


Basal cell carcinoma is a superficial, slowly growing papule or nodule that derives from certain epidermal cells. Basal cell carcinomas arise from keratinocytes near the basal layer, which are sometimes called basaloid keratinocytes. Metastasis is rare, but local growth can be highly destructive. Diagnosis is by biopsy. Treatment depends on the tumor’s characteristics and may involve curettage and electrodesiccation, surgical excision, cryosurgery, topical chemotherapy, or, occasionally, radiation therapy or medications.
(See also Overview of Skin Cancer.)
Basal cell carcinoma is the most common type of skin cancer, with approximately 2 million new cases yearly in the United States (1). It is most common among people with light skin with a history of sun exposure and is very rare in people with dark skin.
Basal cell carcinomas are also associated with genetic syndromes and may arise in a nevus sebaceus (nevus sebaceous). Xeroderma pigmentosum represents an inherited defect in DNA repair that can result in nonmelanoma skin cancer and in melanoma. Basal cell nevus syndrome (Gorlin syndrome) is an autosomal dominant disorder that results in multiple basal cell carcinomas as well as in medulloblastomas, meningiomas, breast cancers, non-Hodgkin lymphomas, and ovarian cancers. Bazex syndrome is a rare genodermatosis that can result in the early onset of multiple basal cell carcinomas.

DR P. MARAZZI / SCIENCE PHOTO LIBRARY
General reference
1. Asgari MM, Moffet HH, Ray GT, Quesenberry CP: Trends in Basal Cell Carcinoma Incidence and Identification of High-Risk Subgroups, 1998-2012. JAMA Dermatol 151(9):976-981, 2015. doi: 10.1001/jamadermatol.2015.1188
Symptoms and Signs of Basal Cell Carcinoma
The clinical manifestations and biologic behavior of basal cell carcinomas are highly variable.
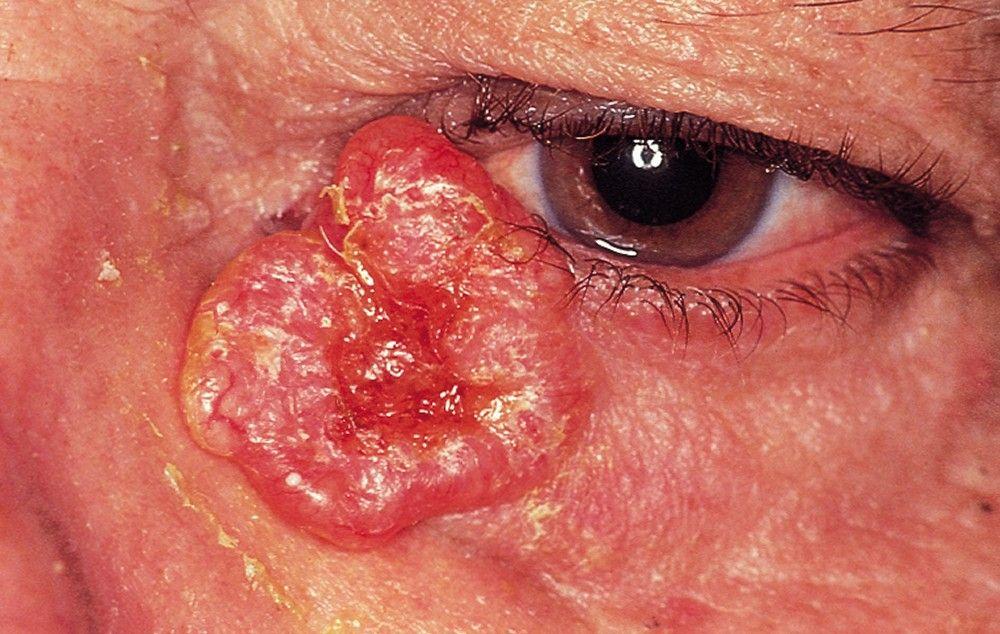
Most commonly, the carcinoma begins as a shiny papule, enlarges slowly, and, after a few months or years, shows a shiny, pearly border with prominent engorged vessels (telangiectases) on the surface and a central dell or ulcer. Recurrent crusting or bleeding is not unusual. Commonly, the carcinomas may alternately crust and heal, which may unjustifiably decrease patient and physician concerns about the seriousness of the lesion.
There are several types of basal cell carcinomas. The most common types are
Nodular (approximately 60% of basal cell carcinomas): These types are small, shiny, firm, almost translucent to pink nodules with telangiectases, usually on the face or other sun-exposed areas. Ulceration and crusting are common.
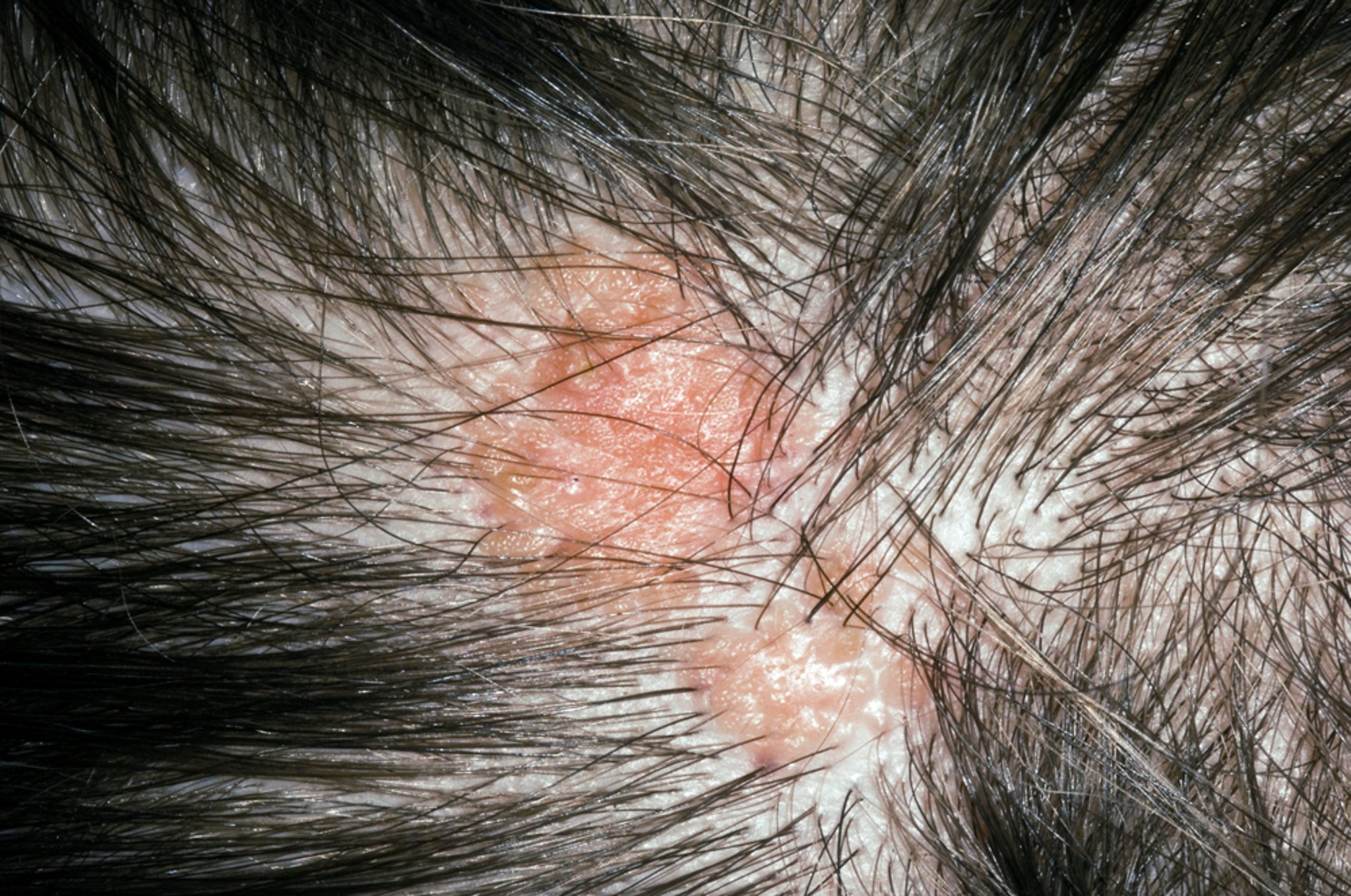
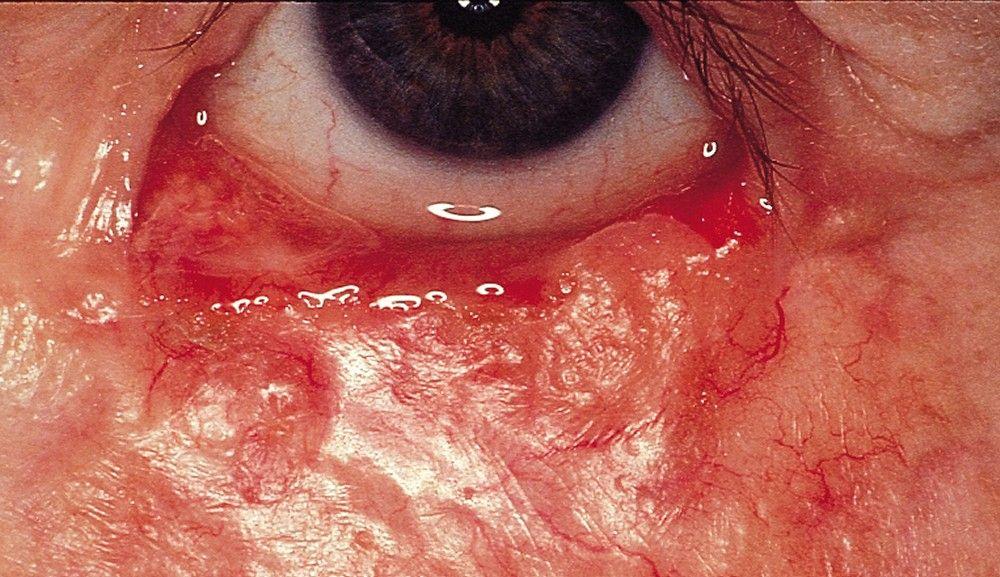
Superficial (approximately 30%): These types are red or pink, marginated, thin papules or plaques, commonly on the trunk, that can be similar to psoriasis or localized dermatitis.
Morpheaform (5 to 10%): These types are flat, scarlike, indurated plaques that can be flesh-colored or light red and have vague borders.
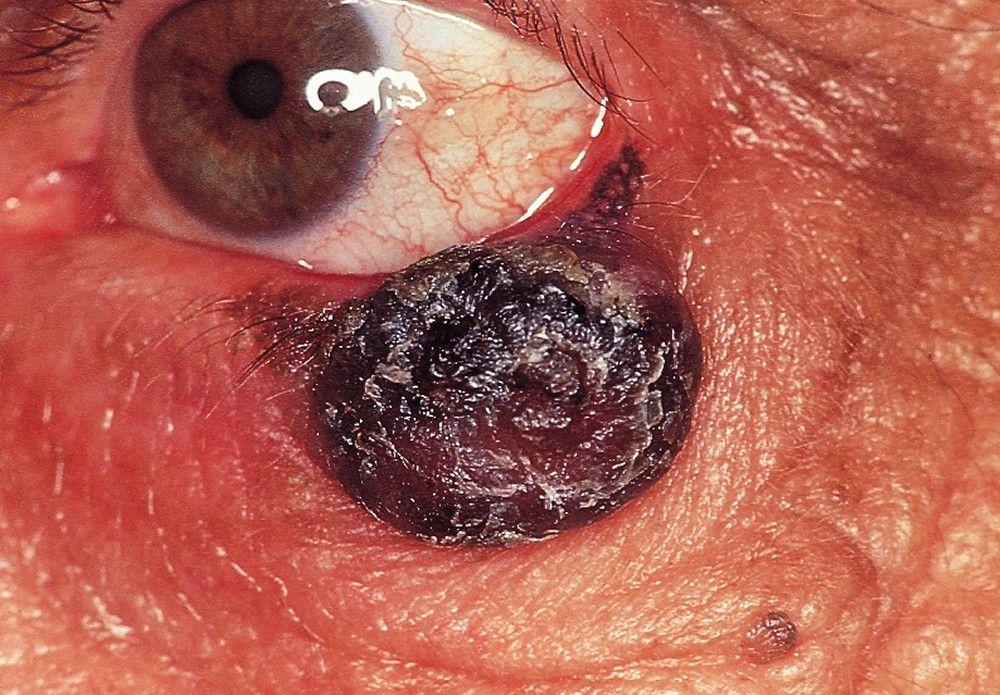
Other: Other types are possible. Nodular and superficial basal cell carcinomas can produce pigment (sometimes called pigmented basal cell carcinomas).
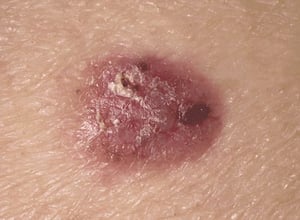
Photo provided by Thomas Habif, MD.

© Springer Science+Business Media

RICHARD USATINE MD / SCIENCE PHOTO LIBRARY
© Springer Science+Business Media
© Springer Science+Business Media

BSIP, GIRAND / SCIENCE PHOTO LIBRARY


Photo provided by Thomas Habif, MD.

© Springer Science+Business Media


RICHARD USATINE MD / SCIENCE PHOTO LIBRARY

© Springer Science+Business Media

© Springer Science+Business Media


BSIP, GIRAND / SCIENCE PHOTO LIBRARY
Diagnosis of Basal Cell Carcinoma
Biopsy
Diagnosis of basal cell carcinoma is by biopsy and histologic examination.
Treatment of Basal Cell Carcinoma
Usually with local methods
Treatment of basal cell carcinoma should be done by a specialist.
Recurrent or incompletely treated cancers, large cancers, cancers at high-risk or recurrence-prone sites (eg, head and neck), and morphea-like cancers with vague borders are often treated with Mohs microscopically controlled surgery, in which tissue borders are progressively excised until specimens are tumor-free (as determined by microscopic examination during surgery).
Treatment references
1. Basset-Séguin N, Hauschild A, Kunstfeld R, et al: Vismodegib in patients with advanced basal cell carcinoma: Primary analysis of STEVIE, an international, open-label trial. Eur J Cancer 86:334-348, 2017. doi: 10.1016/j.ejca.2017.08.022
2. Lear JT, Migden MR, Lewis KD, et al: Long-term efficacy and safety of sonidegib in patients with locally advanced and metastatic basal cell carcinoma: 30-month analysis of the randomized phase 2 BOLT study. J Eur Acad Dermatol Venereol 32(3):372-381, 2018. doi: 10.1111/jdv.14542
3. Stratigos AJ, Sekulic A, Peris K, et al: Cemiplimab in locally advanced basal cell carcinoma after hedgehog inhibitor therapy: An open-label, multi-centre, single-arm, phase 2 trial. Lancet Oncol 22(6):848–857, 2021. doi: 10.1016/S1470-2045(21)00126-1
Prognosis for Basal Cell Carcinoma
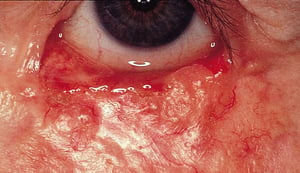
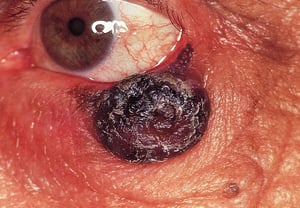
Basal cell carcinomas rarely metastasize but may invade healthy tissues. Rarely, patients die because the carcinoma invades or impinges on underlying vital structures or orifices (eg, eyes, ears, mouth, bone, dura mater).
Almost 25% of patients with a history of basal cell carcinoma develop a new basal cell cancer within 5 years of the original carcinoma. Consequently, patients with a history of basal cell carcinoma should be seen annually for a skin examination.
Prevention of Basal Cell Carcinoma
Because basal cell carcinoma is associated with ultraviolet (UV) exposure, a number of measures are recommended to limit exposure.
Sun avoidance: Seeking shade, minimizing outdoor activities between 10 AM and 4 PM (when sun's rays are strongest), and avoiding sunbathing and the use of tanning beds
Use of protective clothing: Long-sleeved shirts, pants, and broad-brimmed hats
Use of sunscreen: At least sun protection factor (SPF) 30 with broad-spectrum UVA/UVB protection, used as directed (ie, reapplied every 2 hours and after swimming or sweating); should not be used to prolong sun exposure
Key Points
Basal cell carcinomas, the most common skin cancers, are particularly common on sun-exposed skin among people with light skin.
Consider the diagnosis with typical lesions (eg, shiny, slowly enlarging papule, often with a shiny, pearly border) and lesions that bleed easily or alternately crust and heal.
Refer patients to specialists for treatment, usually by locally destructive methods.






