



Actinomycosis is a chronic localized or hematogenous anaerobic infection caused by Actinomyces israelii and other species of Actinomyces. Findings are a local abscess with multiple draining sinuses, a tuberculosis-like pneumonitis, and low-grade systemic symptoms. Diagnosis is by the typical presentation plus laboratory identification. Treatment is with a long course of antibiotics and surgery.
(See also Overview of Anaerobic Bacteria.)
The causative organisms, Actinomyces species (most commonly A. israelii), are often present commensally on the gums, tonsils, and teeth and may be present in the intestines and vagina. Many, if not most, infections are polymicrobial, with other bacteria (oral anaerobes, staphylococci, streptococci, Aggregatibacter actinomycetemcomitans, Enterobacterales [previously Enterobacteriaceae]) frequently cultured from lesions.
Actinomycosis takes several forms:
Cervicofacial (lumpy jaw): The most common portal of entry is periodontal disease.
Thoracic: Pulmonary disease results from aspiration of oral secretions.
Abdominal: Disease presumably results from a break in the mucosa of a diverticulum or the appendix or from trauma.
Uterine: This localized pelvic form is a complication of certain types of intrauterine device (IUD).
Generalized: Rarely, the infection spreads from primary sites, presumably by hematogenous seeding.
Actinomycosis most often occurs in adult males.
Symptoms and Signs of Actinomycosis
The characteristic lesion of actinomycosis is an indurated area of multiple, small, communicating abscesses surrounded by granulation tissue. Lesions tend to form sinus tracts that communicate to the skin and drain a purulent discharge containing “sulfur” granules (rounded or spherical, usually yellowish, and ≤ 1 mm in diameter). Sulfur granules are named because of their yellow appearance but do not contain sulfur; they consist of a tangled mass of the branching filaments of Actinomyces. Infection spreads to contiguous tissues but only rarely hematogenously.

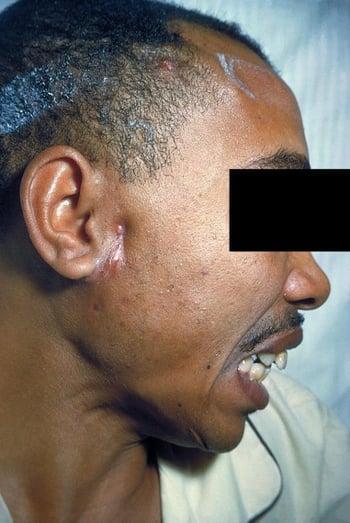
Drainage from a preauricular lesion originating from a sinus tract is shown.
The cervicofacial form usually begins as a small, flat, hard swelling, with or without pain, under the oral mucosa or the skin of the neck or as a subperiosteal swelling of the jaw. Subsequently, areas of softening appear and develop into sinuses and fistulas that discharge the characteristic sulfur granules. The cheek, tongue, pharynx, salivary glands, cranial bones, meninges, or brain may be affected, usually by direct extension.
In the abdominal form, the intestines (usually the cecum and appendix) and the peritoneum are infected. Pain, fever, vomiting, diarrhea or constipation, and emaciation are characteristic. One or more abdominal masses develop and cause signs of partial intestinal obstruction. Draining sinuses and intestinal fistulas may develop and extend to the external abdominal wall.
In the localized pelvic form, patients present with vaginal discharge and pelvic or lower abdominal pain. This form usually occurs in patients who use an IUD.
In the thoracic form, lung involvement resembles tuberculosis (TB). Extensive invasion may occur before chest pain, fever, and productive cough appear. Perforation of the chest wall, with chronic draining sinuses, may result and the ribs and spine may be involved as well. Invasion into the pleural space may lead to pleuritis and empyema.
In the generalized form, infection spreads hematogenously to multiple areas, including the skin, vertebral bodies, brain, liver, kidneys, ureters, and, in women, pelvic organs. Diverse symptoms (eg, back pain, headache, abdominal pain) related to these sites may occur.
Diagnosis of Actinomycosis
Microscopy
Culture
Actinomycosis is suspected clinically and confirmed by identification of A. israelii or other Actinomyces species using microscopy and culture of sputum (ideally obtained endoscopically), pus, or a biopsy specimen. Imaging tests (eg, chest radiograph, abdominal or thoracic CT scan) are often done, depending on presentation.
In pus or tissue, the microorganism appears as the distinctive sulfur granules or as tangled masses of branched and unbranched wavy bacterial filaments, pus cells, and debris, surrounded by an outer zone of radiating, club-shaped, hyaline, and refractive filaments that take hematoxylin-eosin stain in tissue but are positive on Gram stain. The laboratory must be notified that actinomycosis is suspected because special procedures are required to isolate and identify these organisms.
Lesions in any location may simulate malignant growths. Lung lesions must be distinguished from those of TB and cancer. Most abdominal lesions occur in the ileocecal region and are difficult to diagnose, except during laparotomy or when draining sinuses appear in the abdominal wall.
Treatment of Actinomycosis
High-dose penicillin
Sometimes aspiration of small abscesses and drainage of large ones
Surgical excision of fistulas
Most patients with actinomycosis respond to antibiotics, but response is usually slow because of extensive tissue induration and the relatively avascular nature of the lesions. Therefore, treatment must be continued for at least 8 weeks and occasionally for ≥ 1 year, until symptoms and signs have resolved.
High doses of IV penicillin G are usually effective for initial treatment. Oral penicillin or amoxicillin may be substituted after about 2 to 6 weeks. Alternative antibiotics (tetracycline, doxycycline, minocycline, clindamycin, erythromycin, ceftriaxone, linezolid) have also been successful. Antibiotic regimens may be broadened to cover other pathogens cultured from lesions.
Treatment of IUD-associated pelvic actinomycosis also involves removal of the IUD.
Surgical procedures may be required. Extensive pelvic disease may require drainage of intra-abdominal abscesses, sometimes with hysterectomy and salpingo-oophorectomy. Sometimes small abscesses can be aspirated, and large ones are drained. Fistulas are excised surgically.
Recompression therapy (also known as hyperbaric oxygen therapy) may be beneficial.
Prognosis for Actinomycosis
Actinomycosis is slowly progressive. Prognosis relates directly to early diagnosis and site of infection. It is most favorable in the cervicofacial form and progressively worse in the thoracic, abdominal, and generalized forms, especially if the central nervous system is involved.
Key Points
Actinomycosis usually involves multiple, small, communicating abscesses with sinus tracts that drain a purulent discharge.
Infection typically involves the neck and face, lungs, or abdominal and pelvic organs.
Microscopically, Actinomyces appears as distinctive "sulfur" granules (rounded or spherical particles, usually yellowish, and ≤ 1 mm in diameter) or as tangled masses of branched and unbranched wavy bacterial filaments.
High-dose penicillin is usually effective, but antibiotics must be given long-term (8 weeks to 1 year).
Surgery to drain abscesses and excise fistulas may be needed.
Drug Information for the Topic





