


Cervical insufficiency (formerly called cervical incompetence) is painless cervical dilation resulting in second-trimester pregnancy loss. Transvaginal cervical ultrasonography during the second trimester may be used to assess risk or to monitor. Treatment is reinforcement of the cervix with suture material (cerclage).
Cervical insufficiency is painless cervical dilation resulting in second-trimester pregnancy loss in the absence of clinical contractions, labor, or both. Estimated incidence varies greatly (1/100 to 1/2000).
Etiology of Cervical Insufficiency
The cause of cervical insufficiency is not well-understood but seems to involve some combination of structural abnormalities and biochemical factors (eg, inflammation, infection); these factors may be acquired or genetic.
Risk factors
Most women with cervical insufficiency do not have known risk factors; however, the following risk factors have been identified:
Congenital disorders of collagen synthesis (eg, Ehlers-Danlos syndrome)
Prior cone biopsy (particularly when ≥ 1.7 to 2.0 cm of the cervix was removed) or trachelectomy
Prior deep cervical lacerations (usually secondary to vaginal or cesarean delivery)
Prior excessive or rapid dilation with instruments (now uncommon)
Müllerian duct defects (eg, bicornuate or septate uterus)
≥ 2 prior fetal losses during the second trimester
Recurrence
Overall risk of recurrence of fetal loss due to cervical insufficiency is probably ≤ 30%, leading to the question of how large a role fixed structural abnormalities have. Risk is greatest for women with ≥ 2 prior second-trimester fetal losses.
Symptoms and Signs of Cervical Insufficiency
Cervical insufficiency is often asymptomatic until preterm delivery occurs. Some women have earlier symptoms, such as vaginal pressure, vaginal bleeding or spotting, nonspecific abdominal or lower back pain, or vaginal discharge.
The cervix may be soft, effaced, or dilated.
Diagnosis of Cervical Insufficiency
Transvaginal ultrasonography at 15 to 16 weeks through 23 to 24 weeks for women with symptoms or risk factors
Usually, cervical insufficiency is not identified until after the patient has had at least 1 delivery after 15 weeks (1).
The diagnosis of cervical insufficiency is suspected in patients with risk factors or characteristic symptoms or signs.
If there is uncertainty about the clinical suspicion of cervical insufficiency, patients may be monitored starting at 15 to 16 weeks through 23 to 24 weeks with serial transvaginal ultrasonography to measure cervical length.
Suggestive ultrasonographic findings include
Cervical shortening to ≤ 2.5 cm with history of cervical insufficiency
Cervical dilation
Protrusion of fetal membranes into the cervical canal
Diagnosis reference
1. American College of Obstetricians and Gynecologists (ACOG): ACOG Practice Bulletin No.142: Cerclage for the management of cervical insufficiency. Obstet Gynecol 123 (2 Pt 1):372–379, 2014. doi: 10.1097/01.AOG.0000443276.68274.cc
Treatment of Cervical Insufficiency
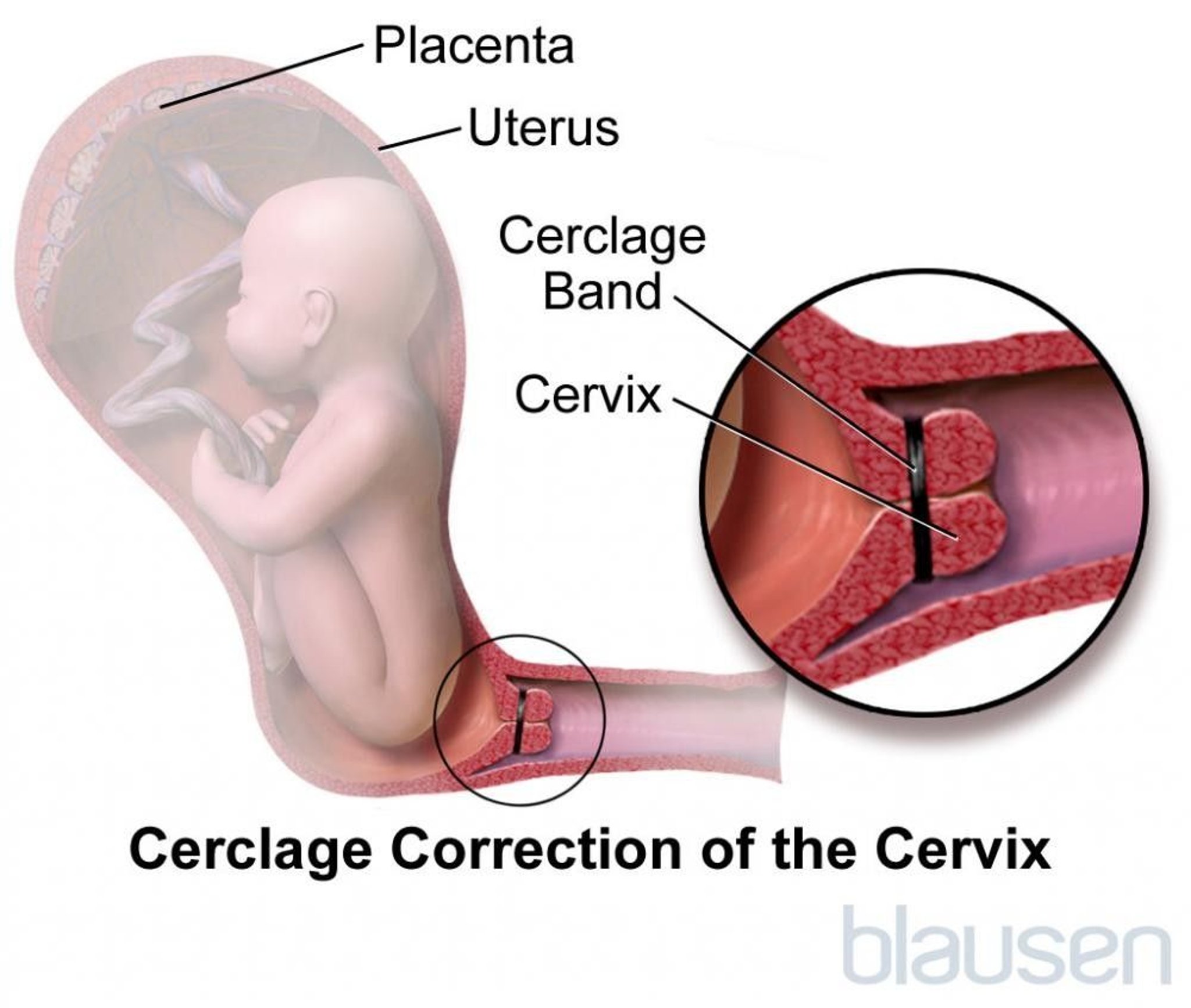
Cervical cerclage
Cervical cerclage is reinforcement of the cervical ring with nonabsorbable suture material. Cerclage appears to prevent preterm delivery in patients with ≥ 2 prior second-trimester fetal losses. Cerclage may be indicated based on history alone (history-indicated cerclage), ultrasonographic findings plus history (ultrasound-indicated cerclage [1]), or physical examination where dilation is present.
History-indicated cerclage placement is usually performed in patients with a history that strongly suggests cervical insufficiency, typically a history ≥ 2 deliveries at 15 to 24 weeks. In these patients, cerclage is done during the first trimester or may be done before pregnancy.
For patients with an uncertain risk of cervical insufficiency who are monitored with serial ultrasonography to measure cervical length, a cerclage is typically placed if length is < 2.5 cm before 24 weeks. Restricting cerclage to such patients does not appear to increase risk of preterm delivery and avoids unnecessary cerclage procedures. Evidence suggests that cerclage may help prevent preterm delivery in women who have a history of idiopathic preterm delivery and whose cervix is < 2.0 to 2.5 cm long (2).
If cervical dilation occurred and is confirmed with physical examination, cerclage may be placed in selected patients prior to 24 weeks gestation. Cerclage may be considered if cerclage is technically feasible and as long as signs of chorioamnionitis, bleeding, or labor are not present. Such cases, though, can be controversial and rely on clinical judgment and shared decision-making between patient and physician.

If preterm labor is suspected after 22 to 23 weeks, corticosteroids (to accelerate fetal lung maturation) and modified activity (modified rest) may also be indicated (2).
Treatment references
1. American College of Obstetricians and Gynecologists (ACOG): ACOG Practice Bulletin No.142: Cerclage for the management of cervical insufficiency. Obstet Gynecol 123 (2 Pt 1):372–379, 2014. doi: 10.1097/01.AOG.0000443276.68274.cc
2. American College of Obstetricians and Gynecologists (ACOG): ACOG Practice Bulletin, No. 234: Prediction and prevention of spontaneous preterm birth. Obstet Gynecol 138 (2):e65-e90, 2021. doi: 10.1097/AOG.0000000000004479
3. Raju TN, Mercer BM, Burchfield DJ, Joseph GF Jr: Periviable birth: Executive summary of a joint workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Academy of Pediatrics, and American College of Obstetricians and Gynecologists. Obstet Gynecol 123 (5):1083-1096, 2014. doi: 10.1097/AOG.0000000000000243
Key Points
Cervical insufficiency is painless cervical dilation resulting in second-trimester pregnancy loss.
Usually, risk of cervical insufficiency cannot be predicted before a patient has a first preterm delivery.
Do transvaginal ultrasonography after 15 to 16 weeks if women have risk factors or symptoms.
Findings that suggest the diagnosis are cervical shortening to ≤ 2.5 cm, cervical dilation, or protrusion of fetal membranes into the cervical canal.
Treat at-risk women with cervical cerclage.






