


Pain in and around the teeth is a common problem, particularly among patients with poor oral hygiene. Pain may be constant, felt after stimulation (eg, heat, cold, sweet food or drink, chewing, brushing), or both.
(See also Evaluation of the Dental Patient.)
Etiology of Toothache
The most common causes of toothache (see table Some Causes of Toothache) are
Dental caries
Pulpitis
Periapical abscess
Trauma
Erupting wisdom tooth (causing pericoronitis)
Toothache is usually caused by dental caries and its consequences.
Caries (tooth decay) causes pain when the lesion extends through the enamel into dentin (resulting in sufficient demineralization of tooth structure to cause a cavitation in the outer surface of the tooth enamel). Pain usually occurs after stimulation from cold, heat, sweet food or drink, or brushing; these stimuli cause fluid to move within dentinal tubules to induce a response in the pulp. As long as the discomfort does not persist after the stimulus is removed, the pulp is likely healthy enough to be maintained. This is referred to as normal dentinal sensitivity, reversible pulpalgia, or reversible pulpitis.
Pulpitis is inflammation of the pulp, typically due to advancing caries, cumulative minor pulp damage resulting from previous large restorations, a defective restoration, or trauma. It may be reversible or irreversible. Pressure necrosis frequently results from pulpitis. Pain may be spontaneous or in response to stimulation, particularly heat or cold. In both cases, pain lingers for a minute or longer. Once the pulp becomes necrotic, pain ends briefly (hours to weeks). Subsequently, periapical inflammation (apical periodontitis) or an abscess develops.
Periapical abscess may follow untreated caries or pulpitis. The tooth is extremely sensitive to percussion (eg, tapping with a metal dental probe or tongue blade) and chewing. The abscess may point intraorally and eventually drain or may become a cellulitis.
Tooth trauma can damage the pulp. The damage may manifest soon after the injury or up to decades later.

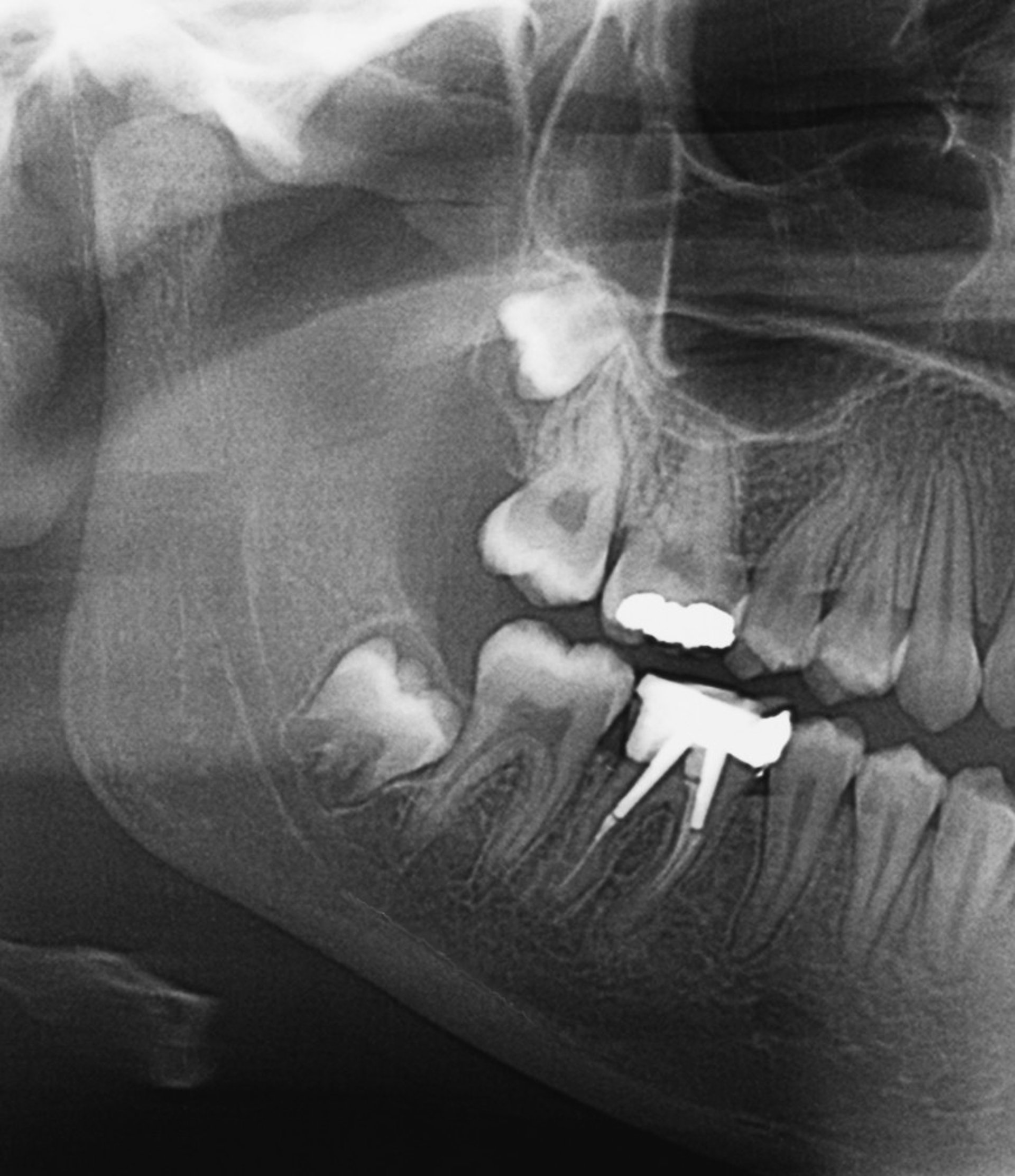
ZEPHYR/SCIENCE PHOTO LIBRARY
Pericoronitis is inflammation and infection of the tissue between the tooth and its overlying flap of gingiva (operculum). It usually occurs in an erupting wisdom tooth (almost always a lower one).
Complications
Rarely, sinusitis results from untreated maxillary dental infection. More commonly, pain resulting from a sinus infection is perceived as originating in the unaffected teeth adjacent to the sinus, mistakenly creating the impression of a dental origin.
Rarely, cavernous sinus thrombosis or Ludwig angina (submandibular space infection) develops; these conditions are life threatening and require immediate intervention.
Evaluation of Toothache
History
History of present illness should identify the location and duration of the pain and whether it is constant or present only after stimulation. Specific triggering factors to review include heat, cold, sweet food or drink, chewing, and brushing. Any preceding trauma or dental work should be noted.
Review of systems should seek symptoms of complications, including face pain, swelling, or both (dental abscess, sinusitis); pain below the tongue, difficulty swallowing, and tongue elevation or protrusion (submandibular space infection); pain with bending forward (sinusitis); and retro-orbital headache, fever, and vision symptoms (cavernous sinus thrombosis).
Past medical history should note previous dental problems and treatment.
Physical examination
Vital signs are reviewed for fever.
The examination focuses on the face and mouth. The face is inspected for swelling and is palpated for induration and tenderness.
The oral examination includes inspection for gum inflammation and caries and any localized swelling at the base of a tooth that may represent a pointing apical abscess. If no tooth is clearly involved, teeth in the area of pain are percussed for tenderness with a tongue depressor. Also, an ice cube or a dental refrigerant–chilled cotton pellet can be applied briefly to each tooth, removing it immediately once pain is felt. In healthy teeth, the pain stops almost immediately. Pain lingering more than a few seconds indicates pulp damage (eg, irreversible pulpitis). The floor of the mouth is palpated for induration and tenderness, suggesting a deep space infection.
Neurologic examination, concentrating on the cranial nerves, should be done in patients with fever, headache, or facial swelling.
Red flags
Findings of particular concern are
Headache
Fever
Swelling or tenderness of floor of the mouth
Cranial nerve abnormalities
Interpretation of findings
Red flag finding of headache suggests sinusitis, particularly if multiple upper molar and premolar (back) teeth are painful. However, presence of vision symptoms or abnormalities of the pupils or of ocular motility suggests cavernous sinus thrombosis.
Fever is unusual with routine dental infection unless there is significant local extension.
Bilateral tenderness and swelling of the floor of the mouth suggest Ludwig angina. Difficulty opening the mouth (trismus) can occur with any lower molar infection but is common only with pericoronitis.
Isolated dental condition: Patients without red flag findings or facial swelling likely have an isolated dental condition, which, although uncomfortable, is not serious. Clinical findings, particularly the nature of the pain, help suggest a cause (see tables Some Causes of Toothache and Characteristics of Pain in Toothache). Because of its innervation, the pulp can perceive stimuli (eg, heat, cold, sweets) only as pain. An important distinction is whether there is continuous pain or pain only on stimulation and, if pain is only on stimulation, whether the pain lingers after the stimulus is removed.
Swelling at the base of a tooth, on the cheek, or both indicates infection, either cellulitis or abscess. A tender, fluctuant area at the base of a tooth suggests a pointing abscess.
Testing
Dental x-rays are the mainstay of testing but can be deferred to a dentist.
The rare cases in which cavernous sinus thrombosis or Ludwig angina are suspected require imaging studies, typically CT or MRI.
Treatment of Toothache
Topical or oral analgesics
Sometimes rinses or systemic antibiotics
Analgesics (see Treatment of Pain
Procedure demonstrated by Scott Solow, DDS, Pediatric Dentistry and Orthodontics. Filmed on location at Pediatric Dentistry and Orthodontics Medical Arts Building, Philadelphia, PA.
© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.
© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.
© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.
Procedure demonstrated by Scott Solow, DDS, Pediatric Dentistry and Orthodontics. Filmed on location at Pediatric Dentistry and Orthodontics Medical Arts Building, Philadelphia, PA.
Procedure demonstrated by Scott Solow, DDS, Pediatric Dentistry and Orthodontics. Filmed on location at Pediatric Dentistry and Orthodontics Medical Arts Building, Philadelphia, PA.

Procedure demonstrated by Scott Solow, DDS, Pediatric Dentistry and Orthodontics. Filmed on location at Pediatric Dentistry and Orthodontics Medical Arts Building, Philadelphia, PA.
© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

Procedure demonstrated by Scott Solow, DDS, Pediatric Dentistry and Orthodontics. Filmed on location at Pediatric Dentistry and Orthodontics Medical Arts Building, Philadelphia, PA.
Procedure demonstrated by Scott Solow, DDS, Pediatric Dentistry and Orthodontics. Filmed on location at Pediatric Dentistry and Orthodontics Medical Arts Building, Philadelphia, PA.
(See also How To Do an Emergency Tooth Extraction.)
Antibiotics directed at oral flora are given for most disorders beyond irreversible pulpitis (eg, necrotic pulp, abscess, cellulitis). It is not clear whether antibiotics are beneficial for irreversible pulpitis (1Clostridioides difficile–induced diarrhea.
An abscess associated with well-developed (soft) fluctuance is typically drained through an incision with a #15 scalpel blade at the most dependent point of the swelling. A rubber drain, held by a suture, may be placed. (See How To Drain a Tooth Abscess.)
Pericoronitis
Teething pain
The rare patient with cavernous sinus thrombosis or Ludwig angina requires immediate hospitalization, removal of the infected tooth, and culture-guided parenteral antibiotics.
Treatment reference
1. Fedorowicz Z, van Zuuren EJ, Farman AG, et al: Antibiotic use for irreversible pulpitis. Cochrane Database Syst Rev (12):CD004969, 2013. doi: 10.1002/14651858.CD004969.pub3. Update in: Cochrane Database Syst Rev 2:CD004969, 2016.
Geriatrics Essentials: Toothache
Older patients are more prone to caries of the root surfaces, usually because of gingival recession and medication-induced xerostomia. Periodontitis often begins in young adulthood; if untreated, tooth pain and loss are common in old age.
Key Points
Most toothache involves dental caries or its complications (eg, pulpitis, abscess).
Symptomatic treatment and dental referral are usually adequate.
Antibiotics are given if signs of an abscess, necrotic pulp, or more severe conditions are present and if same-day dental care is not available.
Very rare but serious complications include extension of dental infection to the floor of the mouth or to the cavernous sinus.
Dental infections rarely cause sinusitis, but sinus infection may cause pain perceived as originating in the teeth.






