



Open growth plates in children are often involved in fractures. Diagnosis is by radiograph. Treatment is with closed reduction and immobilization or open reduction with internal fixation (ORIF).
(See also Overview of Fractures.)
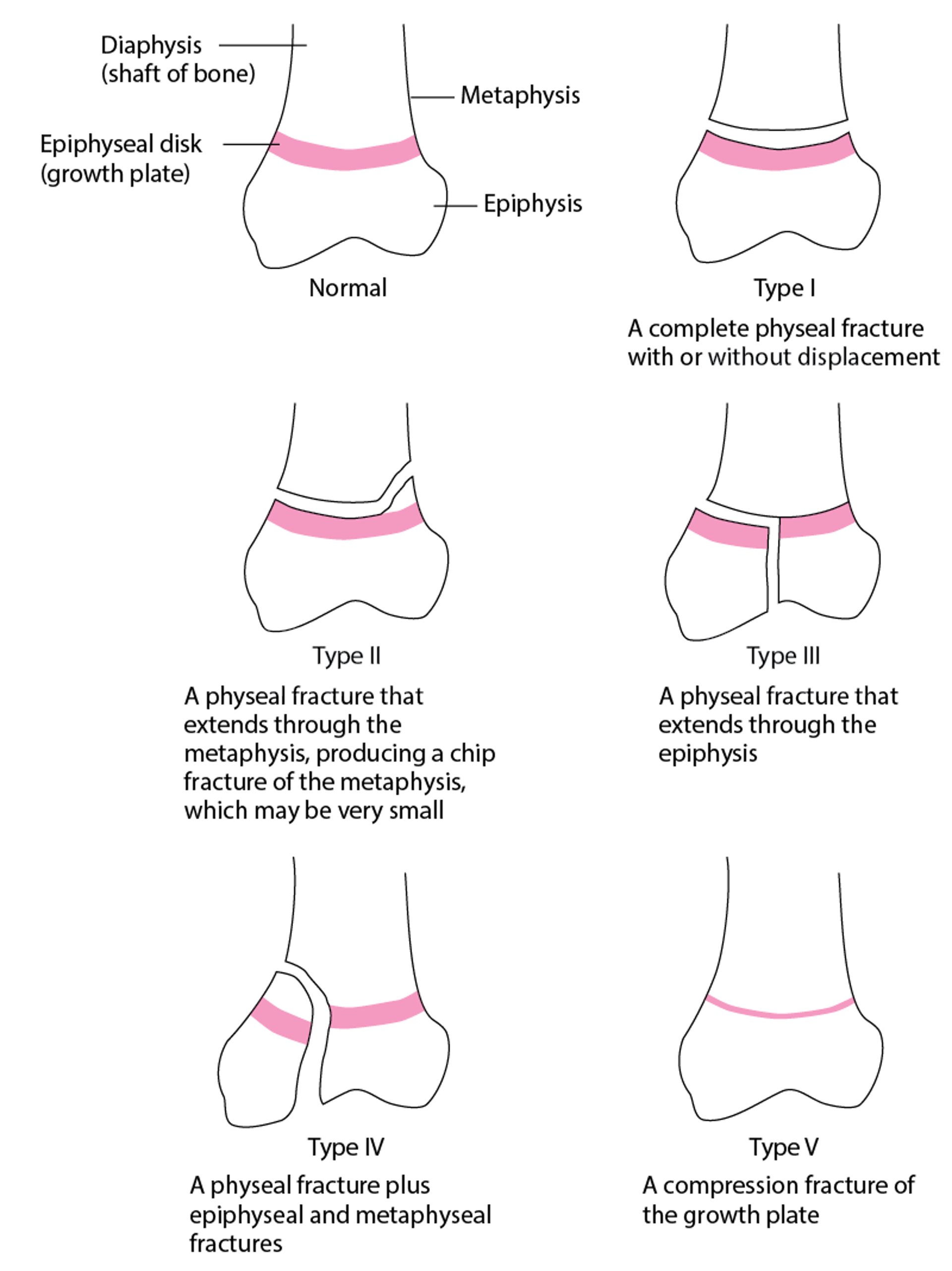
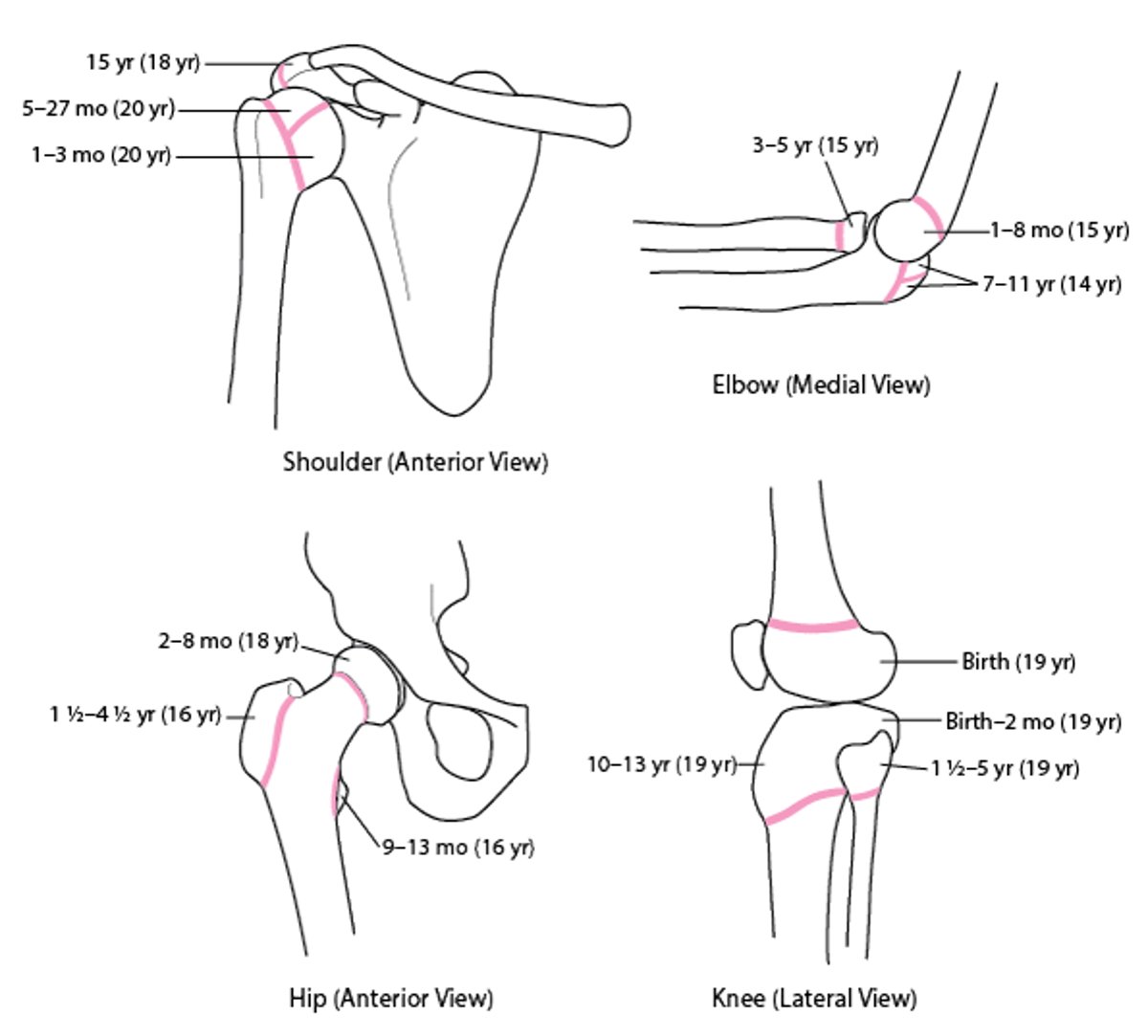
Bone grows as tissue is added at the physeal disk (growth plate), which is bordered by the metaphysis proximally and the epiphysis distally (see figure ). The age at which the growth plate closes and bone growth stops varies by bone, but the growth plate is closed in all bones by age 20 (see figure ).
Before closure, the growth plate is the most fragile part of the bone and is therefore frequently disrupted when force is applied. Growth plate fractures may extend into the metaphysis and/or epiphysis; the different types are classified by the . Risk of impaired growth increases as fractures progress from type I through type V. In English, a useful mnemonic for the types is SALTR:
Type I: S = Straight (the fracture line goes straight across the growth plate)
Type II: A = Above (the fracture line extends above or away from the growth plate)
Type III: L = Lower (the fracture line extends below the growth plate)
Type IV: T = Through (the fracture line extends through the metaphysis, growth plate, and epiphysis)
Type V: R = Rammed (the growth plate has been crushed)
Children with injuries that involve the epiphysis as well as the growth plate (Salter-Harris types III and IV) or that compress the growth plate (Salter-Harris type V) tend to have a worse prognosis.
Salter-Harris Classification of Physeal Disk (Growth Plate) Fractures
Types I through IV are physeal separations; the growth plate is separated from the metaphysis. Type II is the most common, and type V is the least common. |

Epiphyseal Disks (Growth Plates)
The first numbers are the age at which ossification first appears on radiograph; the numbers in parentheses are the age at which union occurs. |

Diagnosis of Pediatric Physeal Fractures
Radiographs
Growth plate fractures are suspected in children who have tenderness and swelling localized over the growth plate or who cannot move or put weight on the affected limb.
Radiographs are the diagnostic test of choice. If findings are equivocal, contralateral comparison radiographs may be helpful. Despite use of comparison views, radiographs may appear normal in Salter-Harris types I and V. If radiograph appear normal but a growth plate fracture is suspected, patients are assumed to have a fracture. A splint or cast is applied, and patients are reexamined in several days. Continued pain and tenderness suggest a growth plate fracture.
Treatment of Pediatric Physeal Fractures
Closed reduction (if needed) and immobilization or open reduction with internal fixation (ORIF), depending on the fracture
Depending on the particular fracture, closed reduction is usually sufficient for Salter-Harris types I and II; ORIF is often required for types III and IV.
Patients with type V injuries should be referred to a pediatric orthopedist because such injuries almost always lead to growth abnormalities.
Key Points
Because the growth plate is more fragile in children, it is often disrupted before other stabilizing structures (eg, major ligaments).
The prognosis tends to be worse for children with Salter-Harris types III, IV, and V than for those with types I and II.
Consider comparison radiographs of the uninjured side if fracture is suspected but is not visible on radiographs of the injured side.
ORIF is often required for Salter-Harris types III and IV.





