



Epistaxis refers to bleeding from the nasal cavity and may have an anterior or posterior origin. Epistaxis that is not controlled by digital compression (ie, pressure applied on the external walls of the nose by a clinician or caregiver for a minimum of 10 minutes, but often longer) requires immediate further management. In lower-resource settings where commercial nasal clips are not available for treating epistaxis, a makeshift nasal clip may be fashioned from tongue depressors to control bleeding.
Indications for Treating Anterior Epistaxis With Makeshift Nasal Clip
Anterior bleeding from a clearly visible site
Failure of digital nasal compression to stop nasal bleeding
Lack of availability of commercial nasal clips
Contraindications to Treating Anterior Epistaxis With Makeshift Nasal Clip
Absolute contraindications
Inability to visualize the source of bleeding
This procedure should only be used when a bleeding site is conspicuous on initial physical examination. If bleeding is persistent and a clear bleeding site is visualized, anterior cautery may be attempted as a next step. Urgent specialist consultation is advised if a posterior bleed is suspected, or if there is a history of facial or skull base trauma.
Relative contraindications
Severe nasal septal deviation toward the bleeding side
Complications of Treating Anterior Epistaxis With Makeshift Nasal Clip
Mechanical injury to the septum and lateral wall cartilage
Pressure necrosis
Rebleeding when clip is removed
Equipment for Treating Anterior Epistaxis With Makeshift Nasal Clip
Gloves, mask, and gown
Gown or drapes for patient
Suction source and Frazier-tip suction of varying sizes with integrated finger control to regulate the strength of the suction
Sterile gauze sponges
Emesis basin
Chair with headrest or an ear, nose, and throat (ENT) specialist's chair
Light source and headlamp with adjustable narrow beam
Nasal speculum
Tongue depressors
Topical anesthetic/vasoconstrictor mixture (eg, 4% cocaine, 1% tetracaine, or 4% lidocaine plus 0.5% oxymetazoline) or topical vasoconstrictor alone (eg, 0.5% oxymetazoline spray)
Cotton swabs or pledgets
Additional Considerations for Treating Anterior Epistaxis With Makeshift Nasal Clip
Ask about use of anticoagulant or antiplatelet medications.
Perform a complete blood count (CBC), prothrombin time (PT), and partial thromboplastin time (PTT) if there are symptoms or signs of a bleeding disorder or the patient has severe or recurrent epistaxis.
Relevant Anatomy for Treating Anterior Epistaxis With Makeshift Nasal Clip
The submucosal vascular plexus supplying the anterior nasal septum is the most common site of anterior epistaxis. This plexus consists of branches from the anterior ethmoid artery, sphenopalatine artery, greater palatine artery, and septal branch of the superior labial artery.
Positioning for Treating Anterior Epistaxis With Makeshift Nasal Clip
The patient should sit upright in the sniffing position with the head extended, preferably in an ENT specialist's chair. The patient's occiput should be supported to prevent sudden backward movement. The patient's nose should ideally be level with the physician's eyes.
The patient should hold the emesis basin to collect any continued bleeding or emesis (eg, of swallowed blood)
Step-by-Step Description of Treating Anterior Epistaxis With Makeshift Nasal Clip
Have the patient gently blow the nose to remove clots. Alternatively, suction the nasal passageway carefully.
Insert a nasal speculum with your index finger resting against the patient's nose and the handle parallel to the floor (so the blades open vertically).
Gently open the speculum and examine the nose using a bright headlamp or directed light source, which allows the clinician to keep one hand free for manipulating suction or other instruments during the examination.
Use a Frazier-tip suction to remove any blood and clots obscuring the view.
Inspect for blood flowing from the area of the anterior septum vascular plexus, and for blood flowing from the back of the nose.
Apply a topical vasoconstrictor/anesthetic mixture: Place approximately 3 mL of 4% cocaine solution or 4% lidocaine with oxymetazoline in a small medicine cup and soak 2 or 3 cotton pledgets with the solution and insert them into the nose, stacked vertically (or spray in a topical vasoconstrictor such as oxymetazoline and place pledgets containing only topical anesthetic).
Leave the topical medications in place for 10 to 15 minutes to stop or reduce the bleeding, provide anesthesia, and reduce mucosal swelling.
Obtain four tongue depressors and some adhesive tape. Take two tongue depressors, and place one of them parallel to and on top of the other. Repeat this step for the other two tongue depressors.
Next, place the two paired tongue depressors with a small gap (approximately the width of the nasal bridge) between them. Secure the tongue depressors together in the middle using adhesive tape, ensuring that the gap between the tongue depressors remains consistent. The finished clip must be fashioned into a wedge- or V-shape.
Position the makeshift clip over the nasal bridge, ensuring that the tongue depressors apply gentle pressure to the sides of the nose, compressing the nasal alae against the septum (to form an inverted V-shape).
Leave the clip in place for at least 15 minutes before re-examination to determine whether bleeding has stopped.

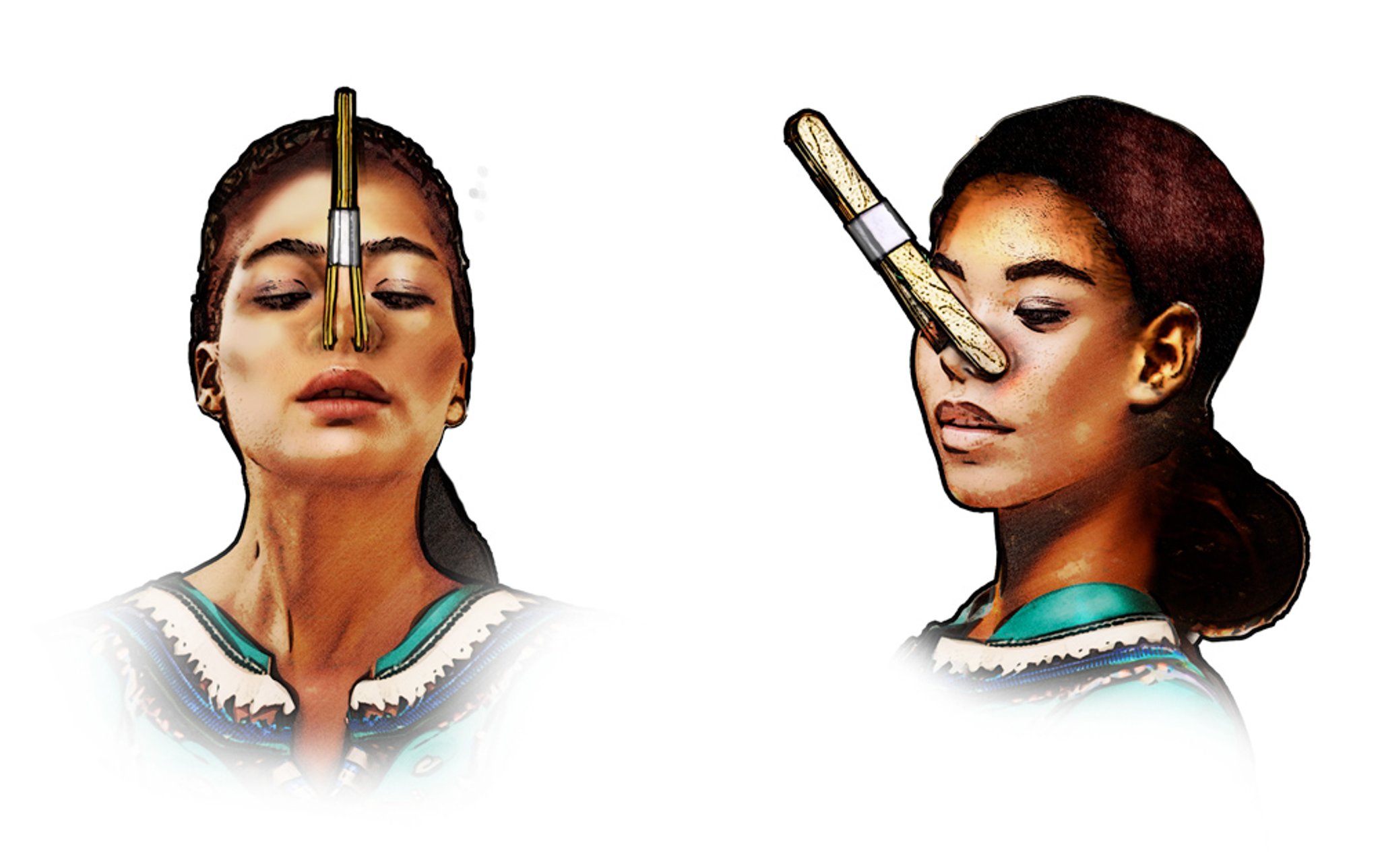
Four tongue depressors can be taped together to fashion a makeshift nasal clip to provide pressure to the nasal alae. This external pressure can compress the plexus of vessels in the anterior interior septum to treat anterior epistaxis.
Copyright © 2023 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
Aftercare for Treating Anterior Epistaxis With Makeshift Nasal Clip
Advise the patient not to take aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs) for 4 days after treatment of epistaxis.
Warnings and Common Errors When Treating Anterior Epistaxis With Makeshift Nasal Clip
Do not open the nasal speculum laterally or use in an unsupported manner. (Brace a finger of the hand holding the speculum on the patient's cheek or nose.)
The makeshift clip may not apply adequate or consistent pressure to the bleeding site, potentially failing to control the epistaxis effectively.
The clip may easily become dislodged, especially if not secured properly
The patient must be cautioned to examine for signs and symptoms of pressure necrosis (eg, pain, erythema/purpura, or eschar formation).
Tips and Tricks for Treating Anterior Epistaxis With Makeshift Nasal Clip
Elevating the patient's chair to eye level puts less strain on the clinician's back compared to bending down.
Advise the patient that if bleeding recurs, the nostrils should be pinched closed for 20 minutes without interruption. Applying oxymetazoline nasal spray before pinching the nostrils may help control bleeding. If this does not stop the bleeding or if the bleeding is profuse, the patient should return to the emergency department.
To prevent dislodgement, position the clip on the lower edge of the nose such that the bound ends on the upper surface point away from the eyes, or at a 30-45 degree angle (directed away from the face).
Drug Information for the Topic





