


Oral cancer refers to cancer occurring between the vermilion border of the lips and the junction of the hard and soft palates or the posterior one third of the tongue. Over 95% of people with oral squamous cell carcinoma smoke tobacco, drink alcohol, or both. Early, curable lesions are rarely symptomatic; thus, preventing fatal disease requires early detection by screening. Treatment is with surgery, radiation, or both, although surgery plays a larger role in the treatment of most oral cavity cancer. The overall 5-year survival rate (all sites and stages combined) is 50%.
(See also Overview of Head and Neck Tumors.)
Oral squamous cell carcinoma affects about 35,000 people in the US each year (1). In the US, 3% of cancers in men and 2% in women are oral squamous cell carcinomas, most of which occur after age 50. As with most head and neck sites, squamous cell carcinoma is the most common oral cancer.
The chief risk factors for oral squamous cell carcinoma are
Smoking (especially > 2 packs/day)
Alcohol use
Risk increases dramatically when alcohol use exceeds 6 oz of distilled liquor, 15 oz of wine, or 36 oz of beer/day. The combination of heavy smoking and alcohol abuse is estimated to raise the risk 100-fold in women and 38-fold in men.
Squamous cell carcinoma of the tongue may also result from any chronic irritation, such as dental caries, overuse of mouthwash, chewing tobacco, or the use of betel quid. Oral human papillomavirus (HPV), typically acquired via oral-genital contact, may have a role in the etiology of some oral cancers; however, HPV is identified in oral cancer much less often than it is in oropharyngeal cancer, and its presence in resected tissue does not necessarily imply causation.
About 40% of intraoral squamous cell carcinomas begin on the floor of the mouth or on the lateral and ventral surfaces of the tongue. About 38% of all oral squamous cell carcinomas occur on the lower lip; these are usually solar-related cancers on the external surface.
General reference
1. Siegel RL, Miller KD, Jemal A: Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7-30. doi:10.3322/caac.21590
Symptoms and Signs of Oral Squamous Cell Carcinoma
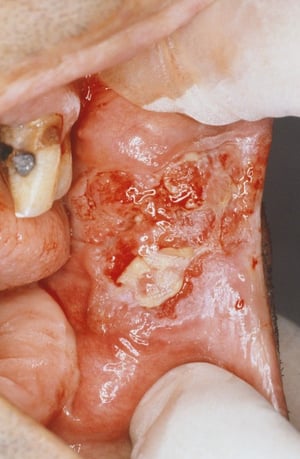
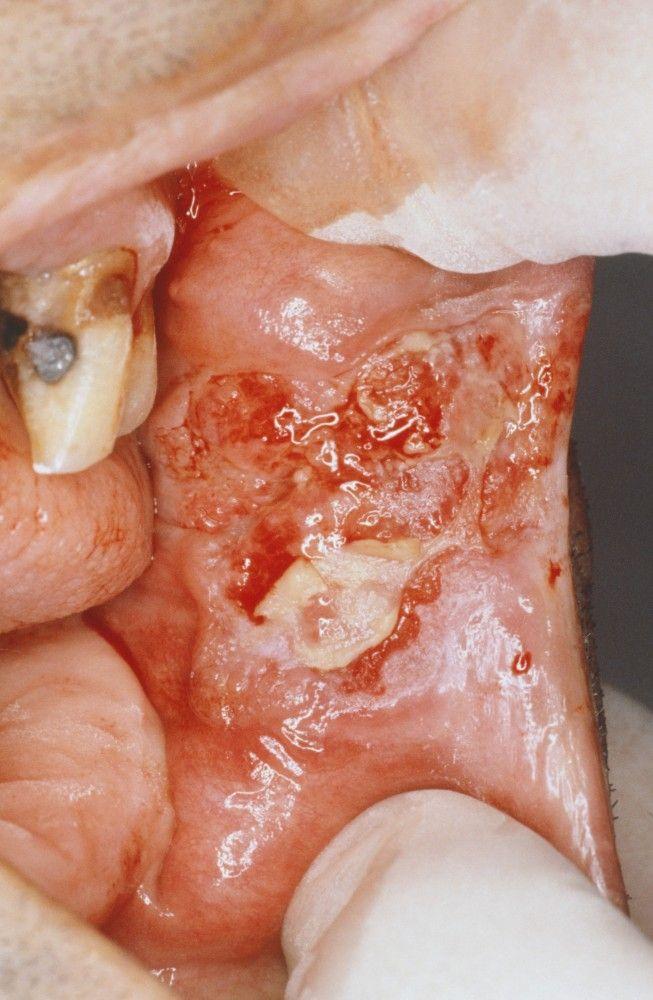
Oral lesions are asymptomatic initially, highlighting the need for oral screening. Most dental professionals carefully examine the oral cavity and oropharynx during routine care and may do a brush biopsy of abnormal areas. The lesions may appear as areas of erythroplakia or leukoplakia and may be exophytic or ulcerated. Cancers are often indurated and firm with a rolled border. As the lesions increase in size, pain, dysarthria, and dysphagia may result.
CLINICA CLAROS/SCIENCE PHOTO LIBRARY

Image provided by Jonathan A. Ship, DMD.
Image provided by Jonathan A. Ship, DMD.

CLINICA CLAROS/SCIENCE PHOTO LIBRARY


Image provided by Jonathan A. Ship, DMD.

Image provided by Jonathan A. Ship, DMD.
Diagnosis of Oral Squamous Cell Carcinoma
Biopsy
Endoscopy to detect second primary cancer
Chest CT or x-ray and CT of head and neck
Any suspicious areas should be biopsied. Incisional or brush biopsy can be done depending on the surgeon's preference. Direct laryngoscopy and esophagoscopy are done in all patients with oral cavity cancer to exclude a simultaneous second primary cancer. Head and neck CT usually is done and a chest CT or x-ray is done; however, as in most sites in the head and neck, PET/CT has begun to play a larger role in the evaluation of patients with oral cavity cancer. (See table Staging of Lip and Oral Cancer.)
Prognosis for Oral Squamous Cell Carcinoma
If carcinoma of the tongue is localized (no lymph node involvement), 5-year survival is > 75%. For localized carcinoma of the floor of the mouth, 5-year survival is 75%. Lymph node metastasis decreases survival rate by about half. Metastases reach the regional lymph nodes first and later the lungs.
For lower lip lesions, 5-year survival is 90%, and metastases are rare. Carcinoma of the upper lip tends to be more aggressive and metastatic.
Treatment of Oral Squamous Cell Carcinoma
Surgery, with postoperative radiation or chemoradiation as needed
For most oral cavity cancers, surgery is the initial treatment of choice. Radiation or chemoradiation is added postoperatively if disease is more advanced or has high-risk histologic features. (See also the National Cancer Institute’s summary Lip and Oral Cavity Cancer Treatment.)
Selective neck dissection is indicated if the risk of nodal disease exceeds 15 to 20%. Although there is no firm consensus, neck dissections are typically done for any lesion with a depth of invasion > about 3.5 mm.
Routine surgical reconstruction is the key to reducing postoperative oral disabilities; procedures range from local tissue flaps to free tissue transfers. Speech and swallowing therapy may be required after significant resections.
Radiation therapy is an alternative treatment. Chemotherapy is not used routinely as primary therapy but is recommended as adjuvant therapy along with radiation in patients with advanced nodal disease.
Treatment of squamous cell carcinoma of the lip is surgical excision with reconstruction to maximize postoperative function. When large areas of the lip exhibit premalignant change, the lip can be surgically shaved, or a laser can remove all affected mucosa. Mohs surgery can be used. Thereafter, appropriate sunscreen application is recommended.
Key Points
The chief risk factors for oral squamous cell carcinoma are heavy smoking and alcohol use.
Oral cancer is sometimes asymptomatic initially, so oral screening (typically by dental professionals) is useful for early diagnosis.
Do direct laryngoscopy and esophagoscopy to exclude a simultaneous second primary cancer.
Once cancer is confirmed, do head and neck CT, a chest imaging (CT or x-ray), and sometimes PET/CT.
Initial treatment is usually surgical.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
National Cancer Institute’s Summary: Lip and Oral Cavity Cancer Treatment






