



Bacterial vaginosis is a dysbiosis—a complex alteration of vaginal flora in which lactobacilli decrease and anaerobic pathogens overgrow; it is considered a sexually transmitted infection. Symptoms include a vaginal discharge (white-gray or green, thin, homogeneous, smoothly coats vaginal walls, and malodorous [fishy-smelling]) and sometimes mild vulvovaginal irritation. Diagnosis is made with either clinical criteria (Amsel criteria) that include vaginal pH and microscopy or with molecular diagnostic tests. Treatment of the patient is usually with oral or vaginal metronidazole or vaginal clindamycin; for recurrent infections, treatment of sexual partners should be considered.
Bacterial vaginosis is the most common infectious vaginitis. The pathogenesis is unclear but involves the overgrowth of multiple bacterial pathogens and a decrease in the usual -predominant vaginal flora (1).
Anaerobic pathogens that overgrow include Prevotella species, Peptostreptococcus species, Gardnerella vaginalis, Mobiluncus species, and Mycoplasma hominis, which increase in concentration by 10- to 100-fold and replace the lactobacilli that usually maintain a normal vaginal environment (2).
Bacterial vaginosis appears to increase the risk of pelvic inflammatory disease, postabortion and postpartum endometritis, and posthysterectomy vaginal cuff infection. In pregnancy, bacterial vaginosis is associated with an increased risk of chorioamnionitis, prelabor rupture of membranes, preterm labor, and preterm birth.
General references
1. Muzny CA, Sobel JD. Understanding and Preventing Recurring Bacterial Vaginosis: Important Considerations for Clinicians. Int J Womens Health. 2023;15:1317-1325. Published 2023 Aug 9. doi:10.2147/IJWH.S383333
2. Martin DH, Marrazzo JM. The Vaginal Microbiome: Current Understanding and Future Directions. J Infect Dis. 2016;214 Suppl 1(Suppl 1):S36-S41. doi:10.1093/infdis/jiw184
Sexual Transmission of Bacterial Vaginosis
Epidemiologic data strongly suggest BV is a sexually transmitted infection. Studies show associations between incident BV and sexual behaviours, including a new sexual partner (of any gender), having a female partner with BV, receptive oral sex, digital-vaginal and digital-anal sex (1, 2, 3). BV occurs rarely in people who are not sexually active. Evidence supporting male-to-female sexual transmission includes microbiologic evidence of BV–associated bacteria in male partners. Men may harbor bacterial species associated with BV in the distal urethra and subpreputial space, and penile microbiota has been shown to predict a female partner's risk of incident BV (2). For women in a monogamous heterosexual relationship, male partner therapy has been found to reduce rates of recurrent BV.
Risk factors for bacterial vaginosis are the same as those for sexually transmitted infections, including multiple sex partners, sharing of sex toys, and inconsistent or incorrect use of condoms or dental dams. Use of a copper intrauterine device is also a risk factor.
Sexual transmission references
1. Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187. Published 2021 Jul 23. doi:10.15585/mmwr.rr7004a1
2. Vodstrcil LA, Plummer EL, Fairley CK, et al. Male-Partner Treatment to Prevent Recurrence of Bacterial Vaginosis. N Engl J Med. 2025;392(10):947-957. doi:10.1056/NEJMoa2405404
3. Fethers KA, Fairley CK, Hocking JS, et al. Sexual risk factors and bacterial vaginosis: a systematic review and meta-analysis. Clin Infect Dis. 2008;47(11):1426-1435. doi:10.1086/592974
Symptoms and Signs of Bacterial Vaginosis
Vaginal discharge due to bacterial vaginosis is white-gray or green, thin, and homogeneous. It smoothly coats the vaginal walls and is malodorous (fishy-smelling). Odor often becomes stronger when the discharge is more alkaline—after coitus and during menses.
Many patients are asymptomatic. Mild vulvovaginal irritation may occur.
Examination findings may also include mild vulvovaginal erythema or edema.
Diagnosis of Bacterial Vaginosis
Pelvic examination
Vaginal pH and microscopy
Molecular diagnostic tests
A pelvic examination is performed.
A sample of vaginal discharge is collected on a swab and tested with pH paper; pH is measured in 0.2 intervals from 4.0 to 6.0 (normal vaginal pH is 3.8 to 4.2).
Then, a sample of discharge on a swab is placed on 2 slides. Each slide is prepared with a different fluid (added by a dropper to the vaginal discharge sample):
Saline wet mount: 0.9% sodium chloride
Potassium hydroxide (KOH) wet mount: 10% potassium hydroxide
Diagnosis of bacterial vaginosis may be made if 3 of 4 criteria (Amsel criteria) are present (1):
Homogeneous, thin, white-gray discharge that smoothly coats the vaginal walls
Vaginal fluid pH > 4.5
Fishy odor on the whiff test (application of 10% potassium hydroxide to vaginal fluid)
Clue cells (epithelial cells with adherent coccobacilli that partially obscure their cell margins) comprise > 20% of vaginal epithelial cells on saline (0.9%) wet mount

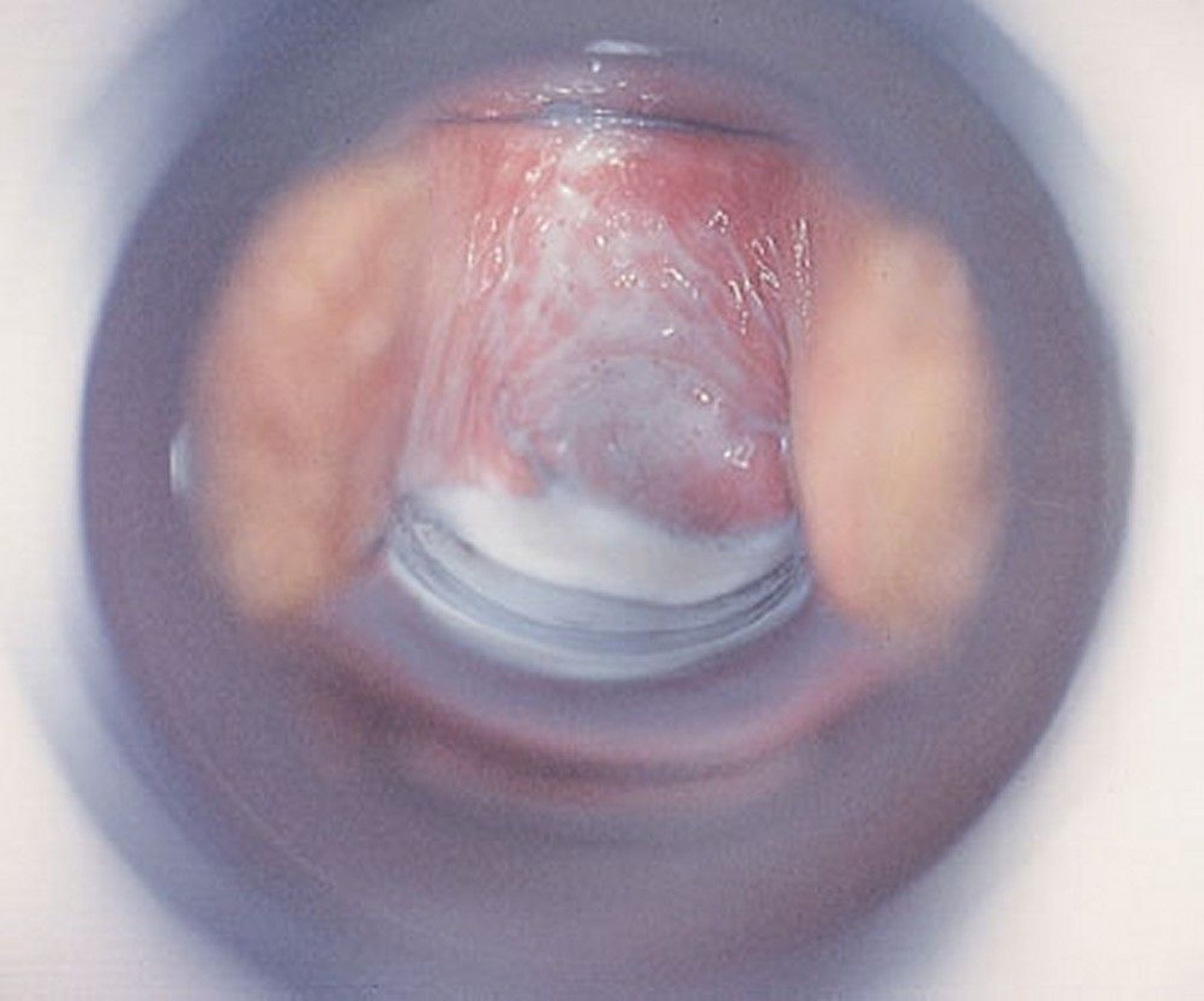
Bacterial vaginosis has a characteristic gray-white discharge.
By permission of the publisher. From Spitzer M, Mann M. In Atlas of Clinical Gynecology: Gynecologic Pathology. Edited by M Stenchever (series editor) and B Goff. Philadelphia, Current Medicine, 1998.


Clue cells are vaginal epithelial cells with adherent coccobacilli that partially obscure their cell margins. Microscopic evaluation of a saline wet mount that shows > 20% of epithelial cells are clue cells contributes to a diagnosis of bacterial vaginosis.
Image obtained from the Public Health Image Library of the Centers for Disease Control and Prevention.
Presence of white blood cells on a saline wet mount suggests a concomitant infection (possibly trichomonal vaginitis or cervicitis or gonorrheal or chlamydial cervicitis) and the need for additional testing.
Molecular diagnostic tests (NAATs and DNA hybridization probes) are available for clinical use (2, 3, 4, 5). If microscopy is unavailable or the diagnosis is inconclusive, a molecular diagnostic test should be considered.
Routine screening for BV in asymptomatic individuals (including in patients planning to become pregnant, during pregnancy, and preoperatively) is not currently recommended (6).
Diagnosis references
1. Vaginitis in Nonpregnant Patients. ACOG Practice Bulletin, Number 215. Obstet Gynecol. 2020;135(1):e1-e17. doi:10.1097/AOG.0000000000003604
2. Cartwright CP, Lembke BD, Ramachandran K, et al. Development and validation of a semiquantitative, multitarget PCR assay for diagnosis of bacterial vaginosis. J Clin Microbiol. 2012;50(7):2321–2329. doi: 10.1128/JCM.00506-12
3. Schwebke JR, Gaydos CA, Nyirjesy P, et al. Diagnostic performance of a molecular test versus clinician assessment of vaginitis. J Clin Microbiol. 2018;56(6):e00252-18. doi: 10.1128/JCM.00252-18
4. Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130 (1):181–189. doi: 10.1097/AOG.0000000000002090
5. Coleman JS, Gaydos CA. Molecular diagnosis of bacterial vaginosis: An update. J Clin Microbiol. 2018;56(9):e00342–e00318. doi: 10.1128/JCM.00342-18
6. Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187. Published 2021 Jul 23. doi:10.15585/mmwr.rr7004a1
Treatment of Bacterial Vaginosis
Metronidazole or clindamycin
The following are the recommended treatment regimens for bacterial vaginosis; they are equally effective (see CDC: Sexually Transmitted Infections Treatment Guidelines, 2021):
Metronidazole 500 mg orally twice a day for 7 days
Metronidazole 0.75% gel 5 g (usually one full applicator, provided with medication) intravaginally once a day for 5 days
Clindamycin 2% cream 5 g (usually one full applicator, provided with medication) intravaginally once a day for 7 days (1)
The choice of oral or topical vaginal treatment is made based on any potential drug interactions with other systemic medications taken by the patient, patient preference, and likelihood of adherence with the full course of treatment. Clindamycin cream is oil-based and may weaken latex condoms and diaphragms for 5 days after use; this specific concern does not apply to metronidazole gel.
All women should be advised to refrain from sexual activity or to use condoms consistently during the BV treatment regimen regardless of which formulation is chosen.
Alternative regimens for BV treatment, which are supported by fewer efficacy data, lack long-term outcomes data, and/or are more expensive include (2):
Clindamycin 300 mg orally twice a day for 7 days
Clindamycin ovules 100 mg intravaginally once a day at bedtime for 3 days (latex contraceptive devices [eg, condoms, diaphragms] should not be used until at least 72 hours after this treatment because of potential damage caused by the oleaginous base of the ovules)
Tinidazole 2 g orally once a day for 2 days
Tinidazole 1 g orally once a day for 5 days
When treated, symptomatic bacterial vaginosis usually resolves in a few days but commonly recurs. If it recurs often (current infection and at least 2 previous episodes within the previous 12 months), ongoing suppressive antibiotics may be required. Suppressive therapy using the metronidazole gel 2 times a week for 16 weeks may be considered in patients with recurrent bacterial vaginosis (5).
Although bacterial vaginosis increases the risk of preterm delivery, screening asymptomatic pregnant women has not been proven effective in reducing that risk in women at average or high risk (6). Pregnant women with symptomatic BV should be treated; treatment regimens may include the recommended regimens of oral metronidazole or vaginal metronidazole 0.75% gel or the alternative regimens of oral clindamycin or vaginal clindamycin ovules (2). Treatments that should not be used during pregnancy include because of insufficient safety data or evidence or harm include: tinidazole (animal data suggest risk of adverse effects), secnidazole, clindamycin 2% vaginal cream, metronidazole 1.3% vaginal gel, and metronidazole 750-mg vaginal tablets.
Vaginal administration of boric acid has been suggested as an option for BV treatment; the proposed mechanism is disruption of BV biofilm (7, 8, 9). Boric acid has been used for over a century to treat vaginal infections, but usually vaginal candidiasis. Use for BV treatment has been investigated only in small observational studies and one phase 2 trial (10, 11). The strongest evidence for its use is from uncontrolled retrospective studies that reported efficacy of boric acid as part of combination therapy for recurrent BV (1, 7, 12). No randomized double-blind controlled trials have definitively established its effectiveness as either monotherapy or as part of combination therapy (10, 11). As an option for women with multiple recurrences, one published regimen is as follows: an oral nitroimidazole (metronidazole or tinidazole 500 mg twice daily for 7 days), followed by boric acid 600 mg intravaginally once a day for 21 days, followed by 0.75% metronidazole gel intravaginally twice weekly for 4 to 6 months (2).
Treatment of sexual partners of women with BV is recommended in certain situations. Historically, male partner treatment trials have shown no or minor benefit for preventing BV recurrence; however, a 2025 randomized trial using oral metronidazole and topical clindamycin applied to the penis demonstrated a significantly lower BV recurrence rate in the female partners compared to no male partner treatment (13). The American College of Obstetricians and Gynecologists recommends that concurrent sexual partner therapy with a combination of oral and topical antimicrobial agents should be considered for male sexual partners of adult patients with recurrent, symptomatic bacterial vaginosis, and shared decision making regarding concurrent sexual partner therapy for those with same-sex partners and for patients with a first occurrence of symptomatic bacterial vaginosis (14).
Treatment references
1. Surapaneni S, Akins R, Sobel JD. Recurrent Bacterial Vaginosis: An Unmet Therapeutic Challenge. Experience With a Combination Pharmacotherapy Long-Term Suppressive Regimen. Sex Transm Dis. 2021;48(10):761-765. doi:10.1097/OLQ.0000000000001420
2. Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187. Published 2021 Jul 23. doi:10.15585/mmwr.rr7004a1
3. Schwebke JR, Morgan FG Jr, Koltun W, Nyirjesy P. A phase-3, double-blind, placebo-controlled study of the effectiveness and safety of single oral doses of secnidazole 2 g for the treatment of women with bacterial vaginosis. Am J Obstet Gynecol. 2017;217 (6):678.e1–678.e9, 2017. doi: 10.1016/j.ajog.2017.08.017
4. Hillier SL, Nyirjesy P, Waldbaum AS, et al. Secnidazole treatment of bacterial vaginosis: A randomized controlled trial. Obstet Gynecol. 2017;130(2):379-386. doi: 10.1097/AOG.0000000000002135
5. Sobel JD, Ferris D, Schwebke J, et al: Suppressive antibacterial therapy with 0.75% metronidazole vaginal gel to prevent recurrent bacterial vaginosis. Am J Obstet Gynecol 194(5):1283-1289, 2006. doi:10.1016/j.ajog.2005.11.041
6. US Preventive Services Task Force, Owens DK, Davidson KW, et al. Screening for Bacterial Vaginosis in Pregnant Persons to Prevent Preterm Delivery: US Preventive Services Task Force Recommendation Statement. JAMA. 2020;323(13):1286-1292. doi:10.1001/jama.2020.2684
7. Reichman O, Akins R, Sobel JD. Boric acid addition to suppressive antimicrobial therapy for recurrent bacterial vaginosis. Sex Transm Dis. 2009;36(11):732-734. doi:10.1097/OLQ.0b013e3181b08456
8. Tomás M, Palmeira-de-Oliveira A, Simões S, et al. Bacterial vaginosis: Standard treatments and alternative strategies. Int J Pharm. 2020;587:119659. doi:10.1016/j.ijpharm.2020.119659
9. Sousa LGV, Pereira SA, Cerca N. Fighting polymicrobial biofilms in bacterial vaginosis. Microb Biotechnol. 2023;16(7):1423-1437. doi:10.1111/1751-7915.14261
10. Zeron Mullins M, Trouton KM. BASIC study: is intravaginal boric acid non-inferior to metronidazole in symptomatic bacterial vaginosis? Study protocol for a randomized controlled trial. Trials. 2015;16:315. Published 2015 Jul 26. doi:10.1186/s13063-015-0852-5
11. Mittelstaedt R, Kretz A, Levine M, et al. Data on Safety of Intravaginal Boric Acid Use in Pregnant and Nonpregnant Women: A Narrative Review. Sex Transm Dis. 2021;48(12):e241-e247. doi:10.1097/OLQ.0000000000001562
12. Powell A, Ghanem KG, Rogers L, et al. Clinicians' Use of Intravaginal Boric Acid Maintenance Therapy for Recurrent Vulvovaginal Candidiasis and Bacterial Vaginosis. Sex Transm Dis. 2019;46(12):810-812. doi:10.1097/OLQ.0000000000001063
13. Vodstrcil LA, Plummer EL, Fairley CK, et al. Male-Partner Treatment to Prevent Recurrence of Bacterial Vaginosis. N Engl J Med. 2025;392(10):947-957. doi:10.1056/NEJMoa2405404
14. Concurrent Sexual Partner Therapy to Prevent Bacterial Vaginosis Recurrence. Obstet Gynecol. 2025;146(6):e111-e114. doi:10.1097/AOG.0000000000006102
Key Points
Bacterial vaginosis is a dysbiosis of the vaginal flora in which lactobacilli decrease and anaerobic pathogens overgrow; it is considered a sexually transmitted infection.
Vaginal discharge smoothly coats the vaginal walls and is malodorous, white-gray or green, thin, and homogeneous; many patients are asymptomatic.
Diagnosis is with pelvic examination, vaginal pH testing, microscopy, and molecular diagnostic tests.
Treat with metronidazole or clindamycin
Drug Information for the Topic





