


Spinal cord disorders can cause permanent severe neurologic disability. For some patients, such disability can be avoided or minimized if evaluation and treatment are rapid.
Anatomy of the Spinal Cord
The spinal cord extends caudally from the medulla at the foramen magnum and terminates at the upper lumbar vertebrae, usually between L1 and L2, where it forms the conus medullaris. In the lumbosacral region, nerve roots from lower cord segments descend within the spinal column in a nearly vertical sheaf, forming the cauda equina.
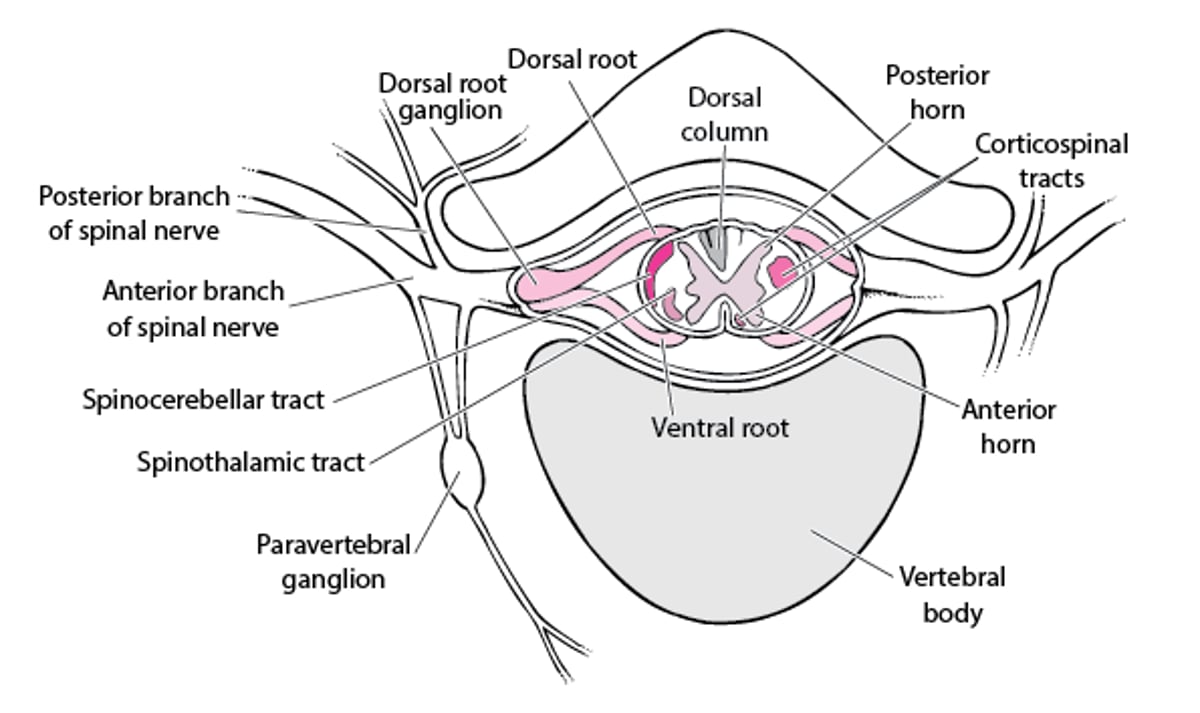
The white matter at the cord’s periphery contains ascending and descending tracts of myelinated sensory and motor nerve fibers. The central H-shaped gray matter is composed of cell bodies and nonmyelinated fibers (see figure Spinal nerve). The anterior (ventral) horns of the “H” contain lower motor neurons, which receive impulses from the motor cortex via the descending corticospinal tracts and, at the local level, from internuncial neurons and afferent fibers from muscle spindles. The axons of the lower motor neurons are the efferent fibers of the spinal nerves. The posterior (dorsal) horns contain sensory fibers that originate in cell bodies in the dorsal root ganglia. The gray matter also contains many internuncial neurons that carry motor, sensory, or reflex impulses from dorsal to ventral nerve roots, from one side of the cord to the other, or from one level of the cord to another.
The spinothalamic tract transmits pain and temperature sensation contralaterally in the spinal cord; most other tracts transmit information ipsilaterally. The cord is divided into functional segments (levels) corresponding approximately to the attachments of the 31 pairs of spinal nerve roots.
Spinal Nerve

Etiology of Spinal Cord Disorders
Spinal cord disorders usually result from conditions extrinsic to the cord, such as the following:
Compression due to spinal stenosis
Less commonly, disorders are intrinsic to the cord. Intrinsic disorders include spinal cord infarction, hemorrhage, transverse myelitis, HIV infection, poliovirus infection, West Nile virus infection, syphilis (which can cause tabes dorsalis), COVID-19, trauma, vitamin B12 deficiency (which causes subacute combined degeneration), decompression sickness, lightning injury (which can cause keraunoparalysis [transient paralysis and sensory deficits with ischemia]), radiation therapy (which can cause myelopathy), syrinx, and spinal cord tumor. Arteriovenous malformations may be extrinsic or intrinsic. may result in myelopathy similar to that caused by vitamin B12 deficiency.
Spinal nerve roots outside of the spinal cord may also be damaged.
Symptoms and Signs of Spinal Cord Disorders
Neurologic dysfunction due to spinal cord disorders occurs at the involved spinal cord segment (see table Motor and Reflex Effects of Spinal Cord Dysfunction by Segmental Level) and at all segments below it. The exception is the central cord syndrome (see table Spinal Cord Syndromes), which may spare segments below.
Spinal cord disorders cause various patterns of deficits depending on which nerve tracts within the cord or which spinal roots outside the cord are damaged. Disorders affecting spinal nerves, but not directly affecting the cord, cause sensory or motor abnormalities or both only in the areas supplied by the affected spinal nerves.
Spinal cord dysfunction causes
Paresis
Loss of sensation
Reflex changes
Autonomic dysfunction (eg, bowel, bladder, and erectile dysfunction; loss of sweating)
Dysfunction may be partial (incomplete). Autonomic and reflex abnormalities are usually the most objective signs of cord dysfunction; sensory abnormalities are the least objective.
Corticospinal tract lesions cause upper motor neuron dysfunction. Acute, severe lesions (eg, infarction, traumatic lesions) cause spinal shock with flaccid paresis (decreased muscle tone, hyporeflexia, and no extensor plantar responses). After days or weeks, upper motor neuron dysfunction evolves into spastic paresis (increased muscle tone, hyperreflexia, and clonus). Extensor plantar responses and autonomic dysfunction are present. Flaccid paresis that lasts more than a few weeks suggests lower motor neuron dysfunction (eg, due to Guillain-Barré syndrome).
Specific cord syndromes include the following (see table Spinal Cord Syndromes):
Transverse myelopathy
Brown-Séquard syndrome
Central cord syndrome
Anterior cord syndrome
Conus medullaris syndrome
Cauda equina syndrome, which involves damage to nerve roots at the caudal end of the cord, is not a spinal cord syndrome. However, it mimics conus medullaris syndrome, causing leg paresis and sensory loss involving the affected nerve roots (often in the saddle area), as well as bladder, bowel, and pudendal dysfunction.
Diagnosis of Spinal Cord Disorders
MRI
Neurologic deficits at segmental levels suggest a spinal cord disorder. Similar deficits, especially if unilateral, may result from nerve root or peripheral nerve disorders, which can usually be differentiated clinically. Level and pattern of spinal cord dysfunction help determine presence and location of a spinal cord lesion but not always type of lesion.
MRI is the most accurate imaging test for spinal cord disorders; MRI shows spinal cord parenchyma, soft-tissue lesions (eg, abscesses, hematomas, tumors, abnormalities involving intervertebral disks), and bone lesions (eg, erosion, severe hypertrophic changes, collapse, fracture, subluxation, tumors).
Myelography with a radiopaque agent followed by CT is used less often. It is not as accurate as MRI and is more invasive but may be more readily available and may be needed for patients who are unable to undergo MRI (eg, due to permanent pacemaker).
Plain x-rays may help detect bone lesions.
Treatment of Spinal Cord Disorders
Treatment of the cause when possible
Prevention of complications
Physical and occupational therapy
If symptoms of a spinal cord disorder (eg, paralysis loss of sensation) occur suddenly, emergency treatment is required.
If possible, the cause is treated or corrected.
Measures to prevent problems due to bed rest are essential if patients are paralyzed or confined to bed.
Extensive loss of body functions can be devastating, causing depression and loss of self-esteem. Formal counseling can help patients cope with loss of function and prepare them for rehabilitation.
Rehabilitation is best provided by an interdisciplinary team (nurses, physical therapist, occupational therapist, social worker, nutritionist, psychologist, counselor); the team also includes the patient and family members.






