



Trisomy 13 is caused by an extra chromosome 13 and causes abnormal forebrain, midface, and eye development; severe intellectual disability; heart defects; and small birth size. Diagnosis is with cytogenetic testing. Treatment is supportive.
(See also Overview of Chromosomal Abnormalities.)
Trisomy 13, also called Patau syndrome, is a chromosomal disorder caused by an extra chromosome 13 and is characterized by severe intellectual disability, multiple congenital anomalies, congenital heart defects, and urogenital anomalies. It is associated with high neonatal mortality; most affected infants die within the first weeks of life (1).
Trisomy 13 occurs in approximately 1.7/10,000 pregnancies (based on data from induced abortion for fetal anomalies, stillbirths, and live births) (2); approximately 80% of cases are complete trisomy 13. Advanced maternal age increases the likelihood, and the extra chromosome is usually maternally derived. Although most cases are due to nondisjunction, extra chromosome 13 material may rarely be present as a result of a translocation.
General references
1. Rasmussen SA, Wong LY, Yang Q, et al: Population-based analyses of mortality in trisomy 13 and trisomy 18. Pediatrics 111(4 Pt 1):777-784, 2003. doi: 10.1542/peds.111.4.777
2. Goel N, Morris JK, Tucker D, et al: Trisomy 13 and 18-Prevalence and mortality-A multi-registry population based analysis. Am J Med Genet A 179(12):2382-2392, 2019. doi: 10.1002/ajmg.a.61365
Symptoms and Signs of Trisomy 13
Infants are usually small for gestational age. Midline anomalies are common and include holoprosencephaly (failure of the forebrain to divide properly), facial anomalies such as cleft lip and cleft palate, microphthalmia, colobomas (fissures) of the iris, and retinal dysplasia. Supraorbital ridges are shallow, and palpebral fissures usually are slanted.
The ears are abnormally shaped and usually low-set. Hearing loss is common. Scalp defects and dermal sinuses are also common. Loose folds of skin often are present over the back of the neck.
A single transverse palmar crease, polydactyly, and hyperconvex narrow fingernails are also common. Approximately 57 to 80% of infants have severe congenital cardiovascular anomalies; dextrocardia is common (1).
Genitals are frequently abnormal in both sexes; cryptorchidism and an abnormal scrotum occur in boys, and a bicornuate uterus occurs in girls.
Apneic spells in early infancy are frequent. Intellectual disability is severe.
Symptoms and signs reference
1. Pierpont ME, Brueckner M, Chung WK, et al. Genetic Basis for Congenital Heart Disease: Revisited: A Scientific Statement From the American Heart Association. Circulation. 2018;138(21):e653-e711. doi:10.1161/CIR.0000000000000606
Diagnosis of Trisomy 13
Cytogenetic testing by karyotyping, fluorescent in situ hybridization (FISH) analysis, and/or chromosomal microarray analysis
(See also Next-generation sequencing technologies.)
Diagnosis of trisomy 13 may be suspected postnatally by appearance or prenatally by abnormalities on ultrasound (eg, intrauterine growth restriction), or by increased risk noted on multiple marker screening or noninvasive prenatal screening (NIPS) using cell-free fetal DNA analysis on a maternal blood sample. Management decisions should not be based only on the NIPS result (1).
Prenatally, confirmation is by cytogenetic testing (karyotyping and/or chromosomal microarray analysis) of samples obtained by chorionic villus sampling or amniocentesis. Postnatally, confirmation is by cytogenetic testing usually of a neonatal blood sample.

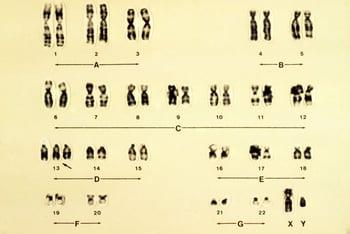
This karyotype represents trisomy 13, which is also known as trisomy D or Patau syndrome (arrow).
Diagnosis reference
1. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics; Committee on Genetics; Society for Maternal-Fetal Medicine: Screening for fetal chromosomal abnormalities: ACOG Practice Bulletin, Number 226. Obstet Gynecol 136(4):e48-e69, 2020. doi: 10.1097/AOG.0000000000004084
Treatment of Trisomy 13
Supportive care
The underlying genetic abnormality cannot be cured.
In carefully selected cases and in alignment with family preferences, ventilatory support, feeding support, and selected surgical procedures (such as cardiac surgery, cleft palate repair, and gastrostomy) may be offered. The focus of treatment is usually palliative care and improving the quality of life for the child and parents. Support for the family is critical.
Prognosis for Trisomy 13
Most infants die during the neonatal period.
Approximately 10% of infants survive beyond the first year of life; however, survival has improved, especially in children who undergo surgical interventions (1).
Prognosis reference
1. Meyer RE, Liu G, Gilboa SM, et al: Survival of children with trisomy 13 and trisomy 18: A multi-state population-based study. Am J Med Genet A 170A(4):825-837, 2016. doi: 10.1002/ajmg.a.37495





