



In total anomalous pulmonary venous return, the pulmonary veins drain to a confluence adjacent to the posterior wall of the left atrium but do not connect to the left atrium. Instead, the entire pulmonary venous return enters the systemic venous circulation through one or more persistent embryologic connections. Filling of the left heart structures and systemic blood flow is dependent on having an adequate atrial communication (stretched patent foramen ovale or actual atrial septal defect). If there is no obstruction to pulmonary venous return, cyanosis is mild, but pulmonary blood flow is markedly increased. Patients may be only mildly symptomatic or have significant heart failure symptoms. Severe obstruction of the pulmonary venous return may occur, resulting in severe neonatal cyanosis, pulmonary edema, and pulmonary hypertension. Diagnosis is by echocardiography. Surgical repair is required.
(See also Overview of Congenital Cardiovascular Anomalies.)
Total anomalous pulmonary venous return (TAPVR—see figure ) accounts for 1 to 2% of congenital heart anomalies. The clinical manifestation depends on the connection between the pulmonary venous confluence and the right side of the circulation. The most common types include
Return via an ascending left vertical vein that drains to the innominate vein or to the superior vena cava (supracardiac TAPVR)
A descending vein that drains infradiaphragmatically to the portal circulation (infracardiac TAPVR)
Connection of the pulmonary vein confluence to the coronary sinus (cardiac TAPVR)
The infradiaphragmatic drainage type is invariably severely obstructed, leading to dramatic pulmonary edema and cyanosis unresponsive to supplemental oxygen that manifest shortly after birth. The other 2 types do not typically involve obstruction and lead to mild to moderate signs of heart failure and mild cyanosis in the first month of life.
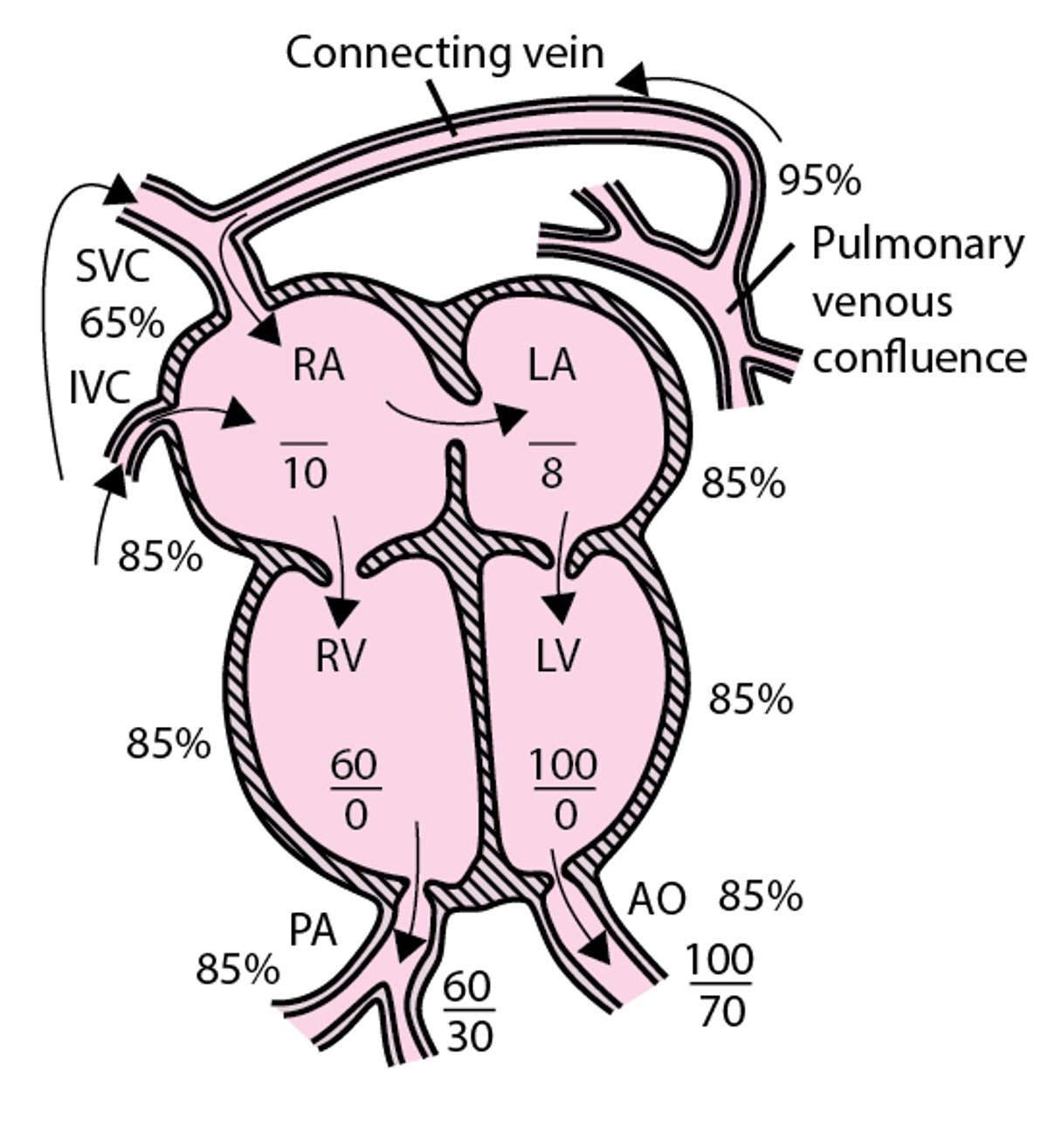
Total anomalous pulmonary venous return
The pulmonary veins do not connect to the left atrium; instead, the entire pulmonary venous return enters systemic venous circulation through various connections. Systemic blood flow depends on right-to-left atrial shunting. AO = aorta; IVC = inferior vena cava; LA = left atrium; LV = left ventricle; PA = pulmonary artery; PV = pulmonary veins; RA = right atrium; RV = right ventricle; SVC = superior vena cava. |

Symptoms and Signs of TAPVR
Neonates with obstructed pulmonary venous return present with respiratory distress, pulmonary edema, and marked cyanosis. Physical examination usually shows a parasternal lift and a single, loud second heart sound (S2), with no significant murmur.
If pulmonary venous return is not obstructed, mild symptoms of heart failure may be present. Some infants with unobstructed supracardiac or cardiac total anomalous pulmonary venous return may be asymptomatic.
Physical examination detects a hyperdynamic precordium, a widely split S2 sometimes with a loud pulmonary component, and a grade 2 to 3/6 systolic ejection murmur audible along the left sternal border (see table ). A mid-diastolic tricuspid flow murmur may be audible at the lower left sternal border.
Diagnosis of TAPVR
Chest x-ray
Echocardiography
Diagnosis of total anomalous pulmonary venous return is suspected by chest x-ray and established by echocardiography. Cardiac catheterization is rarely necessary; occasionally, cardiac MRI or CT angiography may need to be done to better delineate the anatomy of pulmonary venous return.
Chest x-ray shows a small heart and severe diffuse pulmonary edema when there is pulmonary venous obstruction; otherwise, there is cardiomegaly with increased pulmonary vascular markings. In supracardiac total anomalous pulmonary venous return, the anomalous venous pathway creates a second round shadow above the heart, often likened to the appearance of a snowman.
ECG shows right axis deviation, right ventricular hypertrophy, and occasionally right atrial enlargement.
Treatment of TAPVR
Surgical repair
Medical treatment of heart failure (eg, diuretics, digoxin, angiotensin-converting enzyme inhibitors) before surgery
Neonates with total anomalous pulmonary venous return with obstruction require emergent surgical repair. In older infants, heart failure should be treated, followed by surgical repair as soon as the infant is stabilized.
Surgical repair consists of creating a wide anastomosis between the pulmonary venous confluence and the posterior wall of the left atrium. Ligation of the vein decompressing the confluence into the systemic venous circulation is important to prevent a postoperative left-to-right shunt. The repair is different for return to the coronary sinus, in which case the coronary sinus is unroofed into the left atrium and its opening to the right atrium is closed.
Endocarditis prophylaxis is recommended preoperatively but is required only for the first 6 months after repair unless there is a residual defect adjacent to a surgical patch or prosthetic material.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides overview of common congenital heart defects for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing prophylactic antibiotic use, for patients and caregivers
Drug Information for the Topic





