

Preeclampsia is new onset or worsening of existing hypertension with proteinuria after 20 weeks gestation. Eclampsia is unexplained generalized seizures in patients with preeclampsia. Diagnosis is by measuring blood pressure and urine protein and by tests to evaluate for end-organ damage (eg, pulmonary edema, impaired liver or kidney function). Treatment is usually with IV magnesium sulfate and delivery at term, or earlier for maternal or fetal complications.
Preeclampsia occurs in 4.6% and eclampsia in 1.4% of deliveries worldwide (1). Preeclampsia and eclampsia develop after 20 weeks gestation, although most cases occur after 34 weeks (2). Some cases develop postpartum, most often within the first 4 days but sometimes up to 6 weeks postpartum.
Untreated preeclampsia is present for a variable time, then can suddenly progress to eclampsia. Untreated eclampsia is usually fatal.

General references
1. Abalos E, Cuesta C, Grosso AL, Chou D, Say L: Global and regional estimates of preeclampsia and eclampsia: a systematic review. Eur J Obstet Gynecol Reprod Biol 170(1):1-7, 2013. doi:10.1016/j.ejogrb.2013.05.005
2. Lisonkova S, Sabr Y, Mayer C, Young C, Skoll A, Joseph KS. Maternal morbidity associated with early-onset and late-onset preeclampsia. Obstet Gynecol 124(4):771-781, 2014. doi:10.1097/AOG.0000000000000472
Etiology of Preeclampsia and Eclampsia
Etiology of preeclampsia is unknown.
However, high-risk and moderate-risk factors have been identified (1,2).
High-risk factors include
Previous pregnancy with preeclampsia
Multiple gestation
Kidney disorders
Autoimmune disorders
Type 1 or type 2 diabetes mellitus
Chronic hypertension
Moderate-risk factors include
First pregnancy
Maternal age ≥ 35 years
Prepregnancy body mass index > 30
Family history of preeclampsia (in a first-degree relative)
Non-Hispanic Black and American Indian or Alaskan Native women (3)
Lower income
Etiology references
1. Henderson JT, Whitlock EP, O'Conner E, et al: Table 8: Preeclampsia Risk Factors Based on Patient Medical History in Low-dose aspirin for the prevention of morbidity and mortality from preeclampsia: A systematic evidence review for the U.S. Preventive Services Task ForceLow-dose aspirin for the prevention of morbidity and mortality from preeclampsia: A systematic evidence review for the U.S. Preventive Services Task Force. Rockville (MD): Agency for Healthcare Research and Quality (US), 2014
2. American College of Obstetrics and Gynecology (ACOG): ACOG Practice Bulletin, Number 222: Gestational Hypertension and PreeclampsiaObstet Gynecol 135(6):e237-e260, 2020. doi:10.1097/AOG.0000000000003891
3. Johnson JD, Louis JM: Does race or ethnicity play a role in the origin, pathophysiology, and outcomes of preeclampsia? An expert review of the literature. Am J Obstet Gynecol 226(2S):S876-S885, 2022. doi:10.1016/j.ajog.2020.07.038
Pathophysiology of Preeclampsia and Eclampsia
Pathophysiology of preeclampsia and eclampsia is poorly understood. Factors may include poorly developed uterine placental spiral arterioles (which decrease uteroplacental blood flow during late pregnancy), a genetic abnormality, immunologic abnormalities, and placental ischemia or infarction. Lipid peroxidation of cell membranes induced by free radicals may contribute to preeclampsia.
The coagulation system is activated, possibly secondary to endothelial cell dysfunction, leading to platelet activation.

Complications
Preeclampsia and eclampsia are major causes of maternal mortality in the Unites States (1) and worldwide (2). Women who have preeclampsia are at risk of placental abruption in the current pregnancy, possibly because both disorders are related to uteroplacental insufficiency. Pregnant women may develop pulmonary edema, acute kidney injury, liver rupture, or cerebrovascular hemorrhage, with or without seizures.
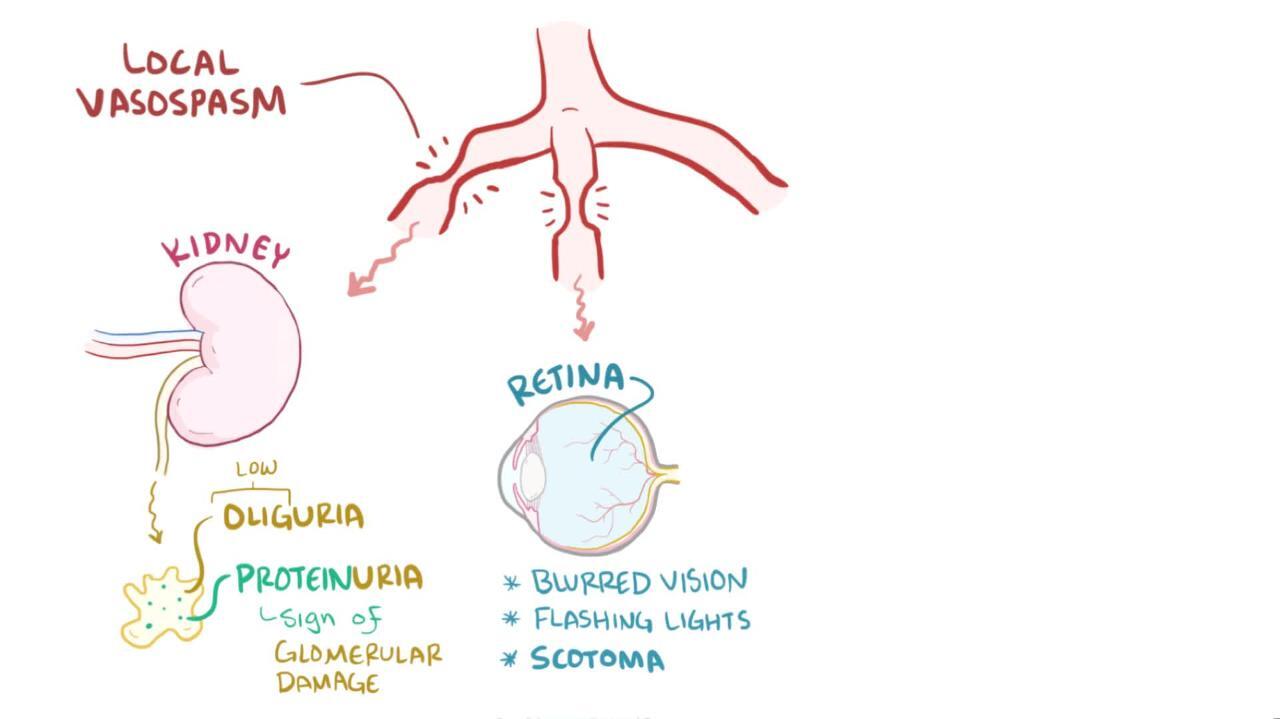
Fetal complications may includegrowth restriction, oligohydramnios, or stillbirth (3). Diffuse or multifocal vasospasm can result in maternal ischemia, eventually damaging multiple organs, particularly the brain, kidneys, and liver. Factors that may contribute to vasospasm include decreased prostacyclin (an endothelium-derived vasodilator), increased endothelin (an endothelium-derived vasoconstrictor), and increased soluble Flt-1 (a circulating receptor for vascular endothelial growth factor).
The HELLP syndrome (hemolysis, elevated liver function tests, and low platelet count) develops in 0.2 to 0.6% of pregnancies (4). Most pregnant women with HELLP syndrome have hypertension and proteinuria, but some have neither.
Pathophysiology references
1. Ford ND, Cox S, Ko JY, et al: Hypertensive Disorders in Pregnancy and Mortality at Delivery Hospitalization - United States, 2017-2019. MMWR Morb Mortal Wkly Rep 71(17):585-591, 2022. Published 2022 Apr 29. doi:10.15585/mmwr.mm7117a1
2. Say L, Chou D, Gemmill A, et al: Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health 2(6):e323-e333, 2014. doi:10.1016/S2214-109X(14)70227-X
3. Harmon QE, Huang L, Umbach DM, et al: Risk of fetal death with preeclampsia. Obstet Gynecol 125(3):628-635, 2015. doi:10.1097/AOG.0000000000000696
4. Sarkar M, Brady CW, Fleckenstein J, et al: Reproductive Health and Liver Disease: Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 73(1):318-365, 2021. doi:10.1002/hep.31559
Symptoms and Signs of Preeclampsia and Eclampsia
Preeclampsia may be asymptomatic or may cause edema or sudden excessive weight gain (> 5 lb/week). Nondependent edema, such as facial or hand swelling (the patient’s ring may no longer fit her finger), is more specific than dependent edema.
Eclampsia manifests as generalized (tonic-clonic) seizures.
Pearls & Pitfalls
|
Preeclampsia with severe features may cause organ damage; these features may include
Severe headache
Visual disturbances
Confusion
Hyperreflexia
Epigastric or right upper quadrant abdominal pain (reflecting hepatic ischemia or capsular distention)
Nausea and/or vomiting
Dyspnea (reflecting pulmonary edema, acute respiratory distress syndrome [ARDS], or cardiac dysfunction secondary to increased afterload)
Oliguria (reflecting decreased plasma volume or ischemic acute tubular necrosis)
Stroke (rarely)
Diagnosis of Preeclampsia and Eclampsia
Preeclampsia: New onset after 20 weeks gestation of hypertension plus new unexplained proteinuria (> 300 mg/24 hours or a urine protein/creatinine ratio of ≥ 0.3) and/or signs of end-organ damage (1)
Blood pressure (BP) criteria for preeclampsia are one of the following:
Systolic BP ≥ 140 mm Hg and/or diastolic BP ≥ 90 mm Hg (at least 2 measurements taken at least 4 hours apart)
Systolic BP ≥ 160 mm Hg and/or diastolic BP ≥ 110 mm Hg (at least 2 measurements)
Proteinuria is defined as > 300 mg/24 hours. Alternatively, proteinuria is diagnosed based on a protein/creatinine ratio ≥ 0.3 or a dipstick reading of 2+; the dipstick test is used only if other quantitative methods are not available. Absence of proteinuria on less accurate tests (eg, urine dipstick testing, routine urinalysis) does not rule out preeclampsia.
In the absence of proteinuria, preeclampsia may be diagnosed if pregnant women meet diagnostic criteria for new-onset hypertension and also have new-onset signs of end-organ damage.
Preeclampsia with severe features is diagnosed in patients with new onset of persistent severe hypertension and/or signs or symptoms of end-organ damage. The blood pressure criterion is systolic BP ≥ 160 mm Hg and/or diastolic BP ≥ 110 mm Hg on at least 2 measurements taken at least 4 hours apart.
Signs or symptoms of end-organ damage may include one or more of the following:
Thrombocytopenia (platelets < 100 x 109 L)
Impaired liver function (aminotransferases > 2 times normal) not accounted for by alternative diagnoses
Severe persistent right upper quadrant or epigastric pain unresponsive to medications
Renal insufficiency (serum creatinine > 1.1 mg/dL or doubling of serum creatinine in the absence of renal disease)
Pulmonary edema
New-onset headache unresponsive to medication and not accounted for by alternative diagnoses
Visual disturbances
Additional diagnostic categories of preeclampsia are as follows:
HELLP syndrome is classified as a severe form of preeclampsia and is diagnosed when all of the following are present: lactate dehydrogenase (LDH) ≥ 600 IU/L; aminotransferases > 2 times normal; and platelets < 100 × 109 L. HELLP syndrome may have an atypical clinical presentation, with the absence of hypertension or proteinuria in up to 15% of patients (2).
Preeclampsia superimposed on chronic hypertension is diagnosed when a patient known to have chronic hypertension develops one of the following after 20 weeks: new unexplained proteinuria or worsening proteinuria; BP elevations above baseline; or signs of end-organ damage. Women with chronic hypertension are at high risk of preeclampsia and should be monitored closely. An elevated uric acid level suggests a diagnosis of superimposed preeclampsia rather than solely chronic hypertension (3).
Patients with any type of preeclampsia are at risk of developing eclampsia. Sometimes eclampsia occurs before a diagnosis of preeclampsia is made.
Eclampsia is new onset of tonic-clonic, focal, or multifocal seizures with no other known causes (eg, epilepsy, cerebral arterial ischemia or infarction, intracranial hemorrhage, or drug use).
Evaluation
If preeclampsia is suspected, the evaluation includes taking a medical history regarding risk factors, current symptoms, and any history or symptoms that suggest another disorder. Physical examination includes measurement of BP and assessment for facial or upper or lower extremity edema, pulmonary edema, upper right quadrant abdominal tenderness, and hyperreflexia. Pelvic examination is performed if vaginal bleeding or regular contractions are present or if induction of labor is planned. Laboratory tests include complete blood count (CBC), platelet count, uric acid, liver tests, blood urea nitrogen (BUN), creatinine, and, if creatinine is abnormal, creatinine clearance. Urine protein is checked with a dipstick or urinalysis; a 24-hour urine collection is begun, if urgent delivery is not indicated.If preeclampsia is suspected, the evaluation includes taking a medical history regarding risk factors, current symptoms, and any history or symptoms that suggest another disorder. Physical examination includes measurement of BP and assessment for facial or upper or lower extremity edema, pulmonary edema, upper right quadrant abdominal tenderness, and hyperreflexia. Pelvic examination is performed if vaginal bleeding or regular contractions are present or if induction of labor is planned. Laboratory tests include complete blood count (CBC), platelet count, uric acid, liver tests, blood urea nitrogen (BUN), creatinine, and, if creatinine is abnormal, creatinine clearance. Urine protein is checked with a dipstick or urinalysis; a 24-hour urine collection is begun, if urgent delivery is not indicated.
The fetus is assessed using a nonstress test or biophysical profile (including assessment of amniotic fluid volume) and measurements to estimate fetal weight.
Other hypertensive disorders in pregnancy
Preeclampsia must be differentiated from other hypertensive disorders in pregnancy (1):
Gestational hypertension is new-onset hypertension at > 20 weeks gestation without proteinuria or other signs of end-organ damage; it resolves by 12 weeks (usually by 6 weeks) postpartum.
Chronic hypertension is identified if hypertension precedes pregnancy, is present at < 20 weeks gestation, or persists for > 6 weeks (usually > 12 weeks) postpartum (even if hypertension is first documented at > 20 weeks gestation). Chronic hypertension may be masked during early pregnancy by the physiologic decrease in BP.
Diagnosis references
1. American College of Obstetrics and Gynecology (ACOG): ACOG Practice Bulletin, Number 222: Gestational Hypertension and Preeclampsia, Obstet Gynecol 135(6):e237-e260, 2020. doi:10.1097/AOG.0000000000003891
2. Martin JNJr, Rinehart BK, May WL, et al: The spectrum of severe preeclampsia: comparative analysis by HELLP (hemolysis, elevated liver enzyme levels, and low platelet count) syndrome classification. Am J Obstet Gynecol 180: 1373– 84, 1999. doi:10.1016/s0002-9378(99)70022-0
3. Lim KH, Friedman SA, Ecker JL, Kao L, Kilpatrick SJ: The clinical utility of serum uric acid measurements in hypertensive diseases of pregnancy. Am J Obstet Gynecol 178(5):1067-1071, 1998. doi:10.1016/s0002-9378(98)70549-6
Treatment of Preeclampsia and Eclampsia
Usually hospitalization
Delivery, depending on factors such as gestational age, fetal status, and severity of preeclampsia
Magnesium sulfate to prevent or treat new seizures or to prevent seizures from recurring
Sometimes antihypertensive treatment, if patient meets criteria for severe hypertension
General approach
Definitive treatment for preeclampsia is delivery. However, risk of preterm delivery is balanced against gestational age, fetal growth restriction, fetal distress, and severity of preeclampsia.
Usually, immediate delivery after maternal stabilization (eg, controlling seizures, beginning to control blood pressure [BP]) is indicated for the following:
Pregnancy of ≥ 37 weeks
Preeclampsia with severe features if pregnancy is ≥ 34 weeks
Deteriorating renal, pulmonary, cardiac, or hepatic function (including HELLP syndrome)
Nonreassuring results of fetal monitoring or testing
Eclampsia
Patients with preeclampsia with severe features or eclampsia are often admitted to a maternal special care unit or an intensive care unit (ICU).
Pregnant patients at 34 to < 37 weeks of gestation who do not require immediate delivery are hospitalized for evaluation, at least initially. If maternal and fetal status are reassuring, outpatient treatment is possible; it includes modified activity (modified rest), BP measurements, laboratory monitoring, fetal nonstress testing, and physician visits at least once a week. As long as no criteria for preeclampsia with severe features develop, delivery can occur (eg, by induction) at 37 weeks.
In pregnancies at < 34 weeks, if delivery can be safely delayed, corticosteroids are given for 48 hours to accelerate fetal lung maturity. Some stable patients can be given corticosteroids after 34 weeks and before 36 weeks (late preterm period) if they have not been given corticosteroids earlier in the pregnancy.
Monitoring
All hospitalized patients with preeclampsia are evaluated frequently for evidence of preeclampsia with severe features, seizures, or vaginal bleeding; BP, reflexes, and fetal status (with nonstress testing or a biophysical profile) are also checked. Platelet count, serum creatinine, and serum liver enzymes are measured frequently until stable, then at least once a week.
Outpatients are usually followed by an obstetrician or a maternal-fetal medicine specialist and evaluated at least once a week with the same laboratory testing as inpatients. Outpatient nonstress testing typically takes place twice a week with weekly amniotic fluid index evaluation usually starting at 32 weeks. In some select cases, this can be offered at 28 weeks.
Magnesium sulfate
It is controversial whether patients who have preeclampsia without severe features always require magnesium sulfate before delivery.
If patients have preeclampsia with severe features, magnesium sulfate is given to prevent seizures. As soon as eclampsia is diagnosed, magnesium sulfate must be given to prevent seizures from recurring.
Magnesium sulfate 4 g IV over 20 minutes is given, followed by a constant IV infusion of 2 g/hour. Dose is adjusted based on whether renal insufficiency is present. Magnesium sulfate is given for 12 to 24 hours postpartum.
Patients with very high magnesium levels and significant symptoms (eg, with magnesium levels > 10 mEq/L or a sudden decrease in reflex reactivity), cardiac dysfunction (eg, with dyspnea or chest pain), or hypoventilation after treatment with magnesium sulfate can be treated with calcium gluconate 1 g IV. 10 mEq/L or a sudden decrease in reflex reactivity), cardiac dysfunction (eg, with dyspnea or chest pain), or hypoventilation after treatment with magnesium sulfate can be treated with calcium gluconate 1 g IV.
IV magnesium sulfate may cause lethargy, hypotonia, and transient respiratory depression in neonates. However, serious neonatal complications are uncommon.
Supportive treatments
If oral intake is prohibited, hospitalized patients are given IV Ringer lactate or 0.9% normal saline solution, beginning at about 125 mL/hour (to maintain hemodynamic status). Persistent oliguria is treated with a carefully monitored fluid challenge. Diuretics are usually not used. Monitoring with a pulmonary artery catheter is rarely necessary and, if needed, is done in consultation with a critical care specialist and in an intensive care unit (ICU). Anuric patients with normovolemia may require renal vasodilators or dialysis.
If seizures occur despite magnesium therapy, diazepam or lorazepam can be given IV to stop seizures, and IV hydralazine or labetalol is given in a dose titrated to lower systolic BP to 140 to 155 mm Hg and diastolic BP to 90 to 105 mm Hg.If seizures occur despite magnesium therapy, diazepam or lorazepam can be given IV to stop seizures, and IV hydralazine or labetalol is given in a dose titrated to lower systolic BP to 140 to 155 mm Hg and diastolic BP to 90 to 105 mm Hg.
Delivery method
The most efficient method of delivery should be used. If the cervix is favorable and rapid vaginal delivery seems feasible, a dilute IV infusion of oxytocin is given to induce or accelerate labor; if labor is active, the membranes are ruptured. If the cervix is unfavorable and prompt vaginal delivery is unlikely, cesarean delivery may be considered. Preeclampsia and eclampsia, if not resolved before delivery, usually resolve rapidly afterward, within 6 to 12 hours.The most efficient method of delivery should be used. If the cervix is favorable and rapid vaginal delivery seems feasible, a dilute IV infusion of oxytocin is given to induce or accelerate labor; if labor is active, the membranes are ruptured. If the cervix is unfavorable and prompt vaginal delivery is unlikely, cesarean delivery may be considered. Preeclampsia and eclampsia, if not resolved before delivery, usually resolve rapidly afterward, within 6 to 12 hours.
Follow-up
BP should be monitored closely until it normalizes after delivery. Patients should then be evaluated at least every 1 to 2 weeks postpartum with periodic BP measurement. If BP remains high after 6 weeks postpartum, patients may have chronic hypertension and should be referred to their primary care physician for management.
Postpartum preeclampsia
Preeclampsia can develop after delivery. Signs and symptoms are similar to preeclampsia during pregnancy, and women should be counseled to call their providers if they experience these symptoms postpartum. The work-up is similar to the work-up done during pregnancy, including blood pressure monitoring and laboratory evaluation. In cases that meet criteria for severe preeclampsia, patients are hospitalized and treated with IV magnesium sulfate for 24 hours to prevent seizures.
Treatment reference
1. American College of Obstetrics and Gynecology (ACOG): ACOG Practice Bulletin, Number 222: Gestational Hypertension and Preeclampsia, Obstet Gynecol 135(6):e237-e260, 2020. doi:10.1097/AOG.0000000000003891
Prevention
Meta-analyses of randomized trials have shown that low-dose aspirin therapy in women with certain risk factors reduces the rate of severe preeclampsia and fetal growth restriction (Meta-analyses of randomized trials have shown that low-dose aspirin therapy in women with certain risk factors reduces the rate of severe preeclampsia and fetal growth restriction (1, 2).
Low-dose aspirin (81 mg/day) is recommended for patients with high-risk factors for preeclampsia (previous pregnancy with preeclampsia, multiple gestation, renal disorders, autoimmune disorders, type 1 or type 2 diabetes mellitus, chronic hypertension) (Low-dose aspirin (81 mg/day) is recommended for patients with high-risk factors for preeclampsia (previous pregnancy with preeclampsia, multiple gestation, renal disorders, autoimmune disorders, type 1 or type 2 diabetes mellitus, chronic hypertension) (3). It is also recommended for those with > 1 moderate-risk factor (first pregnancy, maternal age ≥ 35, prepregnancy body mass index > 30, first-degree relative with a history of preeclampsia, Black women [as a proxy for underlying racism], lower income, personal history factors such as low-birth-weight or small-for-gestational-age infant, previous adverse pregnancy outcome, or a> 10-year pregnancy interval [4]). Some evidence suggests that increasing the aspirin dose to 162 mg once a day is more effective in preventing preeclampsia (]). Some evidence suggests that increasing the aspirin dose to 162 mg once a day is more effective in preventing preeclampsia (5).
Aspirin prophylaxis should be started at 12 to 28 weeks of gestation (ideally before 16 weeks) and continued until delivery.
Prevention references
1. Roberge S, Nicolaides K, Demers S et al: The role of aspirin dose on the prevention of preeclampsia and fetal growth restriction: Systematic review and meta-analysis. : The role of aspirin dose on the prevention of preeclampsia and fetal growth restriction: Systematic review and meta-analysis.Am J Obstet Gynecol 216 (2):110–120.e6, 2017. doi: 10.1016/j.ajog.2016.09.076
2. Meher S, Duley L, Hunter K, Askie L: Antiplatelet therapy before or after 16 weeks gestation for preventing preeclampsia: An individual participant data meta-analysis. Am J Obstet Gynecol 216 (2):121–128.e2, 2017. doi: 10.1016/j.ajog.2016.10.016
3. American College of Obstetrics and Gynecology (ACOG): ACOG Committee Opinion No. 743 Summary: Low-Dose Aspirin Use During Pregnancy. : ACOG Committee Opinion No. 743 Summary: Low-Dose Aspirin Use During Pregnancy.Obstet Gynecol 132(1):254-256, 2018. Reaffirmed 2023. doi:10.1097/AOG.0000000000002709
4. American College of Obstetrics and Gynecology (ACOG): ACOG Practice Bulletin, Number 222: Gestational Hypertension and Preeclampsia. Obstet Gynecol 135(6):e237-e260, 2020. doi:10.1097/AOG.0000000000003891
5. Ayyash M, Goyert G, Garcia R, et al: Efficacy and Safety of Aspirin 162 mg for Preeclampsia Prophylaxis in High-Risk Patients. : Efficacy and Safety of Aspirin 162 mg for Preeclampsia Prophylaxis in High-Risk Patients.Am J Perinatol. Published online July 29, 2023. doi:10.1055/s-0043-1771260
Key Points
Preeclampsia is new-onset hypertension with proteinuria after 20 weeks of gestation, and eclampsia is unexplained generalized seizures in patients with preeclampsia; preeclampsia sometimes develops postpartum.
Preeclampsia is differentiated from chronic hypertension and gestational hypertension by the presence of new-onset proteinuria and/or end-organ damage.
Preeclampsia is severe if it causes severe persistent hypertension and/or significant organ dysfunction (eg, renal insufficiency, impaired liver function, pulmonary edema, visual symptoms), even in the absence of proteinuria.
HELLP syndrome (hemolysis, elevated liver enzymes, low platelets) is a related disorder that occurs in 10 to 20% of women who have preeclampsia with severe features or eclampsia.
Evaluate and closely monitor the mother and fetus, usually in a hospital maternal special care unit, but sometimes outpatient monitoring is possible for mild cases at < 37 weeks of gestation.
Delivery is indicated when the pregnancy is ≥ 37 weeks, but if preeclampsia is diagnosed at < 34 weeks, delay delivery if possible (to allow time to improve fetal lung maturity); if preeclampsia with severe features, HELLP syndrome, or eclampsia is diagnosed, deliver immediately.
Treat eclampsia immediately with magnesium sulfate to prevent seizures from recurring; consider magnesium sulfate for seizure prophylaxis in women who have preeclampsia with severe features, but usually not in those with mild preeclampsia.
If magnesium sulfate is given for seizure prophylaxis, continue for 12 to 24 hours after delivery.
Give women with certain risk factors low-dose aspirin starting at 12 to 28 weeks to reduce risk of preeclampsia, ideally before 16 weeks. Give women with certain risk factors low-dose aspirin starting at 12 to 28 weeks to reduce risk of preeclampsia, ideally before 16 weeks.
Drug Information for the Topic





