Orthoses provide support for damaged joints, ligaments, tendons, muscles, and bones. Most are customized to a patient’s needs and anatomy. Orthoses designed to fit into shoes may shift the patient’s weight to different parts of the foot to compensate for lost function, prevent deformity or injury, help bear weight, or relieve pain, as well as provide support. Orthoses are often very expensive and not covered by insurance.
Ambulation Aids
Characteristic | Walker | Crutches | Canes |
|---|---|---|---|
Stability | Very good | Good | Least stable |
Walking speed | Slowest | Slow | Can be fast |
Use on steps | None | Training needed | Easy |
Strength of arms required for use | Normal | Strong arms required for weight bearing | Normal |
Number of hands required for use | 2 | Usually 2 | Usually 1 |
Possibility of carrying objects | Requires attachment of basket | None | Possible |
Cost | Most expensive | Relatively inexpensive | Least expensive |
Walking aids include walkers, crutches, and canes (see figure ). They help with weight bearing, balance, or both. Each device has advantages and disadvantages, and each is available in many models. After evaluation, a therapist should choose the one that provides the best combination of stability and freedom for the patient (see table ). Physicians should know how to fit crutches (see figure ). Prescriptions for assistive devices should be as specific as possible.

Wheelchairs provide mobility to patients who cannot walk. Some models are designed to be self-propelled and to provide stability for traveling over uneven ground and up and down curbs. Other models are designed to be pushed by an assistant; they provide less stability and speed. Wheelchairs are available with various features. For athletic patients with impaired lower extremities but good upper body strength, racing wheelchairs are available. A one-arm–drive or hemi-height wheelchair may be suitable for hemiplegic patients with good coordination. If patients have little or no arm function, a motorized wheelchair is prescribed. Wheelchairs for patients with quadriplegia may have chin or mouth (sip and puff) controls and built-in ventilators.
Mobility scooters are battery-powered, wheeled carts with a steering wheel or tiller, speed control, and ability to move forward and in reverse. They are used on firm, level surfaces inside and outside buildings but cannot negotiate curbs or stairs. Scooters are helpful for people who can stand and walk short distances (ie, to transfer to and from the scooter) but who lack the strength and/or stamina to walk longer distances.
Prostheses are artificial body parts, most commonly limbs designed to replace lower or upper extremities after amputation (see Limb Prosthetics and Leg Amputation Rehabilitation). Technical innovations have greatly improved the comfort and functionality of prostheses. Many prostheses can be cosmetically altered to appear natural. A prosthetist should be involved early to help patients understand the many options in prosthetic design, which should meet the patients’ needs and safety requirements. Many patients can expect to regain considerable function. Physical therapy should be started even before the prosthesis is fitted; therapy should continue until patients can function with the new limb. Some patients seem unable to tolerate a prosthesis or complete the physical rehabilitation required to successfully use it.
(See also Overview of Rehabilitation.)
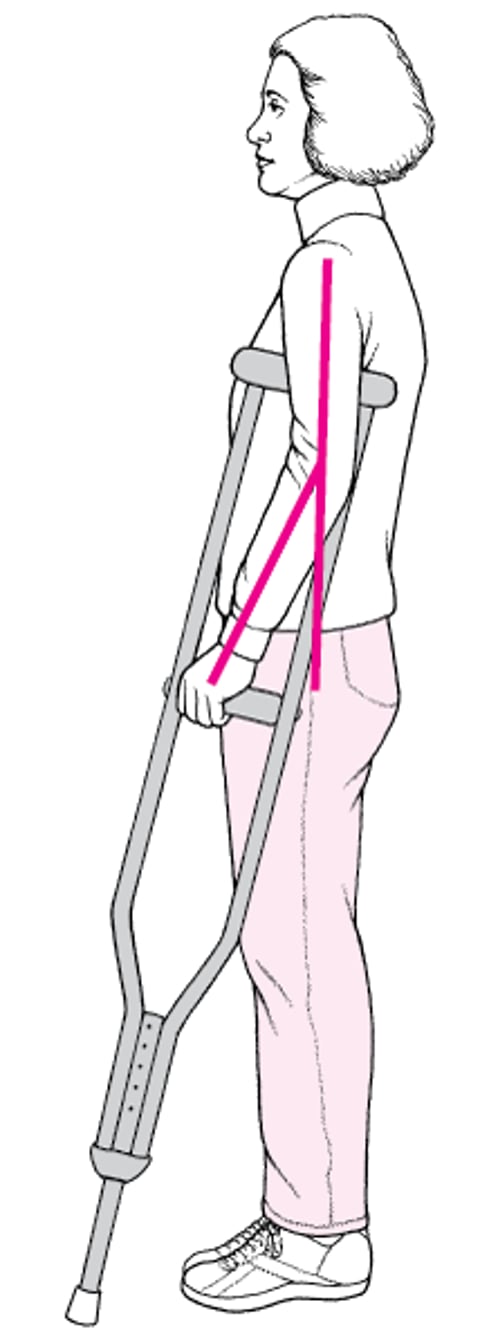
Fitting Underarm Crutches
Patients should wear the type of shoes usually worn, stand erect, and look straight ahead with the shoulders relaxed. For a correct fit, the end of each crutch should be placed approximately 5 cm from the side of the shoe and approximately 15 cm in front of the toe, and the length of the crutch should be adjusted so that the top of the crutch is about 2 to 3 finger widths (approximately 5 cm) below the axilla. The hand grip should be adjusted so that the elbow bends 15 to 30°. |

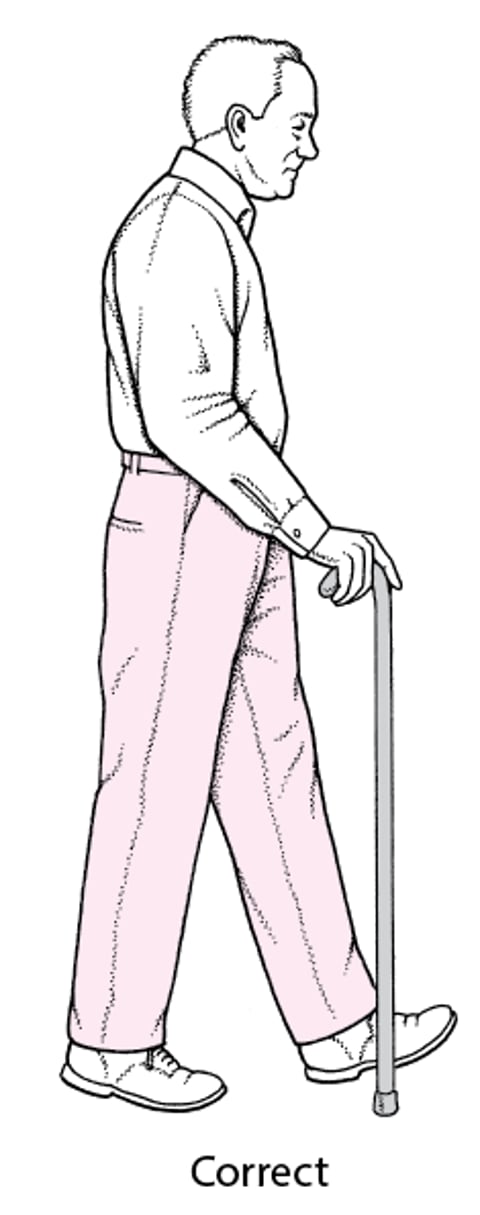
Correct Cane Height
The hand/height of the cane should be at the level of the ipsilateral greater trochanter, which results in about 20 to 30° of elbow flexion. The cane should be held in the hand contralateral to the affected hip. The cane can be held on either side for knee pain, based on safety and patient preference. |