


Trichinosis is infection with Trichinella spiralis or related Trichinella
(See also Approach to Parasitic Infections.)
Trichinosis occurs worldwide. In addition to the classic agent Trichinella spiralis, trichinosis can be caused by T. pseudospiralis, T. nativa, T. nelsoni, and T. britovi in different geographic locations. An estimated 10,000 cases of trichinosis occur worldwide each year. Fewer than 20 cases are reported each year in the United States.
Pathophysiology of Trichinosis
The Trichinella life cycle is maintained by animals that are fed (eg, pigs, horses) or eat (eg, bears, foxes, boars) other animals whose striated muscles contain encysted infective larvae (eg, rodents). Humans become infected by eating raw, undercooked, or under-processed meat from infected animals, most commonly pigs, wild boar, or bear. Larvae excyst in the small bowel, penetrate the mucosa, and become adults in 6 to 8 days. Females are about 2.2 mm long, and males are about 1.2 mm long.
Mature females release living larvae for 4 to 6 weeks and then die or are expelled. Newborn larvae migrate through the bloodstream and lymphatics but ultimately survive only within striated skeletal muscle cells. Larvae fully encyst in 1 to 2 months and remain viable for several years as intracellular parasites. Dead larvae eventually are resorbed or calcify. The cycle continues only if encysted larvae are ingested by another carnivore.

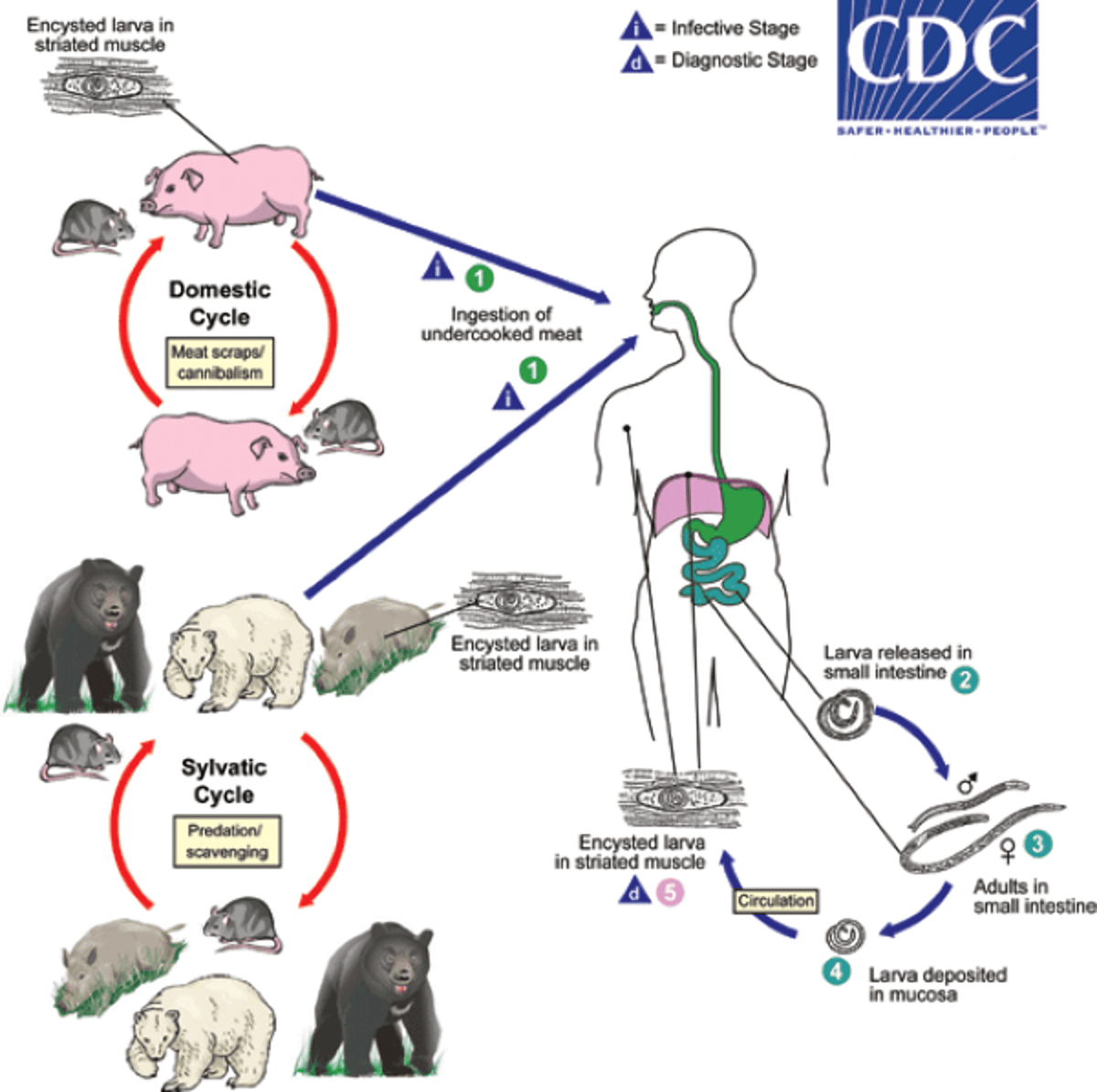
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Symptoms and Signs of Trichinosis
Many Trichinella infections are asymptomatic or mild.
During the 1st week, nausea, abdominal cramps, and diarrhea may occur.
One to 2 weeks after infection, systemic symptoms and signs begin: facial or periorbital edema, myalgia, persistent fever, headache, and subconjunctival hemorrhages and petechiae. Eye pain and photophobia often precede myalgia.
Symptoms due to muscle invasion may mimic symptoms of polymyositis. The muscles of respiration, speech, mastication, and swallowing may be painful. Severe dyspnea may occur in heavy infections.
Fever is generally remittent, rising to 39° C or higher, remaining elevated for several days, and then falling gradually. Eosinophilia usually begins when newborn larvae invade tissues, peaks 2 to 4 weeks after infection, and gradually declines as the larvae encyst.
In heavy infections, the inflammation may cause complications: cardiac (myocarditis, heart failure, arrhythmia), neurologic (encephalitis, meningitis, visual or auditory disorders, seizures), or pulmonary (pneumonitis, pleurisy). Death may result from myocarditis or encephalitis.
Symptoms and signs gradually resolve, and most disappear by about the 3rd month, when the larvae have become fully encysted in muscle cells and eliminated from other organs and tissues. Vague muscular pains and fatigue may persist for many months.
Recurrent infections with T. nativa in northern latitudes can cause chronic diarrhea.
Diagnosis of Trichinosis
Enzyme immunoassay
Rarely muscle biopsy
No specific tests to diagnose the intestinal stage of Trichinella are available. After the 2nd week of infection, a muscle biopsy may detect larvae and cysts but is seldom necessary. Diffuse inflammation in muscle tissue indicates recent infection.
A number of serologic tests have been used, but enzyme immunoassay (EIA) using T. spiralis excretory-secretory (ES) antigen seems to be the quickest way to detect the infection and is used in the United States. Antibodies are often not detectable for the first 2 to 8 weeks of infection, so tests should be repeated at weekly intervals if results are initially negative. Because antibodies may persist for years, serologic tests are of most value if they are initially negative and then positive. Serologic tests and muscle biopsy are complementary tests: Either one can be negative in a given patient with trichinosis. Skin testing with larval antigens is unreliable.
Muscle enzymes (creatine kinase and lactic dehydrogenase [LDH]) are elevated in 50% of patients and correlate with abnormal electromyograms.
Eosinophilia is common but has numerous infectious and noninfectious causes (see table Important Disorders and Treatments Associated With Eosinophilia).
Trichinosis must be differentiated from
Acute rheumatic fever, acute arthritis, angioedema, and myositis
Febrile illnesses such as tuberculosis, typhoid fever, sepsis, and brucellosis (undulant fever)
Neurologic manifestations of meningitis, encephalitis, and poliomyelitis
Eosinophilia due to neoplasms, eosinophilic leukemia, polyarteritis nodosa, or disease caused by other migrating nematodes
Treatment of Trichinosis
Symptomatic treatment
Anthelmintics eliminate adult Trichinella worms from the gastrointestinal tract, but once larvae encyst in skeletal muscle, treatment may not eradicate them or any associated symptoms.
Prevention of Trichinosis
Trichinosis is prevented by cooking pork or meat from wild animals until brown (> 71° C [> 160° F] throughout). Larvae can be killed in pork < 6 inches thick by freezing the pork at -15° C (-5° F) for 20 days. Freezing is not recommended for meat from wild animals because they may be infected with Trichinella species that are resistant to low temperatures.
Smoking, microwave cooking, or salting meat does not reliably kill larvae.
Meat grinders and other items used to prepare raw meat should be thoroughly cleaned. Handwashing with soap and water is also important.
Domestic swine should not be fed uncooked meat.
Key Points
Humans become infected with Trichinella by eating raw, undercooked, or under-processed meat from infected animals—most commonly pigs, wild boar, or bear.
Larvae excyst in the small bowel, penetrate the mucosa, and become adults that release living larvae; the larvae migrate through the bloodstream and lymphatics and encyst within striated skeletal muscle cells.
Symptoms begin with gastrointestinal irritation followed by periorbital edema, muscle pain, fever, and eosinophilia.
Manifestations gradually resolve by about the 3rd month, when the larvae have become fully encysted, although vague muscular pains and fatigue may persist.
Diagnose using enzyme immunoassay.
Thoroughly cooking meat from pigs and wild animals can prevent trichinosis.






