

Meningococci (Neisseria meningitidis) are gram-negative diplococci that cause meningitis and meningococcemia. Symptoms, usually severe, include headache, nausea, vomiting, photophobia, lethargy, rash, multiple organ failure, shock, and disseminated intravascular coagulation. Diagnosis is clinical, confirmed by culture. Treatment is with penicillin or a third-generation cephalosporin.
Meningococci are gram-negative aerobic diplococci that belong to the family Neisseriaceae. There are 13 serogroups; 6 serogroups (A, B, C, W135, X, and Y) cause most human disease.
Worldwide, the incidence of endemic meningococcal disease is 0.5 to 5/100,000, with an increased number of cases during winter and spring in temperate climates (1). Local outbreaks occur most frequently in sub-Saharan Africa between Gambia and Senegal in the west and Ethiopia, Eritrea, and northern Kenya in the east; this area is known as the sub-Saharan (African) meningitis belt, which includes 26 countries. In major African epidemics (which were often caused by serogroup A), attack rates ranged from 100 to 800/100,000 and affected up to 200,000 people each year. After widespread use of the meningococcal A vaccine in the African meningitis belt, serogroup A has been replaced by other meningococcal serogroups and by Streptococcus pneumoniae.
In the United States, the annual incidence ranges from 0.12 to 1.1/100,000. Over the past 20 years, incidence of meningococcal disease declined annually, but, since 2021, it has increased sharply and now exceeds pre-pandemic levels (2). Most cases are sporadic, with the highest rates in children < 1 year of age. Outbreaks of meningococcal disease are rare in the United States, and only about 1 in 20 cases (5%) is related to an outbreak (3). Outbreaks tend to occur in semiclosed communities (eg, military recruit camps, correctional facilities, college/university dormitories, schools, day care centers) and most often involve patients 16 to 23 years of age. Serogroups B and C cause 25 to 40% of invasive disease (3). Serogroup Y has accounted for a large percentage of the recent increase in reported cases (4). Serogroup A is rare in the United States.
References
1. Parikh SR, Campbell H, Bettinger JA, et al. The everchanging epidemiology of meningococcal disease worldwide and the potential for prevention through vaccination. J Infect. 2020;81(4):483-498. doi:10.1016/j.jinf.2020.05.079
2. Centers for Disease Control and Prevention: Meningococcal Disease Surveillance and Trends. Accessed May 29, 2024.
3. Centers for Disease Control and Prevention: The Pink Book: Meningococcal Disease. Accessed May 29, 2024.
4. Centers for Disease Control and Prevention: Increase in Invasive Serogroup Y Meningococcal Disease in the United States. Accessed May 29, 2024.
Diseases Caused by Meningococci
Over 90% of invasive meningococcal infections involve (1)
Meningitis (around 50% of cases)
Meningococcemia (septicemia) (around 35 to 40% of cases)
(See also Bacterial Meningitis in Infants Over 3 Months of Age.)
Infections of lungs, joints, respiratory passageways, genitourinary organs, rectum, eyes, endocardium, and pericardium may occur but are less common.
N. meningitidis has been reported to cause urethritis and cervicitis. Recently, the incidence of meningococcal urethritis has been increasing in men who have sex with men and typically occurs after orogenital contact with an oropharyngeal meningococcal carrier. N. meningitidis colonizes the nasopharynx. N. meningitidis may also cause proctitis, primarily in men who have sex with men.
Reference
1. Centers for Disease Control and Prevention: The Pink Book: Meningococcal Disease. Accessed May 29, 2024.
Pathophysiology of Meningococcal Diseases
N. meningitidis generally exists as a commensal component of the normal nasopharyngeal microbiota (carrier state) and has the potential to cause severe and often devastating invasive disease. However, despite documented high rates of colonization (5 to 40% of healthy people), which may be transient, brief, or prolonged, transition to invasive disease is rare (< 1%) (1). A combination of genetically determined virulence features specific to the colonized meningococcal strain along with predisposing host susceptibility factors have the greatest influence on the development of invasive disease, which occurs primarily in previously uninfected patients.
Carriers (and infected patients) may transmit the organism to people who have direct contact with respiratory secretions or who inhale large-droplet nuclei from a carrier or patient. Nasopharyngeal carriage rates are highest in adolescents and young adults, who serve as reservoirs for transmission of N. meningitidis. Carrier rates rise dramatically during epidemics.
After invading the body, N. meningitidis causes meningitis and severe bacteremia in children and adults, resulting in profound vascular effects. Infection can rapidly become fulminant. The overall case-fatality rate is 10 to 15%; for meningitis alone, it is 5 to 18% but may be up to 40% for meningococcemia with septic shock (2, 3).
Risk factors
The most frequently infected are
Children aged 6 months to 3 years
Other high-risk groups include
Adolescents and young adults (16 to 20 years of age)
Military recruits
First-year college students living in dormitories
Travelers to places where meningococcal disease is common (eg, certain countries in Africa and in Saudi Arabia during the Hajj)
People with functional or anatomic asplenia or complement deficiencies (C3, C5–C9, properdin, factor H, or factor D)
People treated with eculizumab or ravulizumab (terminal complement activation blocking agents)
People with HIV infection
Men who have sex with men
Microbiologists working with N. meningitidis isolates
Close contacts of patients with invasive meningococcal disease
Infection or vaccination confers serogroup-specific immunity.
Antecedent viral infection, household crowding, chronic underlying illness, and both active and passive smoking are associated with increased risk of meningococcal disease.
Pathophysiology references
1. Caugant DA, Maiden MC. Meningococcal carriage and disease--population biology and evolution. Vaccine. 2009;27 Suppl 2(4):B64-B70. doi:10.1016/j.vaccine.2009.04.061
2. Mbaeyi SA, Bozio CH, Duffy J, et al. Meningococcal Vaccination: Recommendations of the Advisory Committee on Immunization Practices, United States, 2020. MMWR Recomm Rep. 2020;69(9):1-41. Published 2020 Sep 25. doi:10.15585/mmwr.rr6909a1
3. MacNeil JR, Blain AE, Wang X, Cohn AC. Current Epidemiology and Trends in Meningococcal Disease-United States, 1996-2015. Clin Infect Dis. 2018;66(8):1276-1281. doi:10.1093/cid/cix993
Symptoms and Signs of Meningococcal Diseases
Patients with meningococcal meningitis frequently report fever, headache, and stiff neck, which are indistinguishable from symptoms reported in acute bacterial meningitis due to other pathogens. Other symptoms include nausea, vomiting, photophobia, and lethargy. Meningeal signs are often apparent during physical examination.
Meningococcemia often manifests with an acute systemic illness, including fever, chills, myalgias, and arthralgias. A maculopapular or hemorrhagic petechial rash often appears soon after disease onset.
Fulminant meningococcemia syndromes include Waterhouse-Friderichsen syndrome (septicemia, profound shock, cutaneous purpura, adrenal hemorrhage), sepsis with multiple organ failure, shock, and disseminated intravascular coagulation. A rare, chronic meningococcemia causes recurrent mild symptoms (mostly joint and cutaneous).
Complications of meningococcemia and meningococcal meningitis are common and serious. Of patients who recover, 10 to 20% have serious sequelae, such as permanent hearing loss, intellectual disability, or loss of phalanges or limbs.


Fulminant meningococcemia initially causes petechiae, which become confluent and rapidly progress to ecchymoses.
Fulminant meningococcemia initially causes petechiae, which become confluent and rapidly progress to ecchymoses.
Photo courtesy of Mr. Gust via the Public Health Image Library of the Centers for Disease Control and Prevention.


Petechiae and purpura are visible on the child's face. Hemorrhagic return from the nasogastric tube is consistent with disseminated intravascular coagulation, also secondary to meningococcemia.
Petechiae and purpura are visible on the child's face. Hemorrhagic return from the nasogastric tube is consistent with
© Springer Science+Business Media

© Springer Science+Business Media


Photo courtesy of Karen McKoy, MD.


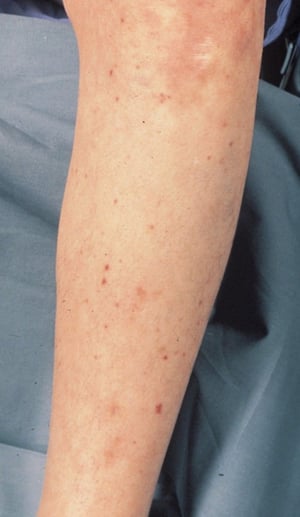
Petechiae and purpura secondary to meningococcemia are widespread. Lesions tend to be common on the trunk and lower extremities.
Petechiae and purpura secondary to meningococcemia are widespread. Lesions tend to be common on the trunk and lower ext
© Springer Science+Business Media

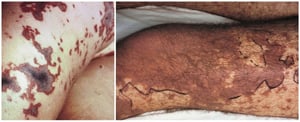
Petechiae are isolated in some areas and coalescent and developing necrosis in other areas (left). A large area of necrosis is seen (right).
Petechiae are isolated in some areas and coalescent and developing necrosis in other areas (left). A large area of necr
© Springer Science+Business Media
Fulminant meningococcemia initially causes petechiae, which become confluent and rapidly progress to ecchymoses.
Fulminant meningococcemia initially causes petechiae, which become confluent and rapidly progress to ecchymoses.
Photo courtesy of Mr. Gust via the Public Health Image Library of the Centers for Disease Control and Prevention.
Petechiae and purpura are visible on the child's face. Hemorrhagic return from the nasogastric tube is consistent with disseminated intravascular coagulation, also secondary to meningococcemia.
Petechiae and purpura are visible on the child's face. Hemorrhagic return from the nasogastric tube is consistent with
© Springer Science+Business Media
© Springer Science+Business Media
Photo courtesy of Karen McKoy, MD.
Petechiae and purpura secondary to meningococcemia are widespread. Lesions tend to be common on the trunk and lower extremities.
Petechiae and purpura secondary to meningococcemia are widespread. Lesions tend to be common on the trunk and lower ext
© Springer Science+Business Media
Petechiae are isolated in some areas and coalescent and developing necrosis in other areas (left). A large area of necrosis is seen (right).
Petechiae are isolated in some areas and coalescent and developing necrosis in other areas (left). A large area of necr
© Springer Science+Business Media
Diagnosis of Meningococcal Diseases
Gram stain and culture of cerebral spinal fluid (CSF)
Sometimes nucleic acid–based testing (NAAT) such as polymerase chain reaction (PCR)
Neisseria are small, gram-negative diplococci readily identified with Gram stain and by other standard bacteriologic identification methods. Bacteriologic isolation from a sterile body fluid such as blood, CSF, or synovial fluid confirms the diagnosis.
PCR testing of CSF, blood, and other normally sterile sites for N. meningitidis is more sensitive and specific than culture and may be useful when the CSF Gram stain is negative and when prior antibiotic administration interferes with isolating the organism.
Serologic methods, such as latex agglutination and coagglutination tests, allow rapid presumptive diagnosis of N. meningitidis in blood, CSF, synovial fluid, and urine.
Because meningococci and gonococci appear similar on Gram stain, meningococcal urethritis should be considered if the urethral discharge shows gram-negative diplococci, but the NAAT is negative for gonococci; this situation requires culture of the urethral discharge to identify the Neisseria species causing the infection (see Diseases Characterized by Urethritis and Cervicitis from the CDC).
Treatment of Meningococcal Diseases
Ceftriaxone
Dexamethasone
While awaiting definitive identification of the causal organism, immunocompetent adults suspected of having meningococcal infection are given a third-generation cephalosporin (eg, cefotaxime 2 g IV every 4 to 6 hours, ceftriaxone 2 g IV every 12 hours) or meropenem (2 g IV every 8 hours) plus vancomycin 15 to 20 mg/kg IV every 8 to 12 hours. In immunocompromised patients and in patients While awaiting definitive identification of the causal organism, immunocompetent adults suspected of having meningococcal infection are given a third-generation cephalosporin (eg, cefotaxime 2 g IV every 4 to 6 hours, ceftriaxone 2 g IV every 12 hours) or meropenem (2 g IV every 8 hours) plus vancomycin 15 to 20 mg/kg IV every 8 to 12 hours. In immunocompromised patients and in patients> 50 years, coverage for Listeria monocytogenes should be considered by adding ampicillin 2 g IV every 4 hours. The fluoroquinolone antibiotic, moxifloxacin, is an alternative in patients allergic to penicillin and cephalosporins.should be considered by adding ampicillin 2 g IV every 4 hours. The fluoroquinolone antibiotic, moxifloxacin, is an alternative in patients allergic to penicillin and cephalosporins.
Once N. meningitidis has been definitively identified, the preferred treatment is one of the following:
Ceftriaxone 2 g IV every 12 hoursCeftriaxone 2 g IV every 12 hours
Penicillin 4 million units IV every 4 hours
In many countries, penicillin G is still the first choice for invasive meningococcal disease. However, because many countries, including the United States, have increasing incidence of isolates with reduced susceptibility to In many countries, penicillin G is still the first choice for invasive meningococcal disease. However, because many countries, including the United States, have increasing incidence of isolates with reduced susceptibility topenicillin, those countries typically give initial treatment with a third-generation cephalosporin, such as ceftriaxone or cefotaxime. Also, when penicillin is used, follow-up treatment with ceftriaxone, ciprofloxacin, or rifampin is necessary to eliminate nasopharyngeal carriage. There have been reports of isolates resistant to both penicillin and third-generation cephalosporins (, ciprofloxacin, or rifampin is necessary to eliminate nasopharyngeal carriage. There have been reports of isolates resistant to both penicillin and third-generation cephalosporins (1, 2).
Corticosteroids decrease the incidence of neurologic complications in children and adults with suspected bacterial meningitis due to Haemophilus influenzae type b or S. pneumoniae. The evidence is less clear when N. meningitidis is the cause. High-dose corticosteroids worsen the outcome in meningococcal shock without meningitis and should not be used in such cases; however, low-dose corticosteroids can be used in patients with inadequate adrenal function. When corticosteroids are used, they should be given with or before the first dose of antibiotics. Dexamethasone 0.15 mg/kg IV every 6 hours in children and 10 mg IV every 6 hours in adults is given for 4 days.is the cause. High-dose corticosteroids worsen the outcome in meningococcal shock without meningitis and should not be used in such cases; however, low-dose corticosteroids can be used in patients with inadequate adrenal function. When corticosteroids are used, they should be given with or before the first dose of antibiotics. Dexamethasone 0.15 mg/kg IV every 6 hours in children and 10 mg IV every 6 hours in adults is given for 4 days.
Meningococcal urethritis is treated with the same medications as gonococcal urethritis. The risk of sexual transmission of meningococcal urethritis is unclear; however, treatment of sex partners can be considered (see Diseases Characterized by Urethritis and Cervicitis from the CDC).
Treatment references
1. Spiliopoulou I, Xirogianni A, Simantirakis S, Tzanakaki G. Meningococcal Antibiotic Resistance: Molecular Characterization of Isolates from Patients with Invasive Meningococcal Disease (IMD) in Greece. Antibiotics (Basel). 2023;12(7):1136. Published 2023 Jun 30. doi:10.3390/antibiotics12071136
2. Willerton L, Lucidarme J, Walker A, et al. Antibiotic resistance among invasive Neisseria meningitidis isolates in England, Wales and Northern Ireland (2010/11 to 2018/19). PLoS One. 2021;16(11):e0260677. Published 2021 Nov 29. doi:10.1371/journal.pone.0260677
Prevention of Meningococcal Diseases
Antibiotic prophylaxis
Close contacts of people with meningococcal disease are at increased risk of acquiring disease and should receive a prophylactic antibiotic.
Options include rifampin, ceftriaxone, and a fluoroquinolone (ciprofloxacin or levofloxacin).Options include rifampin, ceftriaxone, and a fluoroquinolone (ciprofloxacin or levofloxacin).
Azithromycin is not routinely recommended but could be an alternative for patients with contraindications to recommended medications.Azithromycin is not routinely recommended but could be an alternative for patients with contraindications to recommended medications.
Ciprofloxacin-resistant meningococcal disease is rare but has been reported in several countries (Greece, England, Wales, Australia, Spain, Argentina, France, and India) and in 2 U.S. states (North Dakota and Minnesota). When choosing an antibiotic for postexposure prophylaxis, clinicians should consider reports of local ciprofloxacin-resistant meningococci (1).
Vaccination
See Meningococcal Vaccine for more information, including indications, contraindications and precautions, dosing and administration, and adverse effects. See also the vaccine schedules for children and adolescents and adults from the Centers for Disease Control and Prevention (CDC) and meningococcal vaccine recommendations from the Advisory Committee on Immunization Practices (ACIP).
All children should receive a quadrivalent conjugate (MenACWY-D, MenACWY-CRM, or MenACWY-TT) vaccine at age 11 or 12 years, with a booster dose at age 16 years (see also the routine childhood vaccination schedule). These vaccines are also recommended for adults who are at increased risk.
MenB-4C or MenB-FHbp (recombinant protein monovalent vaccines that protect against serogroup B) is recommended for people ≥ 10 years who are at increased risk of serogroup B meningococcal disease.
Combination MenABCWY vaccination is an option for people ≥ 10 years who are receiving MenACWY and MenB vaccines at the same visit (2).
Prevention references
1. Berry I, Rubis AB, Howie RL, et al. Selection of Antibiotics as Prophylaxis for Close Contacts of Patients with Meningococcal Disease in Areas with Ciprofloxacin Resistance - United States, 2024. MMWR Morb Mortal Wkly Rep. 2024;73(5):99-103. Published 2024 Feb 8. doi:10.15585/mmwr.mm7305a2
2. Collins JP, Crowe SJ, Ortega-Sanchez IR, et al. Use of the Pfizer Pentavalent Meningococcal Vaccine Among Persons Aged ≥10 Years: Recommendations of the Advisory Committee on Immunization Practices - United States, 2023. MMWR Morb Mortal Wkly Rep. 2024;73:345–350. Published 2024 Apr 18. doi:10.15585/mmwr.mm7315a4
Key Points
Over 90% of invasive meningococcal infections involve meningitis or meningococcemia.
An asymptomatic nasopharyngeal carrier state is common; transmission usually occurs via direct contact with respiratory secretions from a carrier.
In the United States, most cases are sporadic, typically in children < 2 years of age, but outbreaks can occur, primarily in semiclosed communities (eg, military recruit camps, dormitories, day care centers) and often involve patients aged 16 to 23 years.
Treat with ceftriaxone or penicillin; add dexamethasone for patients with meningitis.Treat with ceftriaxone or penicillin; add dexamethasone for patients with meningitis.
Give close contacts a prophylactic antibiotic.
Vaccinate all children starting at age 11 or 12 years, and selectively vaccinate high-risk younger children and other high-risk people.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Centers for Disease Control and Prevention (CDC): Child and Adolescent Immunization Schedule by Age
CDC: STI Treatment Guidelines 2021: Diseases Characterized by Urethritis and Cervicitis
Advisory Committee on Immunization Practices (ACIP): Meningococcal ACIP Vaccine Recommendations
Drugs Mentioned In This Article





