistive devices are useful (ie, people who have difficulty standing from a seated position may benefit from a chair with a raised seat or a self-lifting chair).
References
1. Nakano J, Yamabayashi C, Scott A, et al. The effect of heat applied with stretch to increase range of motion: A systematic review. Phys Ther Sport. 2012;13(3):180-188.
2. Guiu-Tula FX, Cabanas-Valdés R, Sitjà-Rabert M, Urrútia G, Gómara-Toldrà N. The Efficacy of the proprioceptive neuromuscular facilitation (PNF) approach in stroke rehabilitation to improve basic activities of daily living and quality of life: a systematic review and meta-analysis protocol. BMJ Open. 2017;7(12):e016739. Published 2017 Dec 12. doi:10.1136/bmjopen-2017-016739
3. Hornby TG, Reisman DS, Ward IG, et al. Clinical Practice Guideline to Improve Locomotor Function Following Chronic Stroke, Incomplete Spinal Cord Injury, and Brain Injury. J Neurol Phys Ther. 2020;44(1):49-100. doi:10.1097/NPT.0000000000000303





