


Rapidly progressive glomerulonephritis (RPGN), a type of nephritic syndrome, is a pathologic diagnosis accompanied by extensive glomerular crescent formation (ie, >50% of sampled glomeruli contain crescents, which can be seen in a biopsy specimen); if left untreated, RPGN progresses to end-stage kidney disease over weeks to months. It is relatively uncommon, affecting 10 to 15% of patients with glomerulonephritis, and occurs predominantly in patients 20 to 50 years. Types and causes are classified by findings using immunofluorescence microscopy and serologic tests (eg, anti-glomerular basement membrane [GBM] antibody, anti-neutrophil cytoplasmic antibody [ANCA]—see table Classification of Rapidly Progressive Glomerulonephritis Based on Immunofluorescence Microscopy).
Antiglomerular basement membrane antibody disease
Antiglomerular basement membrane (GBM) antibody disease is an autoimmune glomerulonephritis and accounts for up to 10% of RPGN cases. It may arise when respiratory exposures (eg, cigarette smoke, viral upper respiratory infection) or some other stimulus exposes alveolar capillary collagen, triggering formation of anticollagen antibodies. The anticollagen antibodies cross-react with GBM, fixing complement and triggering a cell-mediated inflammatory response in the kidneys and usually the lungs.
The term Goodpasture syndrome refers to a combination of glomerulonephritis and alveolar hemorrhage in the presence of anti-GBM antibodies. Glomerulonephritis without alveolar hemorrhage in the presence of anti-GBM antibodies is called anti-GBM glomerulonephritis. Immunofluorescent staining of renal biopsy tissue demonstrates linear IgG deposits.
Immune complex RPGN
Immune complex RPGN complicates numerous infectious and systemic rheumatic diseases and also occurs with other primary glomerulopathies.
Immunofluorescent staining demonstrates nonspecific granular immune deposits. The condition accounts for up to 40% of RPGN cases. Pathogenesis is usually unknown.
Pauci-immune RPGN
Pauci-immune RPGN is distinguished by the absence of immune complex or complement deposition on immunofluorescent staining. It constitutes up to 50% of all RPGN cases. Almost all patients have elevated antineutrophil cytoplasmic antibodies (ANCAs), usually antiproteinase 3-ANCA or myeloperoxidase-ANCA, and systemic vasculitis.
Double-antibody disease
Double-antibody disease occurs with the presence of anti-GBM and ANCA antibodies. It is rare.
Idiopathic RPGN
Idiopathic cases are rare. They include patients with either of the following:
Immune complexes but no obvious cause such as infection, systemic rheumatic disease, or glomerular disorder
Pauci-immune features but absence of ANCA antibodies
Symptoms and Signs of RPGN
Manifestations are usually insidious, with weakness, fatigue, fever, nausea, vomiting, anorexia, arthralgia, and abdominal pain. Some patients present similarly to those with postinfectious glomerulonephritis, with abrupt-onset hematuria. About 50% of patients have edema and a history of an acute influenza-like illness within 4 weeks of onset of renal failure, usually followed by severe oliguria. Nephrotic syndrome is present in 10 to 30%. Hypertension is uncommon and rarely severe. Patients with anti-GBM antibody disease may have pulmonary hemorrhage, which can manifest with hemoptysis or be detectable only by findings suggestive of diffuse alveolar infiltrates on lung imaging (pulmonary-renal syndrome or diffuse alveolar hemorrhage syndrome).
Diagnosis of RPGN
Progressive renal failure over weeks to months
Nephritic urinary sediment
Serologic testing
Serum complement levels
Renal biopsy
Diagnosis is suggested by acute kidney injury in patients with hematuria and dysmorphic red blood cells (RBCs) or RBC casts. Testing includes serum creatinine, urinalysis, complete blood count (CBC), serologic tests, and renal biopsy. Diagnosis is usually by serologic tests and renal biopsy.
Serum creatinine is almost always elevated.
Urinalysis shows hematuria is always present, and RBC casts are usually present. Telescopic sediment (ie, sediment with multiple elements, including white blood cells [WBCs]; dysmorphic RBCs; and WBC, RBC, granular, waxy, and broad casts) is common.
On CBC, anemia is usually present, and leukocytosis is common.
Serologic testing should include anti-GBM antibodies (anti-GBM antibody disease); antistreptolysin O antibodies, anti-DNA antibodies, or cryoglobulins (immune complex RPGN); and antineutrophil cytoplasmic antibodies (ANCA) titers (pauci-immune RPGN).
Complement measurement (serum C3 and C4) may be useful in suspected immune complex RPGN because hypocomplementemia is common.
Early renal biopsy is essential. The feature common to all types of RPGN is focal proliferation of glomerular epithelial cells, sometimes interspersed with numerous neutrophils, that forms a crescentic cellular mass (crescents) and that fills Bowman space in > 50% of glomeruli. The glomerular tuft usually appears hypocellular and collapses. Necrosis within the tuft or involving the crescent may occur and may be the most prominent abnormality. In such patients, histologic evidence of vasculitis should be sought.

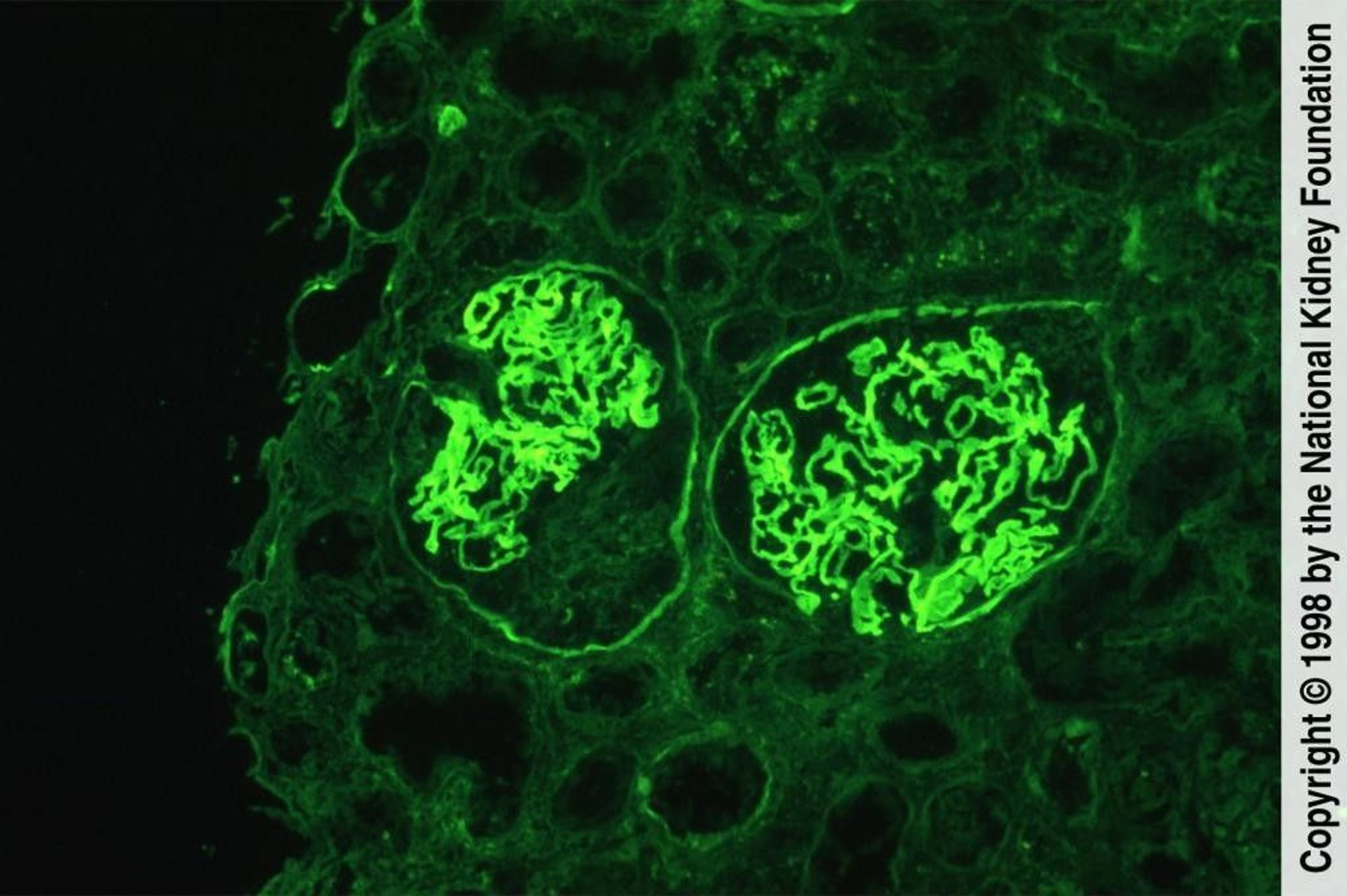
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
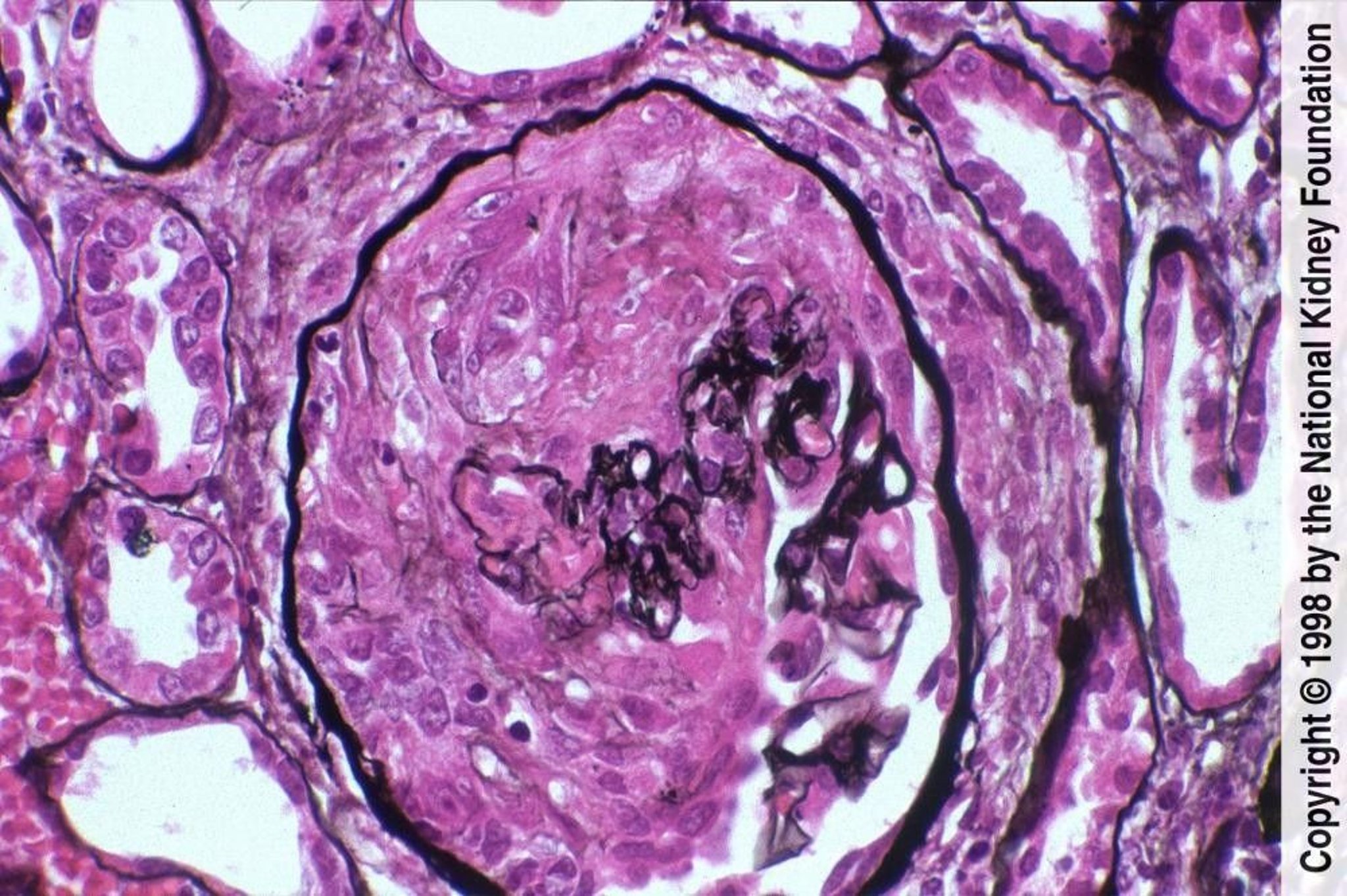
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Immunofluorescence microscopy findings differ for each type:
In anti-GBM antibody disease, linear or ribbon-like deposition of IgG along the GBM is most prominent and is often accompanied by linear and sometimes granular deposition of C3.
In immune complex RPGN, immunofluorescence reveals diffuse, irregular mesangial IgG and C3 deposits.
In pauci-immune RPGN, immune staining and deposits are not detected. However, fibrin occurs within the crescents, regardless of the fluorescence pattern.
In double antibody RPGN, linear staining of the GBM is present.
In idiopathic RPGN, some patients have immune complexes and others have absence of immune staining and deposits.
Treatment of RPGN
Corticosteroids
Plasma exchange
Treatment varies by disease type, although no regimens have been rigorously studied. Therapy should be instituted early, ideally when serum creatinine is < 5 mg/dL (442 micromol/L) and before the biopsy shows crescentic involvement of all glomeruli or organizing crescents as well as fibrotic interstitium and atrophic tubules. Even patients with kidney involvement and higher creatinine levels should be aggressively treated if they do not require immediate renal replacement therapy. Treatment becomes less effective as these features become more prominent and may be harmful in some patients (eg, older patients, patients with infection).
> 3 years in 50% of patients (1, 2).
may be dosed at 375 mg/m2 IV per week for 4 weeks as used in the RAVE trial (formal title: Rituximab in ANCA-Associated Vasculitis; [2
Plasma exchange (daily 3- to 4-L exchanges for 14 days) is recommended for anti-GBM antibody disease. Plasma exchange may also be considered for immune complex and pauci-immune ANCA-associated RPGN with pulmonary hemorrhage or severe renal dysfunction on presentation (serum creatinine > 5 to 7 mg/dL [442 to 618.8 micromol/L] or dialysis dependency), but its use remains controversial. Plasma exchange is thought to rapidly remove free antibody, intact immune complexes, and mediators of inflammation (eg, fibrinogen, complement). While some evidence suggested that plasma exchange improved short-term kidney outcomes, a subsequent randomized trial did not show that it reduced the incidence of death or end-stage kidney disease (3).
renal replacement therapy, even if creatinine levels were elevated above 5 to 7 mg/dL (442 to 618.8 micromol/L; [4]).
Kidney transplantation is effective for all types, but disease may recur in the graft; risk diminishes with time. In anti-GBM antibody disease, the anti-GBM titers should be undetectable for at least 12 months before transplantation. For patients with pauci-immune RPGN, disease activity should be quiescent for at least 6 months before transplantation; ANCA titers do not need to be suppressed.
Treatment references
1. Ponticelli C, Altieri P, et alJ Am Soc Nephrol 9(3):444, 1998. doi: 10.1681/ASN.V93444
2. Jones RB, Cohen Tervaert JW, Hauser TN Engl J Med 363:211-220, 2010. doi: 10.1056/NEJMoa0909169
3. Walsh M, Merkel PA, Peh C-A, et al: Plasma exchange and glucocorticoids in severe ANCA-associated vasculitis. N Engl J Med 382(7):621-631, 2020. doi: 10.1056/NEJMoa1803537
4. Levy JB, Turner AN, Rees AJ, et al: Long-term outcome of anti-glomerular basement membrane antibody disease treated with plasma exchange and immunosuppression. Ann Intern Med 134(11):1033-1042, 2001. doi: 10.7326/0003-4819-134-11-200106050-00009
Prognosis for RPGN
Spontaneous remission is rare, and 80 to 90% of untreated patients progress to end-stage kidney disease within 6 months. Prognosis improves with early treatment.
Favorable prognostic factors include RPGN caused by the following:
Anti-GBM disease if treated early, especially when treated before oliguria occurs and when creatinine level is < 7 mg/dL (618.8 micromol/L)
Unfavorable prognostic factors include the following:
Age > 60 years
Oliguric renal failure
Higher serum creatinine level
Circumferential crescents in > 75% of glomeruli
Pauci-immune RPGN
About 30% of patients with pauci-immune RPGN do not respond to treatment; among nonresponders, about 40% require dialysis, and 33% die within 4 years. In contrast, among patients who respond to treatment, < 20% of patients require dialysis, and about 3% die.
Patients with double-antibody disease appear to have a renal prognosis somewhat better than patients with only anti-GBM antibody disease and worse than patients with pauci-immune disease.
Patients who recover normal renal function after RPGN demonstrate residual histologic changes principally in glomeruli, consisting chiefly of hypercellularity, with little or no sclerosis within the glomerular tuft or the epithelial cells and minimal fibrosis of the interstitium.
Death is usually due to infectious or cardiac causes, providing that a uremic death is prevented by dialysis.
Key Points
Consider rapidly progressive glomerulonephritis if patients have acute kidney injury with hematuria and dysmorphic RBCs or RBC casts, particularly with subacute constitutional or nonspecific symptoms (eg, fatigue, fever, anorexia, arthralgia, abdominal pain).
Evaluate with serologic tests and early renal biopsy.
Consider kidney transplantation after disease activity is controlled.






