




Syphilis is caused by the spirochete Treponema pallidum and is characterized by 3 sequential symptomatic stages separated by periods of asymptomatic latent infection. Common manifestations include genital ulcers, skin lesions, meningitis, aortic disease, and neurologic syndromes. Diagnosis is by serologic tests and adjunctive tests selected based on the disease stage. Penicillin is the treatment of choice.
(See also Overview of Sexually Transmitted Infections and Congenital Syphilis.)
Syphilis is caused by T. pallidum, a spirochete that cannot survive for long outside the human body. T. pallidum enters through the mucous membranes or skin, reaches the regional lymph nodes within hours, and rapidly spreads throughout the body.
In 2020, there were more than 130,000 reported cases of syphilis in the US. The majority of cases of primary and secondary syphilis occurred in men (81%) and, among men, 53% of cases were in men who have sex with men. The incidence of syphilis has been increasing rapidly in the US; from 2015 to 2020, the primary and secondary syphilis rate among women increased 147% (from 1.9 to 4.7 per 100,000), and the rate among men increased 34% (from 15.5 to 20.8 per 100,000) (see Centers for Disease Control and Prevention Preliminary 2021 STD Surveillance Data and Sexually Transmitted Disease Surveillance 2020: Syphilis).
Syphilis occurs in 3 stages (see table Classification of Syphilis):
Primary
Secondary
Tertiary
There are long latent periods between the stages. Infected people are contagious during the first 2 stages.
Infection is usually transmitted by sexual contact (including genital, orogenital, and anogenital) but may be transmitted nonsexually by skin contact or transplacentally, causing congenital syphilis. Risk of transmission is about 30% from a single sexual encounter with a person who has primary syphilis and 60 to 80% from an infected mother to a fetus. Infection does not lead to immunity against reinfection.
Symptoms and Signs of Syphilis
Syphilis may manifest at any stage and may affect multiple or single organs, mimicking many other disorders. Syphilis may be accelerated by coexisting HIV infection; in these cases, eye involvement, meningitis, and other neurologic complications are more common and more severe.
Syphilis should be suspected in patients with typical mucocutaneous lesions or unexplained neurologic disorders, particularly in areas where the infection is prevalent. In such areas, it should also be considered in patients with a broad range of unexplained findings. Because clinical manifestations are so diverse and advanced stages are now relatively rare in most developed countries, syphilis may escape recognition.

Image courtesy of Drs. Gavin Hart and N. J. Flumara via the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of Dr. Susan Lindsley via the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Drs. Gavin Hart and N. J. Flumara via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Dr. Susan Lindsley via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
Primary syphilis
After an incubation period of 3 to 4 weeks (range 1 to 13 weeks), a primary lesion (chancre) develops at the site of inoculation. The initial red papule quickly forms a chancre, usually a painless ulcer with a firm base; when rubbed, it produces clear fluid containing numerous spirochetes. Nearby lymph nodes may be enlarged, firm, and nontender.
Chancres can occur anywhere but are most common on the following:
Penis, anus, and rectum in men
Vulva, cervix, rectum, and perineum in women
Lips or mouth
About half of infected women and one third of infected men are unaware of the chancre because it causes few symptoms. Chancres in the rectum or mouth, usually occurring in men, are often unnoticed.
The chancre usually heals in 3 to 12 weeks. Then, people appear to be completely healthy.
Secondary syphilis
The spirochete spreads in the bloodstream, producing widespread mucocutaneous lesions, lymph node swelling, and, less commonly, symptoms in other organs. Symptoms typically begin 6 to 12 weeks after the chancre appears; about 25% of patients still have a chancre. Fever, loss of appetite, nausea, and fatigue are common. Headache (due to meningitis), hearing loss (due to otitis), balance problems (due to labyrinthitis), visual disturbances (due to retinitis or uveitis), and bone pain (due to periostitis) can also occur.
Over 80% of patients have mucocutaneous lesions; a wide variety of rashes and lesions occur, and any body surface can be affected. Without treatment, lesions may disappear in a few days to weeks, persist for months, or return after healing, but all eventually heal, usually without scarring.
Syphilitic dermatitis is usually symmetric and more marked on the palms and soles. The individual lesions are round, often scale, and may coalesce to produce larger lesions, but they generally do not itch or hurt. After lesions resolve, the affected areas may be lighter or darker than normal. If the scalp is involved, alopecia areata often occurs.
Condyloma lata are hypertrophic, flattened, dull pink or gray papules at mucocutaneous junctions and in moist areas of the skin (eg, in the perianal area, under the breasts); lesions are extremely infectious. Lesions of the mouth, throat, larynx, penis, vulva, or rectum are usually circular, raised, and often gray to white with a red border.
Secondary syphilis can affect many other organs:
About half of patients have lymphadenopathy, usually generalized, with nontender, firm, discrete nodes, and often hepatosplenomegaly.
About 10% of patients have lesions in other organs, such as the eyes (uveitis), bones (periostitis), joints, meninges, kidneys (glomerulitis), liver (hepatitis), or spleen.
About 10 to 30% of patients have mild meningitis, but < 1% have meningeal symptoms, which can include headache, neck stiffness, cranial nerve lesions, deafness, and eye inflammation (eg, optic neuritis, retinitis).
However, acute or subacute meningitis is more common among patients with HIV infection and may manifest as meningeal symptoms or strokes due to intracranial vasculitis.

Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of Susan Lindsley via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.

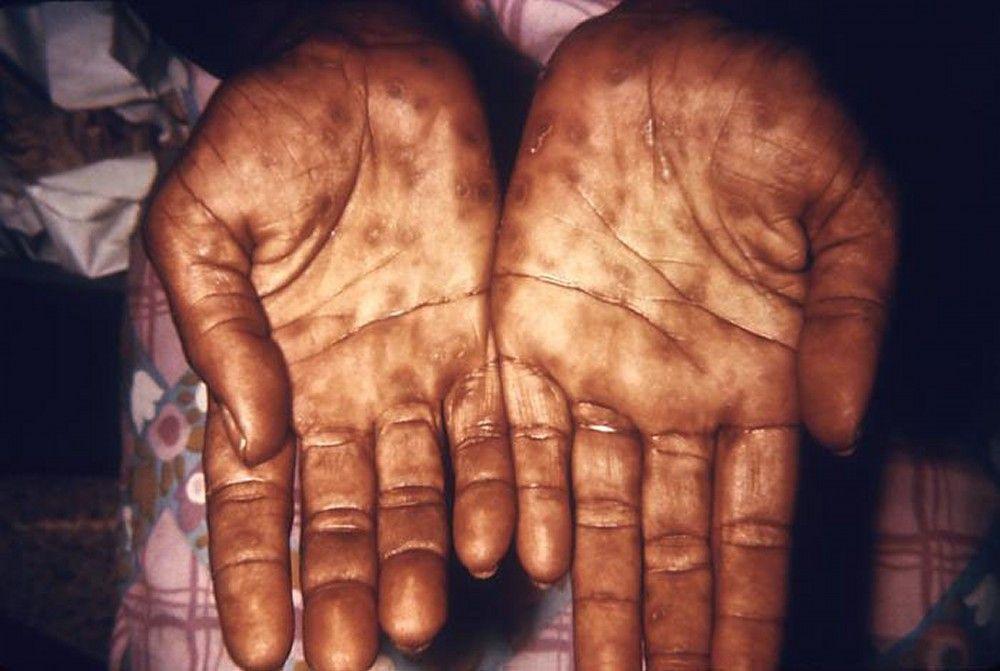
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Susan Lindsley via the Public Health Image Library of the Centers for Disease Control and Prevention.
Latent period
Latent syphilis can be early (< 1 year after infection) or late (≥ 1 year after infection).
Symptoms and signs are absent, but antibodies, detected by serologic tests for syphilis (STS), persist. Because symptoms of primary and secondary syphilis are often minimal or ignored, patients frequently are first diagnosed during the latent stage when routine blood tests for syphilis are done.
Syphilis may remain latent permanently, but relapses with contagious skin or mucosal lesions may occur during the early latent period.
Patients are often given antibiotics for other disorders, which may cure latent syphilis and may account for the rarity of late-stage disease in developed countries.
Late or tertiary syphilis
About one third of untreated people develop late syphilis, although not until years to decades after the initial infection. Lesions may be clinically classified as
Benign tertiary syphilis
Cardiovascular syphilis
Neurosyphilis
Benign tertiary gummatous syphilis usually develops within 3 to 10 years of infection and may involve the skin, bones, and internal organs. Gummas are soft, destructive, inflammatory masses that are typically localized but may diffusely infiltrate an organ or tissue; they grow and heal slowly and leave scars.


BSIP, SIDEA REVUZ/SCIENCE PHOTO LIBRARY
Benign tertiary syphilis of bone results in either inflammation or destructive lesions that cause a deep, boring pain, characteristically worse at night.
Cardiovascular syphilis usually manifests 10 to 25 years after the initial infection as any of the following:
Aneurysmal dilation of the ascending aorta
Insufficiency of the aortic valve
Narrowing of the coronary arteries
Pulsations of the dilated aorta may cause symptoms by compressing or eroding adjacent structures in the chest. Symptoms include brassy cough and obstruction of breathing due to pressure on the trachea, hoarseness due to vocal cord paralysis resulting from compression of the left laryngeal nerve, and painful erosion of the sternum and ribs or spine.
Neurosyphilis has several forms:
Asymptomatic neurosyphilis
Meningovascular neurosyphilis
Parenchymatous neurosyphilis
Tabes dorsalis
Asymptomatic neurosyphilis causes mild meningitis in about 15% of patients originally diagnosed as having latent syphilis, in 25 to 40% of those with secondary syphilis, in 12% of those with cardiovascular syphilis, and in 5% of those with benign tertiary syphilis. Without treatment, it evolves to symptomatic neurosyphilis in 5%. If cerebrospinal fluid (CSF) examination does not detect evidence of meningitis 2 years after the initial infection, neurosyphilis is unlikely to develop.
Meningovascular neurosyphilis results from inflammation of large- to medium-sized arteries of the brain or spinal cord; symptoms typically occur 5 to 10 years after infection and range from none to strokes. Initial symptoms may include headache, neck stiffness, dizziness, behavioral abnormalities, poor concentration, memory loss, lassitude, insomnia, and blurred vision. Spinal cord involvement may cause weakness and wasting of shoulder-girdle and arm muscles, slowly progressive leg weakness with urinary or fecal incontinence or both, and, rarely, sudden paralysis of the legs due to thrombosis of spinal arteries.
Parenchymatous neurosyphilis (general paresis, or dementia paralytica) results when chronic meningoencephalitis causes destruction of cortical parenchyma. It usually develops 15 to 20 years after initial infection and typically does not affect patients before their 40s or 50s. Behavior progressively deteriorates, sometimes mimicking a mental disorder or dementia. Irritability, difficulty concentrating, deterioration of memory, defective judgment, headaches, insomnia, fatigue, and lethargy are common; seizures, aphasia, and transient hemiparesis are possible. Hygiene and grooming deteriorate. Patients may become emotionally unstable and depressed and have delusions of grandeur with lack of insight; wasting may occur. Tremors of the mouth, tongue, outstretched hands, and whole body may occur; other signs include pupillary abnormalities, dysarthria, hyperreflexia, and, in some patients, extensor plantar responses. Handwriting is usually shaky and illegible.
Tabes dorsalis (locomotor ataxia) involves slow, progressive degeneration of the posterior columns and nerve roots. It typically develops 20 to 30 years after initial infection; mechanism is unknown. Usually, the earliest, most characteristic symptom is an intense, stabbing (lightning) pain in the back and legs that recurs irregularly with loss of vibratory sense, proprioception, and reflexes in the lower extremities. Gait ataxia, hyperesthesia, and paresthesia may produce a sensation of walking on foam rubber. Loss of bladder sensation leads to urine retention, incontinence, and recurrent infections. Erectile dysfunction is common.
Most patients with tabes dorsalis are thin and have characteristic sad facies and Argyll Robertson pupils (pupils that accommodate for near vision but do not respond to light). Optic atrophy may occur. Examination of the legs detects hypotonia, hyporeflexia, impaired vibratory and joint position sense, ataxia in the heel-shin test, absence of deep pain sensation, and Romberg sign. Tabes dorsalis tends to be intractable even with treatment.
Visceral crises (episodic pain) are a variant of tabes dorsalis; paroxysms of pain occur in various organs, most commonly in the stomach (causing vomiting) but also in the rectum, bladder, and larynx.
Other lesions
Syphilitic ocular and otic manifestations can occur at any stage of the disease.
Ocular syndromes can affect virtually any part of the eye; they include interstitial keratitis, uveitis (anterior, intermediate, and posterior), chorioretinitis, retinitis, retinal vasculitis, and cranial nerve and optic neuropathies. Cases of ocular syphilis have occurred among HIV-infected men who have sex with men. Several cases resulted in significant morbidity, including blindness. Patients with ocular syphilis are at risk of neurosyphilis.
Otosyphilis may affect the cochlea (causing hearing loss and tinnitus) or vestibular system (causing vertigo and nystagmus).
Trophic lesions, secondary to hypoesthesia of the skin or periarticular tissues, may develop in the later stages. Trophic ulcers may develop on the soles of the feet and penetrate as deeply as the underlying bone.
Neurogenic arthropathy (Charcot joints), a painless joint degeneration with bony swelling and abnormal range of movement, is a classic manifestation of neuropathy.
Diagnosis of Syphilis
Serologic reaginic tests (rapid plasma reagin [RPR] or Venereal Disease Research Laboratory [VDRL]) for screening blood and diagnosing central nervous system infections
Serologic treponemal tests (eg, fluorescent treponemal antibody absorption or microhemagglutination assay for antibodies to T. pallidum)
The US Preventive Services Task Force recommends that asymptomatic, nonpregnant adolescents and adults who are at increased risk for syphilis infection be screened for syphilis. (See US Preventive Services Task Force: Syphilis Infection in Nonpregnant Adolescents and Adults: Screening.)
Diagnostic test selection depends on which stage of syphilis is suspected. Neurologic infection is best detected by and followed with quantitative reaginic tests of cerebrospinal fluid (CSF). Cases must be reported to public health agencies.
Diagnostic tests for syphilis
Tests include serologic tests for syphilis (STS), which consist of
Screening (a reaginic, or nontreponemal) tests
Confirmatory (treponemal) tests
Darkfield microscopy
T. pallidum cannot be grown in vitro. Traditionally, reaginic tests have been done first, and positive results are confirmed by a treponemal test. Some laboratories now reverse this sequence; they do newer, inexpensive treponemal tests first and confirm positive results using a nontreponemal test.
Nontreponemal (reaginic) tests use lipid antigens (cardiolipin from bovine hearts) to detect reagin (human antibodies that bind to lipids). The Venereal Disease Research Laboratory (VDRL) and rapid plasma reagin (RPR) tests are sensitive, simple, and inexpensive reaginic tests that are used for screening but are not completely specific for syphilis. Results may be presented qualitatively (eg, reactive, weakly reactive, borderline, or nonreactive) and quantitatively as titers (eg, positive at 1:16 dilution).
In addition to treponemal infections, the following can produce a positive (biologically false-positive) reagin test result:
Systemic infections unrelated to syphilis (such as tuberculosis, rickettsial diseases, and endocarditis)
Immunization (specifically COVID-19 or smallpox vaccines)
Systemic lupus erythematosus
Antiphospholipid antibody syndromes
Pregnancy
Cerebrospinal fluid (CSF) reaginic tests are reasonably sensitive for early disease but less so for late neurosyphilis. CSF reagin tests can be used to diagnose neurosyphilis or to monitor response to treatment by measuring antibody titers.
Treponemal tests detect antitreponemal antibodies qualitatively and are very specific for syphilis. They include the following:
Fluorescent treponemal antibody absorption (FTA-ABS) test
Microhemagglutination assay for antibodies to T. pallidum (MHA-TP)
T. pallidum hemagglutination assay (TPHA)
T. pallidum enzyme immunoassay (TP-EIA)
Chemoluminescence immunoassays (CLIA)
If they do not confirm treponemal infection after a positive reaginic test, the reaginic result is deemed biologically false-positive. Treponemal tests of CSF are controversial, but some authorities believe the FTA-ABS test is sensitive.
Neither reaginic nor treponemal tests become positive until 3 to 6 weeks after the initial infection. Thus, a negative result is common in early primary syphilis and does not exclude syphilis until after 6 weeks. Reaginic titers decrease at least 4-fold after effective treatment, typically becoming negative by 1 year in primary and by 2 years in secondary syphilis; however, low titers (≤ 1:8) may persist in about 15% of patients, a response referred to as the "serofast reaction." Treponemal tests usually remain positive for many decades, despite effective treatment and thus cannot be used to assess effectiveness.
Choice of tests and interpretation of test results depend on various factors, including previous syphilis, possible exposure to syphilis, and results of testing.
If patients have had syphilis, a reaginic test is done. A 4-fold increase in titer suggests new infection or failed treatment.
If patients have not had syphilis, treponemal and reaginic tests are done. Test results determine the next steps:
Positive results on both tests: These results suggest new infection.
Positive results on the treponemal test, but negative results on the reaginic test: A second treponemal test is done to confirm the positive test. If reaginic test results are repeatedly negative, treatment is not indicated.
Positive results on treponemal test, negative results on the reaginic test, but history suggests recent exposure: A reaginic test is repeated 2 to 4 weeks after exposure to make sure any new infection is detected.
Darkfield microscopy directs light obliquely through a slide of exudate from a chancre or lymph node aspirate to directly visualize spirochetes. Although the skills and equipment required are not usually available, darkfield microscopy is the most sensitive and specific test for early primary syphilis. The spirochetes appear against a dark background as bright, motile, narrow coils that are about 0.25 micrometers wide and 5 to 20 micrometers long. They must be distinguished morphologically from nonpathogenic spirochetes, which may be part of the normal flora, especially of the mouth. Therefore, darkfield examination of intraoral specimens for syphilis is not done.
Primary syphilis
Primary syphilis is usually suspected based on relatively painless genital (but occasionally extragenital) ulcers. Syphilitic ulcers should be differentiated from other sexually transmitted genital lesions (see table Differentiating Common Sexually Transmitted Genital Lesions). Coinfections with 2 ulcer-causing pathogens (eg, herpes simplex virus plus T. pallidum) are not rare.
Darkfield microscopy of exudate from a chancre or lymph node aspirate may be diagnostic. If results are negative or the test is unavailable, a reaginic STS is done. If results are negative or the test cannot be done immediately but a skin lesion has been present for < 3 weeks (before the STS becomes positive) and an alternate diagnosis seems unlikely, treatment may be instituted, and the STS repeated in 2 to 4 weeks.
Patients with syphilis should be tested for other sexually transmitted infections (STIs), including HIV infection, at diagnosis and 6 months later.
Secondary syphilis
Because syphilis can mimic many diseases, it should be considered when any cutaneous eruption or mucosal lesion is undiagnosed, particularly if patients have any of the following:
Generalized lymphadenopathy
Lesions on the palms or soles
Condyloma lata
Risk factors (eg, HIV, multiple sex partners)
Clinically, secondary syphilis may be mistaken for a medication eruption, rubella, infectious mononucleosis, erythema multiforme, pityriasis rubra pilaris, fungal infection, or, particularly, pityriasis rosea. Condyloma lata may be mistaken for warts, hemorrhoids, or pemphigus vegetans; scalp lesions may be mistaken for ringworm or idiopathic alopecia areata.
Secondary syphilis is excluded by a negative reaginic STS, which is virtually always reactive during this stage, often with a high titer. A compatible syndrome with a positive STS (reaginic or treponemal) warrants treatment. Uncommonly, this combination represents latent syphilis coexisting with another skin disease. Patients with secondary syphilis should be tested for other STIs.
Latent syphilis
Asymptomatic, latent syphilis is diagnosed when reaginic and treponemal STSs are positive in the absence of symptoms or signs of active syphilis. Such patients should have a thorough examination, particularly genital, skin, neurologic, and cardiovascular examinations, to exclude secondary and tertiary syphilis.
Criteria for early latent syphilis include during the prior year, a documented conversion from negative to positive treponemal test, a newly positive nontreponemal test, or a sustained (> 2 weeks) 4-fold or greater increase in reaginic test titers plus any of the following:
Unequivocal symptoms of primary or secondary syphilis
A sex partner with documented primary, secondary, or early latent syphilis
No possible exposure except during the previous 12 months
Patients who have latent syphilis but do not fulfill the above criteria have late latent syphilis.
Treatment and serologic follow-up for up to several years may be needed to ensure the success of therapy because reaginic STS titers decrease slowly.
Latent acquired syphilis must be differentiated from latent congenital syphilis, latent yaws, and other treponemal infections.
Late or tertiary syphilis
Patients with symptoms or signs of tertiary syphilis (particularly unexplained neurologic abnormalities) require STS. If the test is reactive, the following should be done:
Lumbar puncture for CSF examination (including reaginic STS)
Imaging of the brain and aorta
Screening of any other organ systems clinically suspected to be involved
At this stage of syphilis, a reaginic STS is nearly always positive, except in a few cases of tabes dorsalis.
In benign tertiary syphilis, differentiation from other inflammatory mass lesions or ulcers may be difficult without biopsy.
Cardiovascular syphilis is suggested by symptoms and signs of aneurysmal compression of adjacent structures, particularly stridor or hoarseness.
Syphilitic aortic aneurysm is suggested by aortic insufficiency without aortic stenosis and, on chest x-ray, by widening of the aortic root and linear calcification on the walls of the ascending aorta. Diagnosis of aneurysm is confirmed with aortic imaging (transesophageal echocardiography, CT, or MRI).
In neurosyphilis, most symptoms and signs, except for Argyll Robertson pupil, are nonspecific, so that diagnosis relies heavily on a high index of clinical suspicion. In parenchymatous neurosyphilis, the CSF reaginic and serum treponemal tests are reactive, and CSF typically has lymphocytic pleocytosis and elevated protein. In tabes dorsalis, serum reaginic tests may be negative if patients have been previously treated, but serum treponemal tests are usually positive. CSF usually has lymphocytic pleocytosis and elevated protein, and sometimes reaginic or treponemal test results are positive; however, in many treated patients, CSF is normal.
CSF finding can be found at any stage of syphilis. If a lumbar puncture is done without neurological symptoms or signs, then a diagnosis of asymptomatic neurosyphilis is made based on abnormal CSF (typically, lymphocytic pleocytosis and elevated protein) and a reactive CSF reaginic test (in the absence of grossly bloody contamination of the CSF). If present, HIV may confound the diagnosis because it causes mild pleocytosis and various other neurologic symptoms. Asymptomatic neurosyphilis does not require any different treatments than those recommended for the stage of syphilis.
If ocular syphilis is diagnosed, CSF testing for neurosyphilis should be done. Patients with ocular symptoms and reactive syphilis serology need a full eye examination, including cranial nerve evaluation. If cranial nerve dysfunction is present, a lumbar puncture should be performed. Patients with reactive syphilis serology and isolated ocular finding but no cranial nerve dysfunction or neurologic finding do not need CSF examination before treatment. Ocular syphilis should be treated using the same regimen as for neurosyphilis.
Hearing loss can occur at any stage of syphilis and also can be isolated or be associated with neurosyphilis. With isolated auditory symptoms and normal neurologic examination, CSF examination is not recommended before treatment. Otosyphilis should be treated using the same regimen as for neurosyphilis.
Treatment of Syphilis
Aqueous penicillin for ocular syphilis or neurosyphilis
Treatment of sex partners
The treatment of choice in all stages of syphilis and during pregnancy is
The sustained-release penicillin benzathine penicillin (Bicillin L-A)
The combination of benzathine and procaine penicillin (Bicillin C-R) should not be used.
All sex partners of a patient diagnosed with syphilis should be evaluated. Sex partners are treated in the following circumstances:
People who had sexual contact with a patient within the 90 days before the patient was diagnosed with primary, secondary, or early latent syphilis should be treated presumptively for early syphilis, even if serologic test results are negative.
People who had sexual contact with a patient > 90 days before the patient was diagnosed with primary, secondary, or early latent syphilis should be treated presumptively for early syphilis if serologic test results are not immediately available and the opportunity for follow-up is uncertain. If serologic tests are negative, no treatment is needed. If serologic tests are positive, treatment should be based on clinical and serologic evaluation and stage of syphilis.
Pearls & Pitfalls
|
Primary, secondary, and early latent syphilis
< 1 year) latent syphilis. Doses of 1.2 million units are usually given in each buttock to reduce local reactions.
Additional doses of 2.4 million units should be given 7 and 14 days after the first (total of 3 doses) for late (> 1 year) latent syphilis or latent syphilis of unknown duration because treponemes occasionally persist in the CSF after single-dose regimens. Treatment is the same regardless of HIV status.
Late latent or tertiary syphilis
Late latent syphilis
Benign or cardiovascular tertiary syphilis can be treated in the same way as late latent syphilis.
For ocular syphilis, otic syphilis, or neurosyphilis, one of the following is recommended:
Aqueous penicillin 3 to 4 million units IV every 4 hours (penetrates the central nervous system best but may be impractical)
Both medications are given for 10 to 14 days, followed by benzathine penicillin 2.4 million units IM once a week for 1 to 3 weeks after completion of these neurosyphilis treatment regimens to provide a total duration of therapy comparable to that for late latent syphilis.
Patients with tabes dorsalis
Jarisch-Herxheimer reaction (JHR)
Most patients with primary or secondary syphilis, especially those with secondary syphilis, have a JHR within 6 to 12 hours of initial treatment. It typically manifests as malaise, fever, headache, sweating, rigors, anxiety, or a temporary exacerbation of the syphilitic lesions. The mechanism is not understood, and JHR may be misdiagnosed as an allergic reaction.
JHR usually subsides within 24 hours and poses no danger. However, patients with general paresis or a high CSF cell count may have a more serious reaction, including seizures or strokes, and should be warned and observed accordingly.
Unanticipated JHR may occur if patients with undiagnosed syphilis are given antitreponemal antibiotics for other infections.
Posttreatment surveillance
After treatment, patients should have
Examinations and reaginic tests at 3, 6, and 12 months and annually thereafter until the test is nonreactive or until a durable 4-fold reduction in titer is achieved
For neurosyphilis, CSF testing every 6 months until CSF cell count is normal
The importance of repeated tests to confirm cure should be explained to patients before treatment. Examinations and reaginic tests should be done at 3, 6, and 12 months after treatment and annually thereafter until the test is nonreactive. Failure of titers to decline by 4-fold at 6 months suggests treatment failure. After successful treatment, primary lesions heal rapidly, and plasma reaginic titers fall and usually become qualitatively negative within 9 to 12 months.
In about 15% of patients with primary or secondary syphilis treated as recommended, the reaginic titer does not decrease by 4-fold—the criterion used to define response at 1 year after treatment. These patients should be followed clinically and serologically; they should also be evaluated for HIV infection.
If neurologic symptoms or signs are identified, a CSF evaluation is recommended, with findings guiding management. If follow-up cannot be ensured, CSF should be checked for neurosyphilis (because unrecognized neurosyphilis may be the cause of treatment failure), or patients should be retreated with benzathine penicillin 2.4 million units IM once a week for 3 weeks.
Treponemal tests may remain positive for decades or permanently and should not be measured to monitor progress. Serologic or clinical relapse, usually affecting the nervous system, may occur after 6 to 9 months, but the cause may be reinfection rather than relapse.
Patients with neurosyphilis without HIV infection or those with HIV infection who are on effective ART and who exhibit serologic (normalization of the serum RPR titer) and clinical responses after treatment do not need repeated CSF examinations. In HIV-infected patients, persisting CSF pleocytosis may represent effects of HIV rather than persisting neurosyphilis. Normal CSF cell count, negative CSF and serum reaginic test results, and negative neurologic examination findings for 2 years indicates probable cure. If any of the following is present, retreatment with a more intensive regimen of antibiotics is indicated:
CSF cell count that remains abnormal for > 2 years
A serum reaginic test that remains reactive for > 2 years
An increasing serum reaginic test titer
Clinical relapse
Key Points
Syphilis has 3 sequential clinical, symptomatic stages separated by periods of asymptomatic latent infection.
A characteristic skin lesion (chancre) typically appears at the site of primary infection.
Subsequently, almost any organ can be affected, but skin, mucous membranes, eyes, bone, aorta, meninges, and the brain are commonly affected.
Diagnose using a nontreponemal (reaginic) test (eg, rapid plasma reagin [RPR] or Venereal Disease Research Laboratory [VDRL]), and confirm positive results using a treponemal antibody test.
Report cases of syphilis to public health agencies.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
US Preventive Services Task Force: Syphilis Infection: Screening: Recommendations applying to asymptomatic, nonpregnant adults and adolescents who are at increased risk for syphilis infection
Centers for Disease Control and Prevention: Sexually Transmitted Infections Treatment Guidelines, 2021: Syphilis: A source of clinical guidance emphasizing treatment of STIs and discussing prevention strategies and diagnostic recommendations






