





Breast cancer occurs when cells in the breast become abnormal and divide into more cells uncontrollably. Breast cancer usually starts in the glands that produce milk (lobules) or the tubes (ducts) that carry milk from the glands to the nipple.
Among women, breast cancer is one of the most common cancers.
Typically, the first symptom is a painless lump, usually noticed by the woman herself.
If a solid lump is detected, doctors use a hollow needle to remove a sample of tissue or make an incision and remove part or all of the lump and then examine the tissue under a microscope (biopsy).
Breast cancer almost always requires surgery, sometimes with radiation therapy, chemotherapy, other medications, or a combination.
Prognosis depends on the type, size, and spread of the cancer and on other factors.
(See also Overview of Breast Disorders.)

Breast disorders may be noncancerous (benign) or cancerous (malignant). Most are noncancerous. Often, they do not require treatment. In contrast, breast cancer can mean loss of a breast or be life threatening. However, potential problems can often be detected early when women have:
Regular physical examinations by their doctor
Mammograms, as recommended
Women should be familiar with how their breasts normally look and feel. Because breast cancer also affects men, men should be aware of changes in or around their nipples. If a woman notices a change, she may do a breast self-examination. Women should report any changes to a health care professional right away. Most medical organizations no longer recommend that people do monthly or weekly breast self-examinations as a routine way to check for cancer. Doing these examinations when there is no lump or other change does not help detect breast cancer early in women who get regularly scheduled screening mammograms.
Early detection of breast cancer can be essential to successful treatment.
In the United States, breast cancer is the second most common cancer in women (skin cancers are most common). Breast cancer is the second leading cause of cancer death (the most common is lung cancer) across all women, but it is the leading cause of cancer death in Black women. Black women are more likely to die from breast cancer than any other race or ethnicity; Asian and Pacific Islander women have the lowest death rate from breast cancer. (See also American Cancer Society: Key Statistics for Breast Cancer.)
In 2023, in women in the United States, it is estimated there will be
297,790 new cases of invasive breast cancer
55,720 new cases of noninvasive (in situ) breast cancer
43,700 breast cancer deaths
In 2023, in men in the United States, it is estimated there will be 2800 new cases of invasive breast cancer and 530 deaths from it.
Risk Factors for Breast Cancer
Several factors affect the risk of developing breast cancer. Thus, for some women, the risk is much higher or lower than average. Most factors that increase risk, such as age and certain abnormal genes, cannot be changed. For example, 1 of 8 women will develop breast cancer throughout her life. However, the risk is lower in younger women, thus a 40-year-old woman has only about a 1 in 70 chance of developing breast cancer during the next decade. But as she ages, her risk increases.
Regular exercise, particularly during adolescence and young adulthood, may reduce the risk of developing breast cancer.
The most important way to minimize the risks to a woman's health is being vigilant about detecting breast cancer so that it can be diagnosed and treated early, when it is more likely to be cured. Early detection is more likely when women have mammograms.
What Are the Risks of Developing Breast Cancer?
Age (Years) | Risk (%) in 10 Years | Risk (%) in 20 Years | Risk (%) in 30 Years |
|---|---|---|---|
30 | 0.5 | 2.0 | 4.3 |
40 | 1.6 | 3.9 | 7.1 |
50 | 2.4 | 5.7 | 9.1 |
60 | 3.5 | 7.2 | 9.2 |
70 | 4.1 | 6.4 | — |
80 | 3.0 | — | — |
Based on seer.cancer.gov. Accessed on July 31, 2023. | |||
Age
The breast cancer rate in the United States is highest among women ages 65 to 74 years. Median age at diagnosis is 63 years overall; it is slightly younger for Black women (60 years old) compared to White women (63 years old).
Race and ethnicity
Black women have the highest death rate from breast cancer compared with other races or ethnicities. Black, Hispanic, American Indian, and Alaska Native women are more likely to have breast cancer that has spread (metastasized) at time of diagnosis than White, Asian, and Pacific Islander women.
Family history of breast cancer
Women with a first-degree relative (mother, sister, or daughter) who has had breast cancer have double the risk of developing breast cancer. The risk is 3 or 4 times higher if 2 or more first-degree relatives had breast cancer. However, the risk is only slightly higher than average if more-distant relatives (grandmother, aunt, or cousin) have had breast cancer.
Breast cancer gene mutation
Several gene mutations increase the risk of breast cancer. BRCA1 and BRCA2 mutations are present in fewer than 1% of women. These mutations are most common among people with Ashkenazi Jewish ancestry. About 5 to 10% of women with breast cancer have one of these gene mutations. If a woman has one of these mutations, her lifetime risk of developing breast cancer is about 50 to 85%. The risk of developing breast cancer by age 80 is about 72% with a BRCA1 mutation and about 69% with a BRCA2 mutation. However, if such a woman develops breast cancer, her chances of dying of breast cancer are not necessarily greater than those of any other woman with breast cancer.
Having a BRCA mutation also increases the risk of ovarian cancer. During their life, women with BRCA1 gene mutations have about a 40% risk of developing ovarian cancer. For women with BRCA2 gene mutations, risk is about 15%.
Men who have a BRCA gene mutation have a 1 to 2% lifetime risk of developing breast cancer.
Women with one of these mutations need to be monitored more closely for breast cancer—for example, by more frequent testing or being screened with both mammography and magnetic resonance imaging (MRI). Or they may need to try to prevent cancer from developing by taking tamoxifen or having both breasts removed (double mastectomy).
Previous history of breast cancer
Having had breast cancer increases the risk of having another breast cancer. For women who have had a mastectomy to remove 1 breast, the risk of developing cancer in the remaining breast is about 0.4% each year.
Age at first menstrual period, first pregnancy, and menopause
Starting to have menstrual periods at a younger age or starting menopause later than average increases the risk of developing breast cancer. Risk increases with increasing age at first pregnancy.
Benign breast disease
Women who have had certain changes in their breasts seem to have a slightly higher risk of breast cancer. They include
Changes in the breast that required a biopsy to rule out cancer
Conditions that change the structure, increase the number of cells, or cause lumps or other abnormalities in breast tissue, such as complex fibroadenoma, hyperplasia (abnormally increased growth of tissue), atypical hyperplasia (hyperplasia with abnormal tissue structure) in the milk ducts or milk-producing glands, sclerosing adenosis (increased growth of tissue in the milk-producing glands), or papilloma (a noncancerous tumor with fingerlike projections)
For women with such changes, the risk of breast cancer is increased only slightly unless abnormal tissue structure is detected during a biopsy or they have a family history of breast cancer.
Dense breast tissue
Dense breast tissue seen on screening mammography is associated with an increased risk of breast cancer. Having dense breast tissue also makes it harder for doctors to identify breast cancer on a mammogram. Having dense breasts means that women have more fibroglandular tissue (composed of fibrous connective tissue and glands) and less fatty tissue in the breast.
Oral contraceptives (birth control pills)
It is not clear if the use of oral contraceptives increases the risk of breast cancer. Some studies have found a small increased risk in current or recent users.
Hormone therapy
After menopause, taking combination hormone therapy (estrogen with a progestin) for a few years or more increases the risk of breast cancer. Taking estrogen alone does not appear to increase the risk of breast cancer. Taking selective estrogen-receptor modulators (such as raloxifene) reduces the risk of developing breast cancer.
Radiation exposure
Radiation exposure of the chest (such as radiation therapy for cancer) up through 45 years of age increases risk, with the highest increase for those exposed between ages 10 to 14 years.
Diet
It is possible that diet contributes to the development or growth of breast cancers, but evidence about the effect of a particular diet (such as a high-fat diet) is lacking (see also Diet and Cancer).
Obesity
Risk of developing breast cancer is somewhat higher for women who have obesity after menopause.
Research about the link between obesity and cancer is ongoing (see also the National Cancer Institute: Uncovering the Mechanisms Linking Obesity and Cancer Risk).
Smoking and alcohol
Smoking and regularly drinking alcoholic beverages may increase the risk of breast cancer. Experts recommend that women limit themselves to one alcoholic drink a day. One drink is about 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of more concentrated liquor, such as whiskey.
Types of Breast Cancer
Breast cancer is usually classified by the following:
Type of tissue in which the cancer starts
Extent of the cancer's spread
Type of tumor receptors on the cancer cells
Type of tissue
There are many different types of tissue in the breast. Cancer can develop in most of these tissues, including
Milk ducts (called ductal carcinoma)
Milk-producing glands, or lobules (called lobular carcinoma)
Fatty or connection tissue (called sarcoma): This type is rare.
Ductal carcinoma accounts for about 90% of all breast cancers.
Paget disease of the breast is a ductal breast carcinoma that affects the skin over and around the nipple. The first symptom is a crusty or scaly nipple sore or a discharge from the nipple. About half of the women who have this cancer also have a lump in the breast that can be felt. Women with Paget disease of the nipple may also have another breast cancer that is not felt but that can be seen using imaging tests—mammography, magnetic resonance imaging (MRI), or ultrasonography—done to look for another cancer. Because this disease usually causes little discomfort, women may ignore it for a year or more before seeing a doctor. The prognosis depends on how invasive and how large the cancer is as well as whether it has spread to the lymph nodes.


In Paget disease of the nipple, ductal carcinoma in situ extends over the nipple and areola and causes scaling, itching, and burning pain in the affected nipple.
DR M.A. ANSARY/SCIENCE PHOTO LIBRARY
Phyllodes breast tumors are relatively rare, accounting for fewer than 1% of breast cancers. About 10 to 25% are cancerous. They originate in breast tissue around milk ducts and milk-producing glands. The tumor spreads to other parts of the body (metastasizes) in about 10 to 20% of women who have it. It recurs in the breast in about 20 to 35% of women who have had it. The prognosis is good unless the tumor has metastasized.
Extent of spread
Breast cancer can remain within the breast or spread anywhere in the body through the lymphatic vessels or bloodstream. Cancer cells tend to move into the lymphatic vessels in the breast. Most lymphatic vessels in the breast drain into lymph nodes in the armpit (axillary lymph nodes). One function of lymph nodes is to filter out and destroy abnormal or foreign cells, such as cancer cells. If cancer cells get past these lymph nodes, the cancer can spread to other parts of the body.
Breast cancer tends to spread (metastasize) to the bones, brain, lungs, liver, and skin but can spread to any area. Spread to the scalp is uncommon. Breast cancer can appear in these areas years or even decades after it is first diagnosed and treated. If the cancer has spread to one area, it probably has spread to other areas, even if it cannot be detected right away.
Breast cancer can be classified as
Carcinoma in situ
Invasive cancer
Carcinoma in situ means cancer in place. It is the earliest stage of breast cancer. Carcinoma in situ may be large and may even affect a substantial area of the breast, but it has not invaded the surrounding tissues or spread to other parts of the body.
Ductal carcinoma in situ is confined to the milk ducts of the breast. It does not invade surrounding breast tissue, but it can spread along the ducts and gradually affect a substantial area of the breast. This type accounts for 85% of carcinoma in situ and at least half of breast cancers. It is detected most often by mammography. This type may become invasive.
Lobular carcinoma in situ develops within the milk-producing glands of the breast (lobules). It often occurs in several areas of both breasts. Women with lobular carcinoma in situ have a 1 to 2% chance each year of developing invasive breast cancer in the affected or the other breast. Usually, lobular carcinoma in situ cannot be seen on a mammogram and is detected only by biopsy. There are two types of lobular carcinoma in situ: classic and pleomorphic. The classic type is not invasive, but having it increases the risk of developing invasive cancer in either breast. The pleomorphic type leads to invasive cancer and, when detected, is surgically removed.
Invasive cancer can be classified as follows:
Localized: The cancer is confined to the breast.
Regional: The cancer has invaded tissues near the breasts, such as the chest wall or lymph nodes.
Distant (metastatic): The cancer has spread from the breast to other parts of the body (metastasized).
Invasive ductal carcinoma begins in the milk ducts but breaks through the wall of the ducts, invading the surrounding breast tissue. It can also spread to other parts of the body. It accounts for about 75% of invasive breast cancers.
Invasive lobular carcinoma begins in the milk-producing glands of the breast but invades surrounding breast tissue and spreads to other parts of the body. It is more likely than other types of breast cancer to occur in both breasts. It accounts for most of the rest of invasive breast cancers.
Rare types of invasive breast cancers include
Medullary carcinoma
Tubular carcinoma
Metaplastic carcinoma
Mucinous carcinoma
Rare types that typically have a poor prognosis include metaplastic and inflammatory breast cancer. Rare types that are usually associated with a favorable prognosis include medullary, mucinous, cribriform, and tubular carcinomas. Mucinous carcinoma tends to develop in older women and be slow growing.
Tumor receptors
All cells, including breast cancer cells, have molecules on their surfaces called receptors. A receptor has a specific structure that allows only particular substances to fit into it and thus affect the cell’s activity. Whether breast cancer cells have certain receptors affects how quickly the cancer spreads and how it should be treated.
Tumor receptors include the following:
Estrogen and progesterone receptors: Some breast cancer cells have receptors for estrogen. The resulting cancer, described as estrogen receptor–positive, grows or spreads when stimulated by estrogen. Approximately 80% of postmenopausal and 20% of premenopausal women with breast cancer have estrogen receptor–positive cancer. Some breast cancer cells have receptors for progesterone. The resulting cancer, described as progesterone receptor–positive, is stimulated by progesterone. Approximately 70% of all breast cancers are progesterone receptor–positive. Breast cancers with estrogen receptors and possibly those with progesterone receptors grow more slowly than those that do not have these receptors, and the prognosis is better. (Estrogen and progesterone are female sex hormones.)
HER2 (also called HER2/neu) receptors: Normal breast cells have HER2 receptors, which help them grow. (HER stands for human epithelial growth factor receptor, which is involved in multiplication, survival, and differentiation of cells.) In about 15% of breast cancers, cancer cells have too many HER2 receptors. Such cancers tend to be very fast growing.
Other characteristics
Sometimes cancer is also classified based on other characteristics.
Inflammatory breast cancer is an example. The name refers to the symptoms of the cancer rather than the affected tissue. This type is fast growing, particularly aggressive, and often fatal. Cancer cells block the lymphatic vessels in the skin of the breast, causing the breast to appear inflamed: swollen, red, and warm. Usually, inflammatory breast cancer spreads to the lymph nodes in the armpit. The lymph nodes can be felt as hard lumps. However, often no lump may be felt in the breast itself because this cancer is dispersed throughout the breast. Inflammatory breast cancer accounts for about 1% of breast cancers.
Symptoms of Breast Cancer
At first, breast cancer usually causes no symptoms. The most common way it is discovered is when a woman (or a health care professional) finds a painless breast lump.
Some women with breast cancer have breast pain, but breast pain has many causes and usually does not mean that a woman has breast cancer. Pain without a lump is rarely due to breast cancer.
Bloody nipple discharge, especially from only one breast rather than both, may be a symptom of breast cancer.
If a woman has a breast lump that does not go away after a few days or has bloody nipple discharge, she should have the lump evaluated by a health care professional.
A breast lump usually feels distinctly different from the surrounding breast tissue. A breast lump that is potentially cancerous is often a firm, distinctive thickening that appears in one breast but not the other. However, noncancerous lumps (such as fibroadenomas) may have the same characteristics. Usually, scattered lumpy changes in the breast, especially the upper outer region, are not cancerous and indicate fibrocystic changes.
In the early stages, the lump may move freely beneath the skin when it is pushed with the fingers.
In more advanced stages, the lump usually becomes attached to the chest wall or the skin over it. In these cases, the lump cannot be moved at all or it cannot be moved separately from the skin over it. A woman can check if a lump is attached to surrounding tissue by lifting her arms over her head while standing in front of a mirror. If a breast contains a lump that is attached to the chest wall or skin, this maneuver may make the skin pucker or dimple or make one breast appear different from the other.
In very advanced cancer, swollen bumps or festering sores may develop on the skin. Sometimes the skin over the lump is dimpled and leathery and the texture (but not the color) looks like the skin of an orange (peau d’orange).
If the cancer has spread, lymph nodes, particularly those in the armpit on the affected side, may feel like hard small lumps. The lymph nodes may be stuck together or become attached to the skin or chest wall. They are usually painless but may be slightly tender. Enlarged lymph nodes in the armpit may also occur for noncancerous reasons, such as an infection.
Occasionally, the first symptoms occur only when the cancer spreads to another organ. For example, if breast cancer spreads to a bone, the bone may ache or become weak, resulting in a fracture. If the cancer spreads to a lung, women may cough or have difficulty breathing.
In Paget disease of the breast, the first symptom is a crusty or scaly nipple sore or a discharge from the nipple. These changes may appear harmless, so women may not think they need to see a health care professional. Many women who have this cancer also have a lump in the breast.
In inflammatory breast cancer, the breast is warm, red, and swollen, as if infected (but it is not). The skin of the breast may become dimpled and leathery, like the skin of an orange, or may have ridges. The nipple may turn inward (invert). A discharge from the nipple is common. Often, no lump can be felt in the breast, but the entire breast is enlarged.


In inflammatory breast cancer, the breast is red and swollen.
MID ESSEX HOSPITAL SERVICES NHS TRUST/SCIENCE PHOTO LIBRARY


Sometimes in inflammatory breast cancer and very advanced cancers, the skin on the breast becomes dimpled and leathery and looks like the skin of an orange (peau d’orange) except in color.
"Creative Commons Patient with inflammatory breast cancer" by Epidemiology and surgical management of breast cancer in gynecological department of Douala General Hospital (Scientific Figure on ResearchGate) is licensed under Creative Commons 2.0. Available from: https://www.researchgate.net/figure/Patient-with-inflammatory-breast-cancer_fig2_234162338 [accessed 3 Oct, 2019].
Diagnosis of Breast Cancer
Initial detection with mammography and/or other imaging (breast tomosynthesis, ultrasonography, magnetic resonance imaging [MRI]) or clinical breast examination
Biopsy
Symptoms, breast examination by a health care professional, or results of a screening mammogram may prompt a diagnostic evaluation for breast cancer.
Several imaging tests can be used to evaluate for breast cancer. The type of imaging test done first depends on the symptoms and results of a physical examination and sometimes on other factors.
If a screening mammogram (or MRI) has a finding suggestive of cancer, a biopsy is usually the next step. Some women at high risk of breast cancer are screened with both mammography and MRI.
When a woman goes to see a health care professional because of symptoms or changes in the breast (such as a lump, nipple discharge, or tenderness), and if changes are found during a physical examination, ultrasonography is usually done first to distinguish between a breast cyst (fluid-filled sac) and a solid lump. This distinction is important because cysts are usually not cancerous. If results of ultrasonography are abnormal or inconclusive, mammography is done as a follow-up step.
Only about 10 to 15% of the abnormalities detected during routine screening with mammography turn out to be cancer.
Even if imaging tests are negative, a biopsy is done if a lump or other findings suggest cancer.
Breast biopsy
All abnormalities that suggest cancer are biopsied.
Doctors may do one of several types of biopsy:
Core needle biopsy: A wide, hollow needle with a special tip is used to remove a sample of breast tissue.
Open (surgical) biopsy: Doctors make a small cut in the skin and breast tissue and remove part or all of a lump. This type of biopsy is done when a needle biopsy is not possible. It may also be done after a needle biopsy that does not detect cancer to be sure that the needle biopsy did not miss a cancer.
Imaging is often done during a biopsy to help doctors determine where to place the biopsy needle.
Imaging may also be done to guide the biopsy. This improves the accuracy of a core needle biopsy. For example, for a mass (whether felt or seen on a mammogram), ultrasonography is used during the core needle biopsy to accurately target the abnormal tissue. When imaging is used to guide placement of the needle, a clip to mark the spot is typically placed during the biopsy.
When an abnormality is seen only on an MRI, then MRI is used to guide the placement of the biopsy needle.
A stereotactic core biopsy is a type of image-guided biopsy. It is useful when there are abnormal patterns of tiny calcium deposits (called microcalcifications) in the breast. This type of biopsy helps doctors accurately locate and remove a sample of the abnormal tissue. For a stereotactic biopsy, doctors take mammograms from two angles and send the two-dimensional images to a computer. The computer compares them and calculates the precise location of the abnormality in three dimensions. The breast tissue to be biopsied by stereotactic core biopsy is x-rayed to make sure doctors get a sample of the abnormal microcalcifications.
Most women do not need to be hospitalized for these procedures. Usually, only a local anesthetic is needed.
A pathologist (a type of doctor who examines biopsy tissue) examines the biopsy samples under the microscope to determine whether cancer cells are present.
Evaluation after cancer diagnosis
If cancer is diagnosed, women are seen by cancer specialists (oncologists), which may include surgeons, medical oncologists (chemotherapy specialists), and radiation oncologists. These doctors determine which tests should be done and plan treatment.
If cancer cells are detected, the biopsy sample is analyzed to determine the characteristics of the cancer cells, such as
Whether the cancer cells have hormone (estrogen or progesterone) receptors
How many HER2 receptors are present
How quickly the cancer cells are dividing
For some types of breast cancer, genetic testing of the cancer cells (multigene panels)
This information helps doctors estimate how rapidly the cancer may spread and which treatments are more likely to be effective.

After breast cancer is diagnosed, tests may include
A chest x-ray to determine whether the cancer has spread
Blood tests, including a complete blood count (CBC), liver tests, and measurement of calcium, also to determine whether the cancer has spread
In women with risk factors for inherited genes that increase the risk of breast cancer (such as BRCA genes), analysis of blood or saliva to check for these genes
Sometimes bone scanning (imaging of bones throughout the body), computed tomography (CT) of the abdomen and chest, and MRI
Sometimes blood tests to measure substances produced by cancer cells (cancer markers)
The National Comprehensive Cancer Network (NCCN) recommends that some women with a current or personal history of breast cancer should be tested for inherited gene mutations that make breast cancer more likely. Some experts have recommended that genetic testing be offered to all patients with breast cancer. For genetic testing, doctors may refer women to a genetic counselor, who can document a detailed family history (including all relatives who have had cancer), choose the most appropriate tests, and help interpret the results.
Staging of Breast Cancer
When cancer is diagnosed, a stage is assigned to it. The stage is a number from 0 to IV (sometimes with substages indicated by letters) that reflects how extensive and aggressive the cancer is:
Stage 0 is assigned to in situ breast cancers, such as ductal carcinoma in situ. In situ means cancer in place. That is, the cancer has not invaded surrounding tissues or spread to other parts of the body.
Stages I through III are assigned to cancer that has spread to tissues within or near the breast (localized or regional breast cancer).
Stage IV is assigned to metastatic breast cancer (cancer that has spread from the breast and lymph nodes in the armpit to other parts of the body).
Staging the cancer helps doctors determine the appropriate treatment and the prognosis.
Many factors go into determining the stage of breast cancer, such as the following:
How large the cancer is
Whether cancer has spread to the lymph nodes
Whether it has spread (metastasized) to other organs, such as the lungs or brain
Other important staging factors include the following:
Grade: How abnormal the cancer cells look under a microscope, scored from 1 to 3
Hormone receptor status: Whether the cancer cells have estrogen, progesterone, and/or HER2 receptors
Genetic testing of the cancer (such as the Oncotype DX test): For some breast cancers, how many and which abnormal genes are present in the cancer
Grade varies because although all cancer cells look abnormal, some look more abnormal than others. If the cancer cells do not look very different from normal cells, the cancer is considered well-differentiated. If the cancer cells look very abnormal, they are considered undifferentiated or poorly differentiated. Well-differentiated cancers tend to grow and spread more slowly than undifferentiated or poorly differentiated cancers. Based on these and other differences in microscopic appearance, doctors assign a grade to most cancers.
The presence of hormone receptors and gene mutations in the cancer cells affect how the cancer responds to different treatments and what the prognosis is.
Treatment of Breast Cancer
Surgery
Radiation therapy
Systemic (body-wide) chemotherapy
Hormone blockers (medications that affect hormones)
Treatment for breast cancer begins after the woman’s condition has been thoroughly evaluated.
Treatment options depend on the stage and type of breast cancer and the receptors that the cancer has. However, treatment is complex because the different types of breast cancer differ greatly in characteristics such as growth rate, tendency to spread (metastasize), and response to various treatments. Also, much is still unknown about breast cancer. Consequently, doctors may have different opinions about the most appropriate treatment for a particular woman.
The preferences of a woman and her doctor affect treatment decisions (shared decision-making). Women with breast cancer should ask for a clear explanation of what is known about the cancer and what is still unknown, as well as a complete description of treatment options. Then, they can consider the advantages and disadvantages of the different treatments and accept or reject the options offered.
Doctors may ask women with breast cancer to participate in research studies investigating a new treatment. New treatments aim to improve the chances of survival or quality of life. Women should ask their doctor to explain the risks and possible benefits of participation, so that they can make a well-informed decision.
Treatment usually involves surgery and often includes radiation therapy and chemotherapy or hormone blockers. Sometimes a woman can choose whether surgery will involve removing part or all of one or both breasts. Women may be referred to a plastic or reconstruction surgeon, who can remove the cancer and reconstruct the breast in the same operation.
Surgery
The cancerous tumor and varying amounts of the surrounding tissue are removed. There are two main options for removing the tumor:
Breast-conserving surgery plus radiation therapy
Removal of the breast (mastectomy)
For women with invasive cancer (stage I or higher), mastectomy is no more effective than breast-conserving surgery plus radiation therapy as long as the entire tumor can be removed during breast-conserving surgery. In breast-conserving surgery, doctors remove the tumor plus some surrounding normal tissue to reduce the risk that tissue that may contain cancer is left behind.
Before surgery, chemotherapy may be used to shrink the tumor before removing it. This approach sometimes enables some women to have breast-conserving surgery rather than mastectomy.
Breast-conserving surgery
Breast-conserving surgery leaves as much of the breast intact as possible. When considering the type of surgery, it is more important for doctors to be sure they remove the whole cancer than to risk leaving tissue that may contain cancer.
For breast-conserving surgery, doctors first determine how big the tumor is and how much tissue around it (called margins) needs to be removed. The size of the margins is based on how big the tumor is in relation to the breast. Then the tumor with its margins is surgically removed. Tissue from the margins is examined under a microscope to check for cancer cells that have spread outside the tumor. These findings help doctors decide on whether further treatment is needed.
Various terms (for example, lumpectomy, wide excision, quadrantectomy) are used to describe how much breast tissue is removed.
Breast-conserving surgery is usually followed by radiation therapy.
The main advantages of breast-conserving surgery are the possibility of preserving breast tissue and how the breast appears after surgery. When the tumor is large in relation to the breast, this type of surgery is less likely to be useful. In such cases, removing the tumor plus some surrounding normal tissue means removing most of the breast. Breast-conserving surgery is usually more appropriate when tumors are small. In about 15% of women who have breast-conserving surgery, the amount of tissue removed is so small that little difference can be seen between the treated and untreated breasts. However, in most women, the treated breast shrinks somewhat and may change in contour.
If either breast-conserving surgery or mastectomy is an option, a woman should consider each option. Some women prefer breast-conserving surgery because they feel that losing a breast would be a very difficult emotional and physical experience and that breast-conserving surgery helps preserve body image. Other women prefer mastectomy because they feel more comfortable having all the breast tissue removed or because if they have a mastectomy, they may not need radiation therapy.
Chemotherapy, given to shrink the tumor before removing it, may enable some women to have breast-conserving surgery rather than a mastectomy.
Mastectomy
Mastectomy is the other main surgical option. There are several types. In all types, all breast tissue is removed, but which other tissues and how much of them are left in place or removed vary by type:
Skin-sparing mastectomy leaves the muscle under the breast and enough skin to cover the wound. Reconstruction of the breast is much easier if these tissues are left. The lymph nodes in the armpit are not removed.
Nipple-sparing mastectomy is the same as skin-sparing mastectomy plus it leaves the nipple and the area of pigmented skin around the nipple (areola).
Simple mastectomy leaves the muscle under the breast (pectoral muscle) and the lymph nodes in the armpit.
Modified radical mastectomy consists of removing some lymph nodes in the armpit but leaves the muscle under the breast.
Radical mastectomy consists of removing the lymph nodes in the armpit and the muscle under the breast. This procedure is rarely done now unless the cancer has invaded the muscle under the breast.
Lymph node assessment
Doctors assess lymph nodes to determine whether cancer has spread to the lymph nodes in the armpit. If cancer is detected in these lymph nodes, it is more likely to have spread to other parts of the body. In such cases, different treatment may be needed.
A network of lymphatic vessels and lymph nodes (lymphatic system) drain fluid from the tissue in the breast (and other areas of the body). Lymph nodes trap foreign or abnormal cells (such as bacteria or cancer cells) that may be contained in this fluid. Thus, breast cancer cells often end up in lymph nodes near the breast, such as those in the armpit. Usually, foreign and abnormal cells are then destroyed. However, the cancer cells sometimes continue to grow in the lymph nodes or pass through the nodes into the lymphatic vessels and spread to other parts of the body.
Doctors first feel the armpit to check for enlarged lymph nodes. Depending on what doctors find, they may do one or more of the following:
Ultrasonography to check for lymph nodes that may be enlarged
A biopsy (by removing a lymph node or taking a sample of tissue with a needle using ultrasonography to guide placement of the needle)
Axillary lymph node dissection: Removal of many (typically 10 to 20) lymph nodes in the armpit
Sentinel lymph node dissection: Removal of only the lymph node or nodes that cancer cells are most likely to spread to
If doctors feel an enlarged lymph node in the armpit or are uncertain whether lymph nodes are enlarged, ultrasonography is done. If an enlarged lymph node is detected, a needle is inserted into it to remove a sample of tissue to be examined (fine-needle aspiration or core needle biopsy). Ultrasonography is used to guide placement of the needle.
If the biopsy detects cancer, surgical removal of lymph nodes from the armpit (axillary lymph node dissection) may be needed. Removing many lymph nodes in the armpit, even if they contain cancer, does not help cure the cancer. However, it does help doctors decide what treatment to use. Axillary lymph nodes are evaluated again after chemotherapy is given before surgery (called neoadjuvant chemotherapy).
If the biopsy after ultrasonography does not detect cancer, a sentinel lymph node biopsy is done because even if there are no cancer cells in a biopsy sample, cancer cells may be present in other parts of a lymph node. A sentinel lymph node biopsy is usually done as part of the operation to remove the cancer, such as lumpectomy or mastectomy. It enables doctors to identify and test the most important lymph node related to a breast cancer. If that lymph node is not cancerous, a woman does not need a more extensive surgery to remove all axillary lymph nodes.
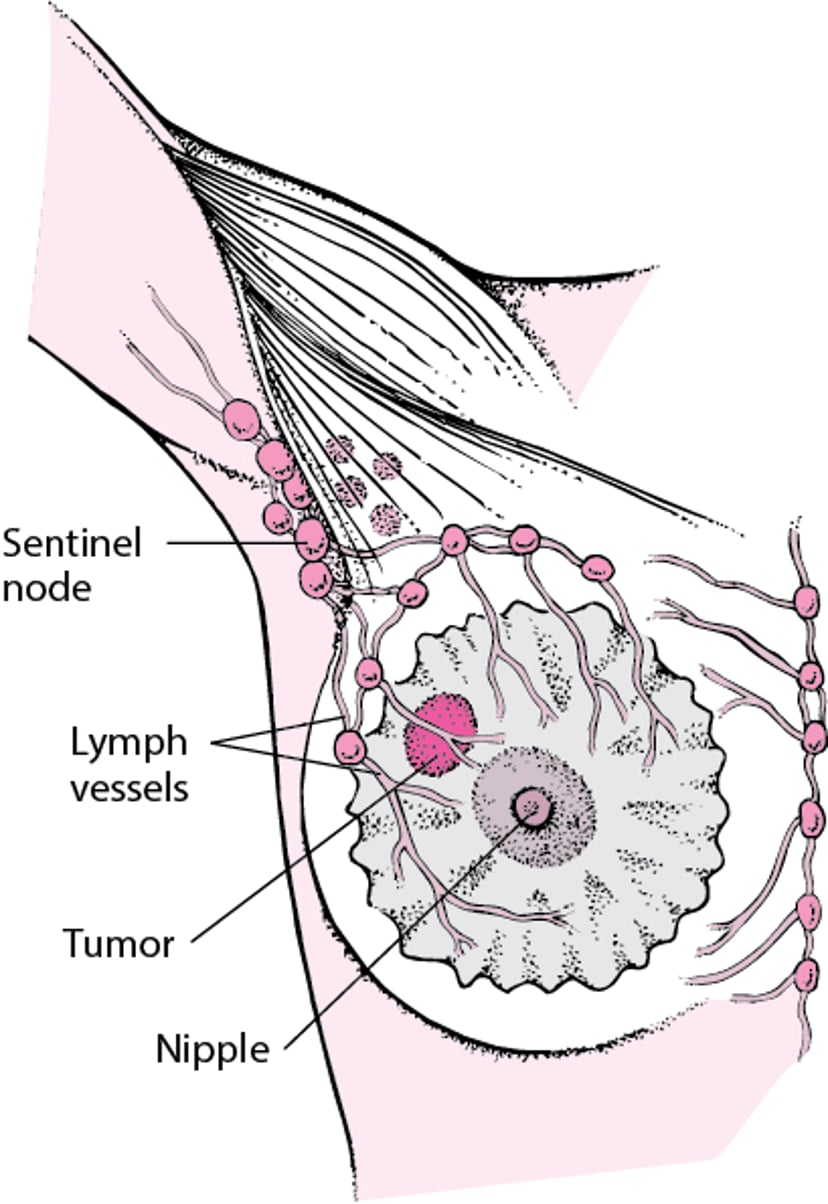
For a sentinel lymph node biopsy, doctors inject a blue dye and/or a radioactive substance into the breast. These substances map the pathway from the breast to the first lymph node (or nodes) in the armpit. Doctors then make a small incision in the armpit and look for a lymph node that looks blue and/or gives off a radioactive signal (detected by a handheld device). This lymph node is the one that cancer cells are most likely to have spread to. This node is called a sentinel lymph node because it is the first to warn that cancer has spread. Doctors remove this node and send it to a laboratory to be checked for cancer. More than one lymph node may look blue and/or give off a radioactive signal and thus be considered a sentinel lymph node.
If the sentinel lymph nodes do not contain cancer cells, no other lymph nodes are removed.
If the sentinel nodes contain cancer, axillary lymph node dissection may be done, depending on various factors, such as
Whether a mastectomy is planned
How many sentinel nodes are present and whether the cancer has spread outside the nodes
Sometimes during surgery to remove the tumor, doctors discover that the cancer has spread to the lymph nodes, and axillary lymph node dissection is required. Before the surgery is done, women may be asked whether they are willing to let the surgeon do more extensive surgery if cancer has spread to the lymph nodes. Otherwise, a second surgical procedure, if needed, is done later.
Removal of lymph nodes often causes problems because it affects the drainage of fluids in tissues. As a result, fluids may accumulate, causing persistent swelling (lymphedema) of the arm or hand. After surgery, the risk of developing lymphedema continues throughout life. Arm and shoulder movement may be limited, requiring physical therapy. The more lymph nodes removed, the worse the lymphedema. Sentinel lymph node biopsy causes less lymphedema than axillary lymph node dissection.
If lymphedema develops, it is treated by specially trained therapists. They teach women how to massage the area, which may help the accumulated fluid drain, and how to apply a bandage, which helps keep fluid from reaccumulating. The affected arm should be used as normally as possible, except that the unaffected arm should be used for heavy lifting. Women should exercise the affected arm daily as instructed and bandage it overnight indefinitely.
If lymph nodes have been removed, women may be advised to ask health care professionals not to insert catheters or needles in veins in the affected arm and not to measure blood pressure in that arm. These procedures makes lymphedema more likely to develop or worsen. Women are also advised to wear gloves whenever they are doing work that may scratch or injure the skin of the hand and arm on the side of the surgery. Avoiding injuries and infections can help reduce the risk of developing lymphedema.
Other problems that may occur after lymph nodes are removed include temporary or persistent numbness, a persistent burning sensation, and infection.
What Is a Sentinel Lymph Node?
A network of lymphatic vessels and lymph nodes drain fluid from the tissue in the breast. The lymph nodes are designed to trap foreign or abnormal cells (such as bacteria or cancer cells) that may be contained in this fluid. Sometimes cancer cells pass through the nodes into the lymphatic vessels and spread to other parts of the body. Although fluid from breast tissue eventually drains to many lymph nodes, the fluid usually drains first through one or only a few nearby lymph nodes. Such lymph nodes are called sentinel lymph nodes because they are the first to warn that cancer has spread. |

Breast reconstruction surgery
Breast reconstruction surgery may be done at the same time as a mastectomy or later.
Women should consult with a plastic surgeon early during treatment to plan the breast reconstruction surgery. When reconstruction is done depends not only on the woman's preference but also on the other treatments needed. For example, if radiation therapy is done before reconstruction surgery, reconstruction options are limited. Oncoplastic breast surgery, which combines cancer (oncologic) surgery and plastic surgery, is one option. This type of surgery is designed to remove all cancer from the breast and preserve or restore the natural appearance of the breast.
Most often, the surgery is done by
Inserting an implant (made of silicone or saline)
Reconstructing the breast using tissue taken from other parts of the woman’s body
Surgeons often obtain tissue for breast reconstruction from a muscle in the lower abdomen. Alternatively, skin and fatty tissue (instead of muscle) from the lower abdomen can be used to reconstruct the breast.
Before inserting an implant, doctors use a tissue expander, which resembles a balloon, to stretch the remaining chest skin and muscle to make room for the breast implant. The tissue expander is placed under the chest muscle during mastectomy. The expander has a small valve that health care professionals can access by inserting a needle through the skin. Over the next several weeks, a salt solution (saline) is periodically injected through the valve to expand the expander a little at a time. After expansion is complete, the expander is surgically removed, and the implant is inserted.
Alternatively, tissues taken from the woman's body (such as muscle and tissues under the skin) can be used for reconstruction. These tissues are taken from the abdomen, back, or buttock and moved to the chest area to create the shape of a breast.
The nipple and surrounding skin are usually reconstructed in a separate operation done later. Various techniques can be used. They include using tissue from the woman's body and tattooing.
Surgery may also be done to modify (augment, reduce, or lift) the other breast to make both breasts match.
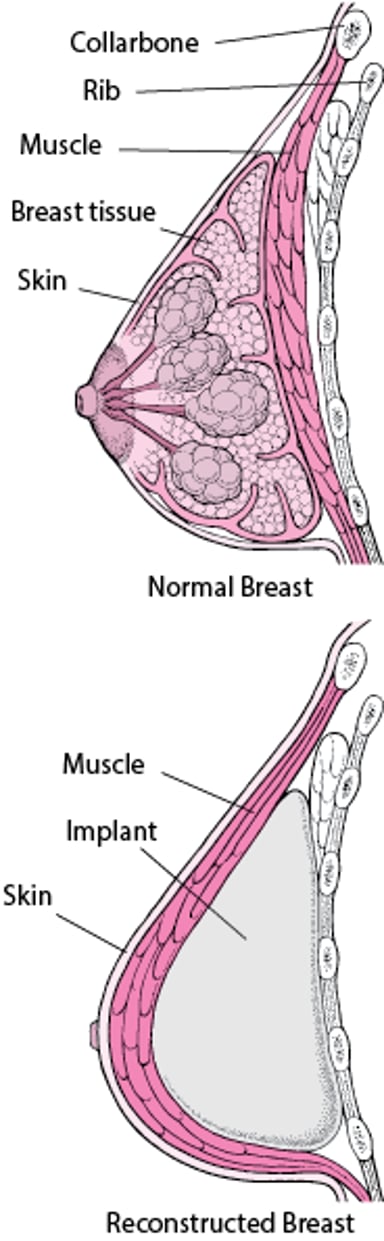
Rebuilding a Breast
After a general surgeon removes a breast tumor and the surrounding breast tissue (mastectomy), a plastic surgeon may reconstruct the breast. A silicone or saline implant may be used. Or in a more complex operation, tissue may be taken from other parts of the woman’s body, such as the abdomen, buttock, or back. Reconstruction may be done at the same time as the mastectomy—a choice that involves being under anesthesia for a longer time—or later—a choice that involves being under anesthesia a second time. Reconstruction of the nipple and surrounding skin is done later, often in a doctor's office. A general anesthetic is not required. In many women, a reconstructed breast looks more natural than one that has been treated with radiation therapy, especially if the tumor was large. If a silicone or saline implant is used and enough skin was left to cover it, the sensation in the skin over the implant is relatively normal. However, neither type of implant feels like breast tissue to the touch. If skin from other parts of the body is used to cover the breast, much of the sensation is lost. However, tissue from other parts of the body feels more like breast tissue than does a silicone or saline implant. Silicone occasionally leaks out of its sack. As a result, an implant can become hard, cause discomfort, and appear less attractive. Also, silicone sometimes enters the bloodstream. Some women are concerned about whether the leaking silicone causes cancer in other parts of the body or rare diseases such as systemic lupus erythematosus (lupus). There is almost no evidence suggesting that silicone leakage has these serious effects, but because it might, the use of silicone implants has decreased, especially among women who have not had breast cancer. |

Removal of the Breast Without Cancer
Certain women with breast cancer have a high risk of developing breast cancer in their other breast (the one without cancer). Doctors may suggest that these women have the other breast removed before cancer develops in it. This procedure is called contralateral (opposite side) prophylactic (preventive) mastectomy. This preventive surgery may be appropriate for women with any of the following:
An inherited genetic mutation that increases the risk of developing breast cancer (such as the BRCA1 or BRCA2 mutation)
At least two close, usually first-degree relatives who have had breast or ovarian cancer
Radiation therapy directed at the chest when women were under 30 years old
Lobular carcinoma in situ (a noninvasive type)
In women with lobular carcinoma in situ in one breast, invasive cancer is equally likely to develop in either breast. Thus, the only way to eliminate the risk of breast cancer for these women is to remove both breasts. Some women, particularly those who are at high risk of developing invasive breast cancer, choose this option.
Advantages of contralateral prophylactic mastectomy include the following:
Longer survival for women with breast cancer and a genetic mutation that increases risk and possibly for women who are under 50 years old when they are diagnosed with breast cancer
Decreased need for cumbersome follow-up imaging tests after treatment
For some women, decreased anxiety
Disadvantages of this procedure include the following:
Twice the risk of complications
Instead of having a contralateral prophylactic mastectomy, some women may choose to have their doctor monitor the breast closely for cancer—for example with imaging tests.
Radiation Therapy
Radiation therapy is used to kill cancer cells at and near the site from which the tumor was removed, including nearby lymph nodes.
Radiation therapy after mastectomy is done if the following are present:
The tumor is 5 centimeters (about 2 inches) or larger.
The cancer has spread to one or more lymph nodes.
In such cases, radiation therapy after mastectomy reduces the incidence of cancer recurring on the chest wall and in nearby lymph nodes, and it improves the chances of survival.
Radiation therapy after breast-conserving surgery significantly reduces the incidence of breast cancer recurring near the original tumor and in nearby lymph nodes, and it may improve overall survival. However, if women are over 70 have a lumpectomy and the cancer has estrogen receptors, radiation therapy may not be necessary because it does not significantly reduce the risk of recurrence or improve the chances of survival in these women.
Side effects of radiation therapy include swelling in the breast, reddening and blistering of the skin in the treated area, and fatigue. These effects usually disappear within several months up to about 12 months. Fewer than 5% of women treated with radiation therapy have rib fractures that cause minor discomfort. In about 1% of women, the lungs become mildly inflamed 6 to 18 months after radiation therapy is completed. Inflammation causes a dry cough and shortness of breath during physical activity that last for up to about 6 weeks. Lymphedema may develop after radiation therapy.
Chemotherapy and hormone blockers (tamoxifen and aromatase inhibitors)
Chemotherapy and hormone blockers (medications that affect hormones, such as tamoxifen or aromatase inhibitors) can suppress the growth of cancer cells throughout the body.
To decide whether to treat with chemotherapy, doctors evaluate a few factors about a woman and the breast cancer and discuss the risks and benefits with her. Factors that doctors consider include
Whether cancer has spread to lymph nodes
Whether a woman is premenopausal or postmenopausal
What the results of tests for estrogen receptors and progesterone receptors are
What the results of tests for the human epidermal growth factor 2 (HER2) oncogene are
Genetic testing of the cancer (such as the Oncotype DX test)
For women with invasive breast cancer, chemotherapy and/or hormone blockers are usually begun soon after surgery. These medications are continued for months or years. Some, such as tamoxifen, may be continued for 5 to 10 years. If tumors are larger than 5 centimeters (about 2 inches), chemotherapy or hormone blockers may be started before surgery. These medications delay or prevent the recurrence of cancer in most women and prolong survival in some.
Analyzing the genetic material of the cancer (predictive genomic testing) may help predict which cancers are susceptible to chemotherapy or hormone blockers.
If women have a breast cancer with estrogen and progesterone receptors but no HER2 receptors and the lymph nodes are not affected, they may not need chemotherapy. Hormone blockers alone may be sufficient.
Hormone blockers (endocrine therapy)
Hormone blockers uses medications that interfere with the actions of estrogen or progesterone, which stimulate the growth of cancer cells that have estrogen and/or progesterone receptors. Hormone blockers may be used when cancer cells have these receptors, sometimes instead of chemotherapy. The benefits of hormone blockers are greatest when cancer cells have both estrogen and progesterone receptors and are almost as great when only estrogen receptors are present. The benefit is minimal when only progesterone receptors are present.
Medications used for endocrine therapy include tamoxifen and aromatase inhibitors.
Tamoxifen:Tamoxifen, which is given by mouth, is a selective estrogen-receptor modulator. It binds with estrogen receptors and prevents stimulation of breast tissue by estrogen. In women who have estrogen receptor–positive cancer, tamoxifen, taken for 5 years, increases the likelihood of survival by about 25%, and 10 years of treatment may be even more effective. Tamoxifen increases the risk of blood clots in the legs and lungs. It also increases the tendency to form polyps in the lining of the uterus (endometrial polyps), which can cause abnormal uterine bleeding, and the risk of developing cancer of the uterus (endometrial cancer). Thus, if a woman taking tamoxifen has an abnormal vaginal bleeding pattern, she should see her doctor.
Aromatase inhibitors: These medications (anastrozole, exemestane, and letrozole) inhibit aromatase (an enzyme that converts some hormones to estrogen) and thus reduce blood levels of estrogen. In postmenopausal women, these medications may be more effective than tamoxifen. Aromatase inhibitors may increase the risk of osteoporosis and fractures and often cause vaginal dryness. Sometimes premenopausal women are treated with a medication to suppress ovarian function (such as leuprolide) combined with an aromatase inhibitor; this is called ovarian suppression.
Chemotherapy
Chemotherapy is used to kill rapidly multiplying cells or slow their multiplication. Chemotherapy alone cannot cure breast cancer. It must be used with surgery or radiation therapy. Chemotherapy is usually given intravenously in cycles. Sometimes they are given by mouth. Typically, a day of treatment is followed by 2 or more weeks of recovery. Using several chemotherapy drugs together is more effective than using a single drug. The choice of chemotherapy depends partly on whether cancer cells are detected in nearby lymph nodes.
Commonly used chemotherapy drugs include cyclophosphamide, doxorubicin, epirubicin, 5-fluorouracil, methotrexate, and paclitaxel (see Chemotherapy).
Side effects (such as vomiting, nausea, hair loss, and fatigue) vary depending on which chemotherapy is used. Chemotherapy can cause infertility and early menopause by destroying the eggs in the ovaries. Chemotherapy may also suppress the production of blood cells by the bone marrow and thus cause anemia or bleeding or increase the risk of infections. So drugs, such as filgrastim or pegfilgrastim, may by used to stimulate the bone marrow to produce blood cells.
HER2-directed therapy
Trastuzumab and pertuzumab are a type of monoclonal antibody called anti-HER2 medications. They are used with chemotherapy to treat metastatic breast cancer only when the cancer cells have too many HER2 receptors. These medications bind with HER2 receptors and thus help prevent cancer cells from multiplying. Sometimes both of these medications are used. Trastuzumab is usually taken for a year. Both medications can weaken the heart muscle. So doctors monitor heart function during treatment.
Treatment of Noninvasive Cancer (Stage 0)
(See also table Treating Breast Cancer Based on Type and Stage.)
For ductal carcinoma in situ, treatment usually consists of one the following:
A mastectomy
Removal of the tumor and a large amount of surrounding normal tissue (lumpectomy) with or without radiation therapy
Women with estrogen receptor–positive or progesterone receptor–positive ductal carcinoma in situ may also be given hormone blockers as part of their treatment.
Lobular carcinoma in situ (LCIS) is not cancer, but causes abnormal cells to form in milk glands (lobules) in the breast. People with LCIS have an increased risk of developing breast cancer. Treatment for LCIS includes the following:
Classic lobular carcinoma in situ: Surgical removal to check for cancer and, if no cancer is detected, close observation afterward and sometimes tamoxifen, raloxifene, or an aromatase inhibitor to reduce the risk of developing invasive cancer
Pleomorphic lobular carcinoma in situ: Surgery to remove the abnormal area and sometimes tamoxifen or raloxifene to reduce the risk of developing invasive cancer
Observation consists of a physical examination every 6 to 12 months for 5 years and once a year thereafter plus mammography once a year. Although invasive breast cancer may develop, the invasive cancers that develop are usually not fast growing and can usually be treated effectively. Furthermore, because invasive cancer is equally likely to develop in either breast, the only way to eliminate the risk of breast cancer for women with lobular carcinoma in situ is removal of both breasts (bilateral mastectomy). Some women, particularly those who are at high risk of developing invasive breast cancer, choose this option.
Women with lobular carcinoma in situ are often given tamoxifen, a hormone-blocking medication, for 5 years. It reduces but does not eliminate the risk of developing invasive cancer. Postmenopausal women may be given raloxifene or sometimes an aromatase inhibitor instead.
Treatment of Early-Stage Invasive Cancer (Stages I and II)
For breast cancers that are within the breast and may or may not have spread to nearby lymph nodes, treatment almost always includes surgery to remove as much of the tumor as possible. One of the following may be done:
Breast-conserving surgery (lumpectomy), followed by radiation therapy
Mastectomy with or without breast reconstruction
The initial surgery may include axillary lymph node dissection (removal of many lymph nodes from the armpit) or sentinel lymph node biopsy (removal of the lymph node nearest the breast or the first few nodes that are nearest the breast).
Breast-conserving surgery rather than mastectomy is used only when the tumor is not too large, because the entire tumor plus some of the surrounding normal tissue must be removed.
After surgery, women may be given chemotherapy, hormone blockers, anti-HER2 medications, or a combination, depending on analysis of the tumor.
There are several reasons that a woman may be treated with chemotherapy before surgery (called neoadjuvant chemotherapy). If the tumor is attached to the chest wall, chemotherapy helps make removing the tumor possible. Chemotherapy also helps shrink the size of a breast cancer that is large in relation to the rest of the breast. This increases the chances of being able to have breast-conserving surgery.
Neoadjuvant chemotherapy may also be considered for treatment of breast cancers that do not have receptors for estrogen, progesterone, and HER2 (called triple negative breast cancer) and cancers that have only HER2 receptors.
Treatment of Locally Advanced Cancer (Stage III)
For breast cancers that have spread to more lymph nodes, the following may be done:
Before surgery, medications, usually chemotherapy, to shrink the tumor
Breast-conserving surgery or mastectomy
After surgery, usually radiation therapy
After surgery, chemotherapy, hormone blockers, or both
Whether radiation therapy and/or chemotherapy or other medications are used after surgery depends on many factors, such as the following:
How large the tumor is
Whether menopause has occurred
Whether the tumor has receptors for hormones
How many lymph nodes contain cancer cells
Treatment of Cancer That Has Spread (Stage IV) or Recurs
Breast cancer that has spread beyond the lymph nodes can not be cured, but most women who have it live at least 2 years, and a few live 10 to 20 years. Treatment response depends on the tumor biology, but may relieve symptoms and improve quality of life. However, some treatments have troublesome side effects. Thus, deciding whether to be treated and, if so, which treatment to choose can be highly personal.
Choice of therapy depends on the following:
Whether the cancer has estrogen and progesterone receptors
How long the cancer had been in remission before it spread
How many organs and how many parts of the body the cancer has spread to (where the metastases are)
Whether the woman is postmenopausal or still menstruating
If the cancer is causing symptoms (pain or other discomfort), women are usually treated with chemotherapy or hormone blockers. Pain is usually treated with analgesics. Other medications may be given to relieve other symptoms. If curative therapy is not possible, treatments are given to reduce symptoms (called palliative therapy).
Hormone blockers (endocrine therapy) is preferred to chemotherapy when the cancer has the following characteristics:
The cancer is estrogen receptor–positive.
Cancer has not recurred for more than 2 years after diagnosis and initial treatment.
Cancer is not immediately life threatening.
Different endocrine therapies are used in different situations:
Tamoxifen:Tamoxifen is often the first choice of a hormone blocker for premenopausal women.
Aromatase inhibitors: For postmenopausal women with estrogen receptor–positive breast cancer, aromatase inhibitors (such as anastrozole, letrozole, and exemestane) may be more effective as a first treatment than tamoxifen.
Progestins: These medications, such as medroxyprogesterone or megestrol, may be used if aromatase inhibitors and tamoxifen are no longer effective.
Fulvestrant: This medication may be used when tamoxifen is no longer effective. It destroys the estrogen receptors in cancer cells.
Alternatively, for premenopausal women, surgery to remove the ovaries or medications to inhibit their activity (such as buserelin, goserelin, or leuprolide) may be used to stop estrogen production. These therapies may be used with tamoxifen or aromatase inhibitors.
Trastuzumab can be used to treat cancers with HER2 receptors that have spread throughout the body. Trastuzumab can be used alone or with chemotherapy (such as paclitaxel), with hormone blockers, or with pertuzumab (another anti-HER2 medication).
Tyrosine kinase inhibitors (such as lapatinib and neratinib), another type of anti-HER2 medication, block the activity of HER2.
In some situations, radiation therapy may be used instead of or before medications. For example, if only one area of cancer is detected and that area is in a bone, radiation to that bone might be the only treatment used. Radiation therapy is usually the most effective treatment for cancer that has spread to bone, sometimes keeping it in check for years. It is also often the most effective treatment for cancer that has spread to the brain.
Surgery may be done to remove single tumors in other parts of the body (such as the brain) because such surgery can relieve symptoms. Mastectomy (removing the breast) may be done to help relieve symptoms. But it is unclear whether removing the breast helps prolong life when cancer has spread to other parts of the body and has been treated and controlled.
Bisphosphonates (used to treat osteoporosis), such as pamidronate or zoledronate, reduce bone pain and bone loss and may prevent or delay bone problems that can result when cancer spreads to bone.
Treating Breast Cancer Based on Type and Stage
Type | Possible Treatments |
|---|---|
Ductal carcinoma in situ (cancer confined to the milk ducts of the breast) | Lumpectomy (breast-conserving surgery to remove tumor and some surrounding tissue) or mastectomy Sometimes hormone blockers (medications, such as tamoxifen or aromatase inhibitors, that affect hormones) |
Lobular carcinoma in situ, classic (abnormal cells confined to the milk-producing glands of the breast) | Sometimes surgery to check for cancer If no cancer is detected, observation plus regular examinations and mammograms Tamoxifen or, for some postmenopausal women, raloxifene or an aromatase inhibitor (such as anastrozole, exemestane, or letrozole) to reduce the risk of invasive cancer Rarely, bilateral mastectomy (removal of both breasts) to prevent invasive cancers |
Lobular carcinoma in situ, pleomorphic (which, unlike the classic type, leads to invasive cancer) | Surgery to remove the abnormal area and some of the tissue around it Sometimes tamoxifen or raloxifene to try to prevent cancer from developing |
Stages I and II (early-stage) cancer | Lumpectomy, followed by radiation therapy Mastectomy with or without breast reconstruction After surgery, chemotherapy, hormone blockers, anti-HER2 medications (such as trastuzumab), or a combination Sometimes, neoadjuvant therapy (chemotherapy before surgery) to reduce tumor size and optimize the chances for breast-conserving surgery |
Stage III (locally advanced) cancer (including inflammatory breast cancer) | Often, chemotherapy or sometimes hormone blockers before surgery to reduce tumor size Lumpectomy or mastectomy, if the tumor is small enough to be completely removed Usually, radiation therapy after surgery Sometimes chemotherapy, hormone blockers, or both after surgery |
Stage IV (metastatic) cancer or cancer that recurs | For estrogen receptor–positive tumors, hormone blockers or removal or suppression of ovaries Chemotherapy For HER2 receptor–positive tumors, trastuzumab, sometimes with pertuzumab Radiation therapy for the following:
For metastases to bone, bisphosphonates (such as zoledronate or pamidronate) given intravenously to reduce bone pain and bone loss |
Treatment of Specific Types of Breast Cancer
For inflammatory breast cancer, treatment usually consists of both chemotherapy and radiation therapy. Mastectomy is usually done.
For Paget disease of the breast, treatment is usually similar to that of other types of breast cancer. It often involves simple mastectomy or breast-conserving surgery plus removal of the lymph nodes. Breast-conserving surgery is usually followed by radiation therapy. Less commonly, only the nipple with some surrounding normal tissue is removed. If another breast cancer is also present, treatment is based on that type of breast cancer.
For phyllodes tumors, treatment usually consists of removing the tumor and a large amount of surrounding normal tissue (at least 1 centimeter (0.4 inch) around the tumor)—called a wide margin. If the tumor is large in relation to the breast, a simple mastectomy may be done to remove the tumor plus wide margins. Whether phyllodes tumors recur depends on how wide the tumor-free margins are and whether the phyllodes tumor is noncancerous or cancerous. Cancerous phyllodes tumors can metastasize to distant sites, such as the lungs, bone, or brain. Recommendations for treatment of metastatic phyllodes tumors are evolving, but radiation therapy and chemotherapy may be useful.
Preservation of Fertility
Women should not become pregnant while being treated for breast cancer.
If women wish to have children (preserve fertility) after being treated, they are referred to a reproductive endocrinologist before treatment is started. These women can then find out about the effect of different chemotherapy drugs on fertility and about procedures that may enable them to have children after treatment.
Options to preserve fertility include assisted reproductive techniques with ovarian stimulation and freezing eggs or embryos.
Choice of the procedure to be used to preserve fertility depends on the following:
Type of breast cancer
Type of breast cancer treatment that is planned
The woman's preferences
Assisted reproductive techniques involve use of hormonal medications. Doctors discuss the risks and benefits of having these treatments with women who have had an estrogen or progesterone receptor–positive cancer.
Follow-up Care
After the first phases of treatment are completed, follow-up physical examinations, including examination of the breasts, chest, neck, and armpits, are usually done every year. Regular mammograms and breast self-examinations are also important. Women should promptly report certain symptoms to their doctor:
Any lumps or other changes in their breasts
Changes in nipples or a discharge
Pain—for example in the arm or spine
Swelling in the armpit
Loss of appetite or weight
Chest pain
Chronic dry cough
Bleeding from the vagina (if not associated with menstrual periods)
Severe headaches
Blurred vision
Dizziness or balance problems
Numbness or weakness
Any symptoms that seem unusual or that persist
Diagnostic procedures, such as chest x-rays, blood tests, bone scans, and computed tomography (CT), are not needed unless symptoms suggest the cancer has recurred.
The effects of treatment for breast cancer cause many changes in a woman’s life. Support from family members and friends can help, as can support groups. Counseling may be helpful.
Prognosis for Breast Cancer
Generally, a woman's prognosis depends on
How large the cancer is
What type of cancer it is
Whether it has spread to the lymph nodes or other organs
(See also the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) Program.)
The number and location of lymph nodes that contain cancer cells is one of the main factors that determine whether the cancer can be cured and, if not, how long women will live.
The 5-year survival rate for breast cancer (the percentage of women who are alive 5 years after diagnosis) is
99% if the cancer remains at its original site (localized)
86% if the cancer has spread to nearby lymph nodes but no further (regional)
29% if the cancer has spread to distant sites (metastasized)
58% if a full evaluation has not been done and the cancer has not been staged
Women with breast cancer tend to have a worse prognosis if they have any of the following:
Diagnosis of breast cancer during their 20s and 30s
Larger tumors
Cancer that has rapidly dividing cells, such as tumors that do not have well-defined borders or cancer that is dispersed throughout the breast
Tumors that do not have estrogen or progesterone receptors
Tumors that have too many HER2 receptors
A BRCA1 gene mutation
In the United States, women who are non-Hispanic Black have higher rates of death from breast cancer than women who are non-Hispanic White.
Having the BRCA2 gene mutation probably does not make the current cancer result in a worse outcome. However, having either BRCA gene mutation increases the risk of developing a second breast cancer.
End-of-Life Issues in Breast Cancer
For women with metastatic breast cancer, quality of life may deteriorate, and the chances that further treatment will prolong life may be small. Staying comfortable may eventually become more important than trying to prolong life.
Cancer pain can be adequately controlled with appropriate medications. So if women are having pain, they should ask their doctor for treatment to relieve it. Treatments can also relieve other troublesome symptoms, such as constipation, difficulty breathing, and nausea.
Psychological and spiritual counseling may also help.
Women with metastatic breast cancer should prepare advance directives indicating the type of care they desire in case they are no longer able to make such decisions. Also, making or updating a will is important.
Drug Information for the Topic





