

Necrotizing enterocolitis is an acquired disease, primarily of preterm or sick neonates, characterized by mucosal or even deeper intestinal necrosis. It is the most common gastrointestinal emergency among neonates. Symptoms and signs include feeding intolerance, lethargy, temperature instability, ileus, bloating, bilious emesis, hematochezia, reducing substances in the stool, apnea, and sometimes signs of sepsis. Diagnosis is clinical and is confirmed by imaging studies. Treatment is primarily supportive and includes nasogastric suction, parenteral fluids, parenteral nutrition, antibiotics, isolation in cases of infection, and, sometimes, surgery.
The vast majority of necrotizing enterocolitis (NEC) cases occur in premature infants, of which 85% weigh < 1.5 kg at birth or are born at < 32 weeks gestational age (1). Incidence of NEC has been reported to vary between 6% and 15% of all neonates admitted to a neonatal intensive care unit (NICU) (2, 3).
Risk factors for necrotizing enterocolitis
General risk factors for NEC in addition to prematurity include the following:
Prolonged rupture of the membranes with amnionitis
Birth asphyxia
Alteration of the intestinal microbiome (dysbiosis)
Non-human milk feeding
Three intestinal factors are usually present:
A preceding ischemic insult
Bacterial colonization
Intraluminal substrate (ie, enteral feedings)
General references
1. Sharma R, Hudak ML. A clinical perspective of necrotizing enterocolitis: past, present, and future. Clin Perinatol. 2013;40(1):27-51. doi:10.1016/j.clp.2012.12.012
2. Alene T, Feleke MG, Yeshambel A, et al. Time to occurrence of necrotizing enterocolitis and its predictors among low birth weight neonates admitted at neonatal intensive care unit of felege hiwot compressive specialized hospital BahirDar, Ethiopia, 2021: A retrospective follow-up study. Front Pediatr. 2022;10:959631, 2022. doi:10.3389/fped.2022.959631
3. Caplan M, Portman R. Second Annual Neonatal Scientific Workshop at the EMA Report. London: International Neonatal Consortium, 2016.
Etiology of Necrotizing Enterocolitis
The exact etiology of NEC is not clear. However, the increased permeability and immature immune function of the immature intestinal tract are predisposing factors. It is believed that an ischemic insult damages the intestinal lining, leading to increased intestinal permeability and leaving the intestine susceptible to bacterial invasion. NEC rarely occurs before enteral feedings have begun and is less common among breastfed (chestfed) infants. However, once feedings are begun, ample substrate is present for proliferation of luminal bacteria, which can penetrate the damaged intestinal wall, producing hydrogen gas. The gas may collect within the intestinal wall (pneumatosis intestinalis) or enter the portal veins. Dysbiosis (alteration of the intestinal microbiome), such as that which occurs after treatment with antibiotics or acid-suppressing medications, may also be a contributing factor because it increases potentially pathogenic bacteria.
The initial ischemic insult may result from vasospasm of the mesenteric arteries, which can be caused by an anoxic insult triggering the primitive diving reflex that markedly diminishes intestinal blood flow. Intestinal ischemia may also result from low blood flow during an exchange transfusion, during sepsis, or from the use of hyperosmolar formulas. Similarly, congenital heart disease with reduced systemic blood flow or arterial oxygen desaturation may lead to intestinal hypoxia/ischemia and predispose to NEC, even in term infants.
NEC may occur as clusters of cases or as outbreaks in neonatal intensive care units. Some clusters appear to be associated with specific organisms (eg, Klebsiella, Escherichia coli, coagulase-negative staphylococci, Pseudomonas, Clostridioides difficile), but often no specific pathogen is identified.
Symptoms and Signs of Necrotizing Enterocolitis
Infants may present with feeding difficulties and bloody or bilious gastric residuals (after feedings) that may progress to bilious emesis, ileus manifested by abdominal distention, discoloration of abdominal skin, or gross blood in stool.
Sepsis may be manifested by lethargy, temperature instability, increased apneic spells, and metabolic acidosis.
Complications of necrotizing enterocolitis
Necrosis begins in the mucosa and may progress to involve the full thickness of the intestinal wall, causing intestinal perforation with subsequent peritonitis and often free intra-abdominal air. Perforation occurs most commonly in the terminal ileum; the colon and the proximal small bowel are involved less frequently.
In retrospective cohort studies, 24 to 42% of infants with NEC developed sepsis (1, 2). In a systematic review, death occurred in approximately 23% of all infants with confirmed NEC, and in 40% of infants weighing < 1000 g (3).
Intestinal strictures are a common long-term complication of NEC, occurring in 10 to 36% of infants who survive the initial event (4). Strictures typically manifest within 2 to 3 months of an NEC episode. Strictures are most commonly noted in the colon, especially on the left side.
Intestinal failure due to short bowel syndrome develops in up to 15 to 35% of infants surgically treated for NEC (3, 5).
Neurodevelopmental disability is also a common long-term complication of NEC, occurring in 25 to 61% of infants (3).
Symptoms and signs references
1. Garg PM, Paschal JL, Ansari MAY, Block D, Inagaki K, Weitkamp JH. Clinical impact of NEC-associated sepsis on outcomes in preterm infants. Pediatr Res. 2022;92(6):1705-1715. doi:10.1038/s41390-022-02034-7
2. Zouari M, Ben Ameur H, Ben Saad N, et al. Predictive Factors for Mortality in Pre-Term Neonates with Necrotizing Enterocolitis: A Retrospective Cohort Study. Surg Infect (Larchmt). 2023;24(1):52-57. doi:10.1089/sur.2022.266
3. Jones IH, Hall NJ. Contemporary Outcomes for Infants with Necrotizing Enterocolitis-A Systematic Review. J Pediatr. 2020;220:86-92.e3. doi:10.1016/j.jpeds.2019.11.011
4. Hau EM, Meyer SC, Berger S, et al. Gastrointestinal sequelae after surgery for necrotising enterocolitis: A systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2019;104(3):F265-F273. doi:10.1136/archdischild-2017-314435
5. Fredriksson F, Engstrand Lilja H. Survival rates for surgically treated necrotising enterocolitis have improved over the last four decades. Acta Paediatr. 2019;108(9):1603-1608. doi:10.1111/apa.14770
Diagnosis of Necrotizing Enterocolitis
Detection of blood in stool
Abdominal radiographs
Ultrasound
Laboratory testing and blood culture
Sometimes, blood is detected in the stool.
Early radiographs may be nonspecific and reveal only ileus. However, a fixed, dilated intestinal loop (sentinel loop) that does not change on repeated radiographs is very concerning for NEC. Radiographic signs diagnostic of NEC are pneumatosis intestinalis and portal vein gas. Pneumoperitoneum indicates bowel perforation and an urgent need for surgery.
Necrotizing enterocolitis may be staged as (1, 2):
Stage 1 (suspected): Mild systemic or gastrointestinal signs with or without bloody stools
Stage 2 (definite or confirmed): Moderate to severe systemic or gastrointestinal signs
Stage 3 (advanced): Severe systemic and gastrointestinal signs, with or without perforation and pneumoperitoneum
Laboratory testing includes complete blood count and inflammatory markers (eg, C-reactive protein, erythrocyte sedimentation rate) as well as blood culture to guide antibiotic therapy.
The differential diagnosis for advanced NEC with perforation includes spontaneous intestinal perforation. Spontaneous intestinal perforation is a distinct condition that also occurs in preterm neonates and that is more localized and occurs without the widespread inflammation seen in NEC (3).

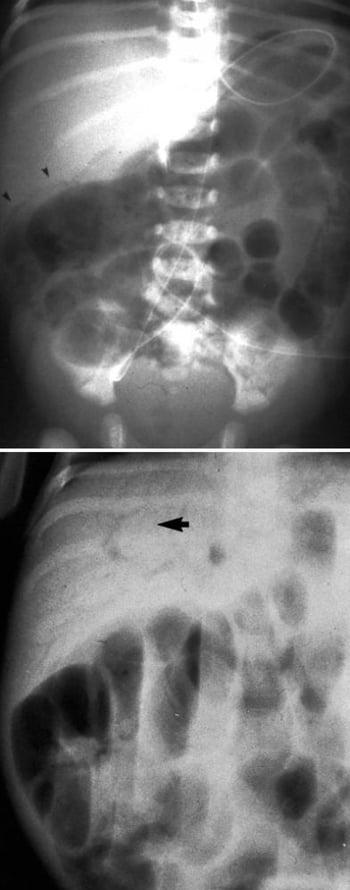
This image shows pneumatosis intestinalis (top, arrowheads) and portal vein gas (bottom, arrow).


This image shows an autopsy specimen with areas of pneumatosis intestinalis, necrotic bowel, and a perforation indicated by the arrow.
CDC/ Dr. Edwin P. Ewing, Jr.
Ultrasound is being used increasingly in cases of NEC. With ultrasound, clinicians have the ability to look at bowel wall thickness, pneumatosis intestinalis, and blood flow. This technique, however, is very operator dependent, and plain radiographs are still more commonly used.
Diagnosis references
1. Juhl SM, Hansen ML, Gormsen M, Skov T, Greisen G. Staging of necrotising enterocolitis by Bell's criteria is supported by a statistical pattern analysis of clinical and radiological variables. Acta Paediatr. 2019;108(5):842-848. doi:10.1111/apa.14469
2. Bell MJ, Ternberg JL, Feigin RD, et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg. 1978;187(1):1-7. doi:10.1097/00000658-197801000-00001
3. Dantes G, Keane OA, Do L, et al. Clinical Predictors of Spontaneous Intestinal Perforation vs Necrotizing Enterocolitis in Extremely and Very Low Birth Weight Neonates. J Pediatr Surg. 2024;59(11):161608. doi:10.1016/j.jpedsurg.2024.06.017
Treatment of Necrotizing Enterocolitis
Feedings stopped
Nasogastric suction
Fluid resuscitation
Broad-spectrum antibiotics
Parenteral nutrition (PN)
Sometimes surgery or percutaneous drainage
The mortality rate is approximately 25% in confirmed cases overall, 35% in infants requiring surgery, and 40% in infants with birthweight < 1 kg (1). Aggressive support and judicious timing of surgical intervention maximize the chance of survival.
Support
Nonsurgical support is sufficient in approximately50 to 75% of cases (2). Feedings must be stopped immediately if NEC is suspected, and the intestine should be decompressed with a double-lumen nasogastric tube attached to intermittent suction. Appropriate colloid and crystalloid parenteral fluids must be given to support circulation because extensive intestinal inflammation and peritonitis may lead to considerable third-space fluid loss.
PN is needed for 10 to 14 days while the intestine heals.
Systemic antibiotics should be started at once with a beta-lactam antibiotic (eg, ampicillin, piperacillin/tazobactam) and an aminoglycoside (eg, gentamicin, amikacin). Additional anaerobic coverage (eg, metronidazole) may also be considered (Systemic antibiotics should be started at once with a beta-lactam antibiotic (eg, ampicillin, piperacillin/tazobactam) and an aminoglycoside (eg, gentamicin, amikacin). Additional anaerobic coverage (eg, metronidazole) may also be considered (3). Antibiotics should be continued for 10 to 14 days. Because some outbreaks may be infectious, patient isolation should be considered, particularly if several cases occur within a short time.
The infant requires close monitoring; frequent complete reevaluation (eg, at least every 12 hours); and serial abdominal radiographs, complete blood counts (CBCs) including platelet counts, and blood gas analysis.
Surgery
Surgical intervention is needed in approximately 25 to 50% of infants (2). Absolute indications are intestinal perforation (pneumoperitoneum), signs of peritonitis (often absent in NEC but include absent intestinal sounds and diffuse guarding and tenderness or erythema and edema of the abdominal wall), or aspiration of purulent material from the peritoneal cavity by paracentesis. Surgery should be considered for an infant with NEC whose clinical and laboratory conditions worsen despite nonsurgical support.
Primary percutaneous peritoneal drainage is an option and can be performed at the bedside. In this procedure, the surgeon makes an incision in the right lower quadrant through which the abdomen is irrigated with warm saline solution. A drain is then placed to allow continued drainage of the abdomen. When drainage has stopped, the drain can be pulled back a little each day and subsequently removed. This procedure is performed more commonly in very sick, extremely low-birth-weight infants (< 1 kg) who would be at risk if taken to an operating room; however, it may be associated with a higher mortality. Some, but not all, patients undergoing percutaneous peritoneal drainage require additional surgery.
For infants undergoing laparotomy, the gangrenous bowel is resected, and ostomies are created. (Primary reanastomosis may be performed if the remaining intestine shows no signs of ischemia.) With resolution of sepsis and peritonitis, intestinal continuity can be reestablished several weeks or months later.
Strictures secondary to NEC require resection.
Treatment references
1. Jones IH, Hall NJ. Contemporary Outcomes for Infants with Necrotizing Enterocolitis-A Systematic Review. J Pediatr. 2020;220:86-92.e3. doi:10.1016/j.jpeds.2019.11.011
2. Robinson JR, Rellinger EJ, Hatch LD, et al. Surgical necrotizing enterocolitis. Semin Perinatol. 2017;41(1):70-79. doi:10.1053/j.semperi.2016.09.020
3. Roberts AG, Younge N, Greenberg RG. Neonatal Necrotizing Enterocolitis: An Update on Pathophysiology, Treatment, and Prevention. Paediatr Drugs. 2024;26(3):259-275. doi:10.1007/s40272-024-00626-w
Prevention of Necrotizing Enterocolitis
At-risk infants should ideally be fed human milk, and feedings should begin with small amounts that are gradually increased according to standardized protocols (1). (Preterm formula is an appropriate substitute if human milk is not available.) Hypertonic formula, medications, or contrast material should be avoided. Anemia, low oxygen saturations, and polycythemia should be treated promptly. In particular, when possible, antibiotics and acid-suppressing medications should be avoided.
Probiotics (eg, Bifidus infantis, Lactobacillus acidophilusLactobacillus acidophilus) help prevent NEC, but further studies to determine optimal dosing and appropriate strains are required before routine use (2, 3).
Corticosteroids may be given to pregnant people who are at risk of preterm birth to help prevent NEC (4).
Prevention references
1. Quigley M, Embleton ND, Meader N, McGuire W. Donor human milk for preventing necrotising enterocolitis in very preterm or very low-birthweight infants. Cochrane Database Syst Rev. 2024;9(9):CD002971. Published 2024 Sep 6. doi:10.1002/14651858.CD002971.pub6
2. van den Akker CHP, van Goudoever JB, Shamir R, et al. Probiotics and preterm infants: A position paper by the European Society for Paediatric Gastroenterology Hepatology and Nutrition Committee on Nutrition and the European Society for Paediatric Gastroenterology Hepatology and Nutrition Working Group for Probiotics and Prebiotics. J Pediatr Gastroenterol Nutr. 2020;70(5):664–680. doi:10.1097/MPG.0000000000002655
3. Razak A, Patel RM, Gautham KS. Use of Probiotics to Prevent Necrotizing Enterocolitis: Evidence to Clinical Practice. JAMA Pediatr. 2021;175(8):773-774. doi:10.1001/jamapediatrics.2021.1077
4. Xiong T, Maheshwari A, Neu J, et al. An overview of systematic reviews of randomized-controlled trials for preventing necrotizing enterocolitis in preterm infants. Neonatology. 2016;13:1–11. doi:10.1159/000504371
Key Points
Necrotizing enterocolitis (NEC) is intestinal necrosis of uncertain etiology; it occurs mainly in preterm or sick neonates after enteral feedings have begun.
Complications include intestinal perforation (most often in the terminal ileum) and peritonitis; sepsis occurs in 24 to 42%, and death occurs in 23%.
Initial manifestations are feeding difficulties and bloody or bilious gastric residuals (after feedings) followed by bilious emesis, abdominal distention or discoloration, and/or gross blood in stool.
Diagnose using plain radiographs.
Supportive treatment using fluid resuscitation, nasogastric suction, broad-spectrum antibiotics, and parenteral nutrition is effective in 50 to 75% of cases.
Surgery to resect gangrenous bowel and treat perforation is needed in approximately 25 to 50% of infants.
Drug Information for the Topic





